Hospital Infection Control: Preventing Pseudomonas aeruginosa Spread
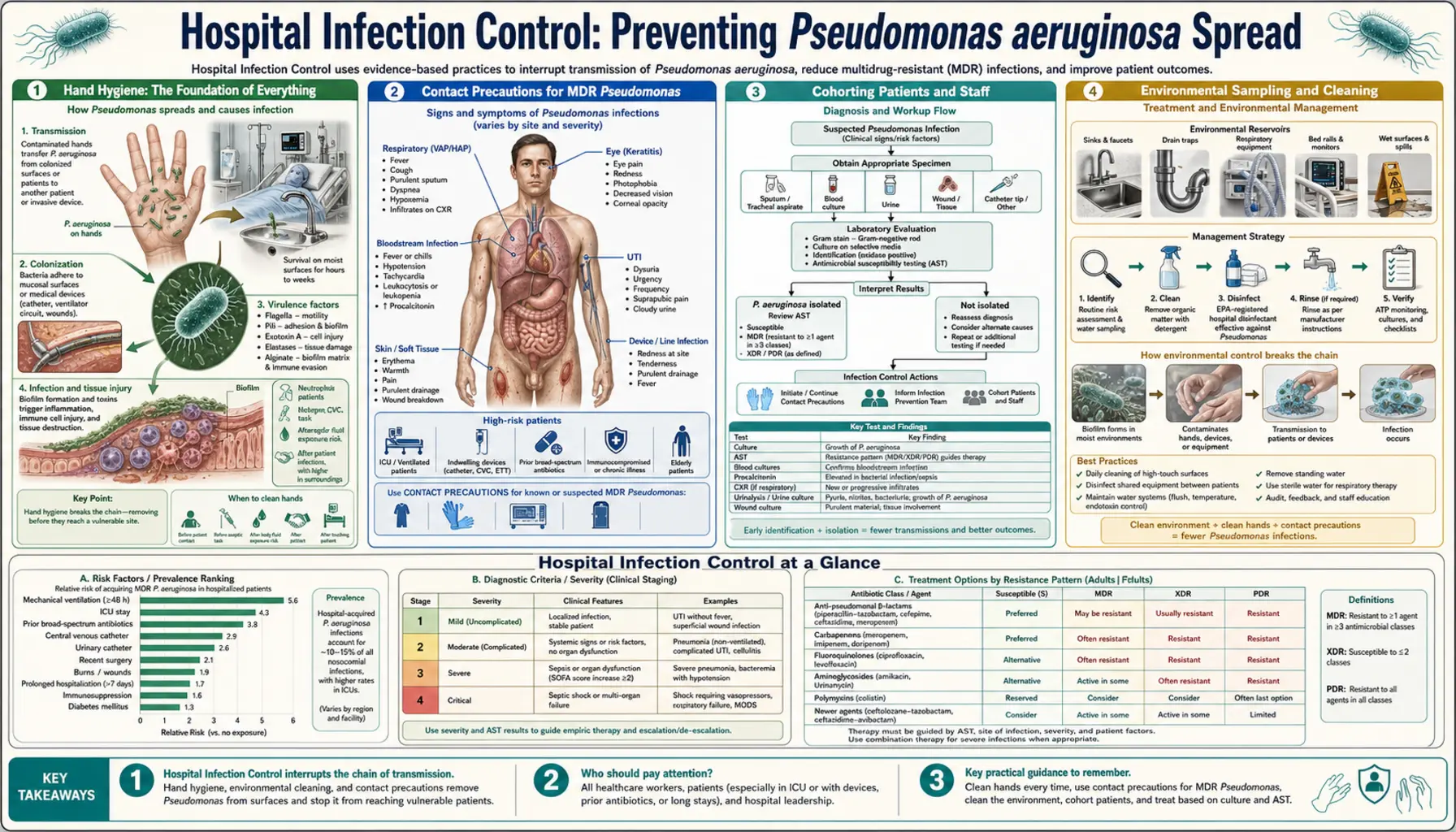
Antibiotic treatment cures individual patients. Infection control prevents the next patient from getting infected. For Pseudomonas aeruginosa — an organism that colonizes hospital water systems, forms persistent biofilms on environmental surfaces, and spreads readily via contaminated hands — a strong hospital infection control program is as important as the antibiotic formulary. This article covers the evidence-based bundle of measures that reduces Pseudomonas transmission in healthcare settings.
Table of Contents
- Hand Hygiene: The Foundation of Everything
- Contact Precautions for MDR Pseudomonas
- Cohorting Patients and Staff
- Environmental Sampling and Cleaning
- Water System Safety: Sinks and Drains as Reservoirs
- VAP Prevention Bundle
- Catheter-Associated UTI Prevention
- Oral Care with Chlorhexidine
- Outbreak Investigation and Response
- Key Research Papers
- Featured Videos
Hand Hygiene: The Foundation of Everything
Hand hygiene is the single most effective measure for preventing healthcare-associated infections of any kind, and P. aeruginosa is no exception. The organism is frequently carried transiently on the hands of healthcare workers who touch colonized patients, contaminated equipment, or environmental surfaces, and is then transmitted to the next patient touched.
Alcohol-based hand rubs (ABHR) are the preferred method for routine hand hygiene in healthcare settings. They are highly effective against P. aeruginosa, faster to use than soap and water, and cause less skin damage with repeated use. Soap and water is required when hands are visibly soiled with organic material or when dealing with spore-forming organisms (Clostridioides difficile), but for Pseudomonas prevention, ABHR is equally effective and more practical.
The WHO "Five Moments for Hand Hygiene" framework identifies the five key situations requiring hand hygiene: (1) before touching a patient; (2) before a clean or aseptic procedure; (3) after exposure to body fluids; (4) after touching a patient; (5) after touching the patient's surroundings. Studies consistently show that compliance with these five moments reduces Pseudomonas and other healthcare-associated infection rates by 20 to 50%.
Barriers to compliance include time pressure, skin irritation from frequent hand hygiene, inadequate access to ABHR dispensers at point of care, and cultural factors. Successful programs combine easy access to ABHR (bedside dispensers at every patient room entry), regular education, leadership role-modeling, and real-time feedback on compliance rates to teams. ( — Search PubMed)
Contact Precautions for MDR Pseudomonas
Patients who are known to be colonized or infected with MDR Pseudomonas aeruginosa — strains resistant to multiple antibiotic classes — should be placed on contact precautions to prevent transmission to other vulnerable patients. Contact precautions consist of a bundle of measures implemented together:
- Single room placement: The patient should ideally be placed in a private room with dedicated bathroom. Single rooms are strongly preferred over curtained bed spaces in shared bays, which provide inadequate physical separation and frequent opportunities for hand contamination on shared surfaces.
- Gloves: Non-sterile examination gloves should be donned before entering the room and removed and disposed of before leaving. Hands must be cleaned with ABHR immediately after glove removal — gloves do not replace hand hygiene and can harbor bacteria on their outer surfaces.
- Gown: A clean non-sterile gown should be worn when entering the room and discarded before leaving. Gowns prevent contamination of the healthcare worker's clothing, which can transfer organisms to the next patient without hand contact.
- Dedicated equipment: Stethoscopes, blood pressure cuffs, and other non-critical patient care items should be dedicated to the patient on contact precautions or thoroughly disinfected between patients.
The duration of contact precautions should be based on microbiological evidence: precautions can be discontinued when serial negative surveillance cultures demonstrate clearance of the organism, though for MDR Pseudomonas in the ICU, many centers maintain precautions for the entire hospitalization. ( — Search PubMed)
Cohorting Patients and Staff
During Pseudomonas outbreaks or periods of heightened transmission, cohorting — grouping together all patients who carry the same organism in a dedicated area of the ward, attended by a dedicated cohort of nursing and medical staff — is a powerful outbreak control measure. The principle is straightforward: if colonized patients and their dedicated staff are physically separated from uncolonized patients, transmission pathways are severed.
Nursing cohorting is the most critical element: nurses who care only for colonized patients cannot inadvertently transmit organisms to uncolonized patients in adjacent beds. Medical cohorting (physicians, physiotherapists, dietitians assigned to the cohort) reduces but does not eliminate transmission risk from other staff categories. Cohorting requires sufficient staffing to implement, which can be challenging during peak outbreak periods or staff shortages.
Active surveillance cultures — systematically swabbing all patients on admission or weekly — are an important adjunct that identifies patients who are colonized but have no clinical infection (and therefore no isolate from clinical cultures). Without active surveillance, colonized patients may be placed in general bays and seed the environment before colonization is recognized. ( — Search PubMed)
Environmental Sampling and Cleaning
P. aeruginosa survives on moist environmental surfaces for extended periods — up to several weeks on wet surfaces and several days on dry surfaces. High-touch surfaces in patient rooms (bed rails, call buttons, door handles, IV pole surfaces, over-bed tables) are frequently contaminated during the care of colonized patients and serve as vectors for transmission via hands.
Effective environmental cleaning protocols include:
- Daily disinfection of all high-touch surfaces in rooms of colonized/infected patients using an EPA-registered hospital-grade disinfectant with proven activity against gram-negative pathogens.
- Terminal cleaning with a disinfectant followed by ultraviolet-C (UV-C) disinfection or hydrogen peroxide vapor when a patient on contact precautions is discharged. These automated no-touch technologies reduce residual organism burden on surfaces missed by manual cleaning.
- Environmental surveillance cultures during outbreak investigations — systematic sampling of sinks, drains, shower heads, respiratory therapy equipment, and ice machines to identify environmental reservoirs of outbreak strains, confirmed by molecular typing against patient isolates.
A key environmental surface deserving special attention is the sink drain. Hospital sink drains harbor complex biofilm communities including P. aeruginosa, which can splash contaminated water droplets onto surfaces up to 1 meter away during routine water use. "Splash-back" contamination from drain biofilms has been documented as a route of healthcare-associated Pseudomonas transmission in multiple studies. Interventions include redesigning sink drains to minimize splash, applying hydrogen peroxide or enzymatic agents to drain biofilms, and physical drain covers. ( — Search PubMed)
Water System Safety: Sinks and Drains as Reservoirs
Hospital water systems are perhaps the most important but least visible reservoir for P. aeruginosa. The organism thrives in biofilms on the interior surfaces of water pipes, taps, shower heads, and hospital equipment connected to the water supply. Standard municipal water treatment and routine hospital chlorination are insufficient to eliminate Pseudomonas from complex biofilm communities in building water infrastructure.
Key water safety interventions include:
- Point-of-use water filters (0.2 micrometer pore size): Installed directly on taps and shower heads in high-risk units (ICU, bone marrow transplant, burn unit, hematology-oncology). These filters remove P. aeruginosa and other microorganisms at the point of patient exposure. Filters require regular replacement (typically every 30 to 62 days) as the membrane loads with organisms and biofilm may form on the upstream side.
- Hot water temperature maintenance: Maintaining hot water above 60°C at the calorifier and above 50°C at the point of delivery inhibits Pseudomonas growth. However, scalding risk must be managed with thermostatic mixing valves.
- Regular flushing of infrequently used outlets: Taps and showers that are rarely used accumulate stagnant water in which Pseudomonas can multiply to very high concentrations before use. A systematic flushing protocol (running the tap for 1 to 2 minutes at least three times per week) prevents stagnation.
- Microbiological surveillance of water outlets: Regular water sampling from high-risk unit outlets to monitor for Pseudomonas contamination, particularly following building work, refurbishment, or periods of reduced water flow.
( — Search PubMed)
VAP Prevention Bundle
Ventilator-associated pneumonia prevention relies on a bundle of interventions applied consistently to every mechanically ventilated patient. Individual measures have modest evidence; their combination in a bundle applied reliably is highly effective:
- Head-of-bed (HOB) elevation to 30–45 degrees: Reduces aspiration of oropharyngeal secretions and gastric content into the lower respiratory tract. Patients must be consistently maintained at 30 to 45 degrees, not positioned flat for procedures and nursing care without returning promptly to the elevated position. ( — Search PubMed)
- Daily sedation awakening trials: Minimizing sedation allows patients to maintain more protective airway reflexes and reduces the duration of mechanical ventilation — the single biggest risk factor for VAP. Daily spontaneous awakening and breathing trials accelerate weaning and extubation.
- Oral care with chlorhexidine: Decontaminating the oropharynx reduces the bacterial load of secretions that pool above the endotracheal tube cuff and are aspirated. A 0.12% chlorhexidine oral rinse applied every 2 to 4 hours reduces VAP incidence by 40% in cardiac surgery patients. Evidence in medical ICU patients is mixed but still supports its use.
- Subglottic secretion drainage (SSD): Specialized endotracheal tubes with a suction port above the cuff allow continuous or intermittent aspiration of the secretion pool above the cuff — the most direct reservoir for lower airway aspiration. Meta-analyses show SSD reduces early VAP incidence by approximately 50%.
- Endotracheal tube cuff pressure management: Maintaining cuff pressure at 20 to 30 cmH₂O minimizes microaspiration through cuff folds while avoiding excessive tracheal mucosal pressure. Automated cuff pressure devices are being investigated to ensure consistent maintenance.
- Minimizing ventilator circuit changes: Frequent ventilator circuit changes paradoxically increase VAP risk by repeatedly introducing the outside environment into the circuit. Current recommendations support changing circuits only when visibly soiled or malfunctioning, not on a scheduled basis.
( — Search PubMed)
Catheter-Associated UTI Prevention
Pseudomonas is one of the leading causes of catheter-associated urinary tract infections (CAUTI). The organism forms biofilms on the surface of urinary catheters rapidly after insertion and is the most common cause of polymicrobial CAUTI. Prevention focuses on:
- Catheter insertion only when indicated: The most effective prevention is avoiding catheter insertion when not strictly necessary. Indications include acute urinary retention, accurate urine output monitoring in critically ill patients, selected perioperative uses, and comfort measures in palliative care. "Convenience" catheterization should never be an indication.
- Daily review and prompt removal: The risk of CAUTI increases approximately 5% per day of catheterization. Nurse-driven protocols for daily catheter review and prompt removal when indications are no longer present significantly reduce CAUTI rates.
- Aseptic insertion technique: Standard sterile technique, including sterile drape, sterile gloves, antiseptic periurethral cleaning, sterile lubricant, and sterile drainage system.
- Closed drainage system maintenance: The drainage bag and tubing must remain a closed system. The drainage bag should be kept below bladder level at all times to prevent reflux. Emptying the drainage bag through the drain valve without contaminating the valve prevents ascending colonization.
( — Search PubMed)
Oral Care with Chlorhexidine
Oral colonization with gram-negative pathogens including P. aeruginosa begins within 24 to 48 hours of ICU admission in most patients. This oropharyngeal colonization serves as the bacterial reservoir for microaspiration and subsequent VAP. Chlorhexidine gluconate oral rinse reduces oropharyngeal gram-negative colonization and has been adopted as a standard ICU nursing practice in most major hospitals.
The standard protocol involves applying 0.12% to 0.2% chlorhexidine gluconate solution or gel to the teeth, gums, tongue, and oral mucosa every 2 to 4 hours using swabs or foam applicators. In intubated patients, the solution is applied around the endotracheal tube entry site and to accessible oral surfaces. Suctioning before and after oral care removes secretion pools above the cuff.
One nuance: some studies have raised concerns about chlorhexidine-associated ventilator-associated events in medical ICU patients — specifically, that its aspiration in large amounts may cause chemical injury. Current evidence supports continued use in cardiac surgery ICU patients, and most authorities continue to recommend it for medical ICU patients given the overall reduction in VAP rates. ( — Search PubMed)
Outbreak Investigation and Response
A cluster of P. aeruginosa cases with similar antibiotic resistance patterns in a ward or unit should trigger a systematic outbreak investigation. The key steps:
- Case definition and cluster confirmation: Define cases by organism, time period, and location. Confirm that the cases represent a true cluster by reviewing background baseline rates for Pseudomonas in the affected unit.
- Molecular typing: Send all isolates from cases to a reference laboratory for PFGE or WGS to determine whether they are clonally related. Non-related isolates (diverse PFGE/WGS patterns) indicate multiple independent acquisitions from the environment rather than person-to-person transmission.
- Environmental sampling: If isolates are clonally related, systematically culture potential environmental sources: all water outlets in the affected area, respiratory therapy equipment, ice machines, humidifiers, any pooled liquids. Match environmental isolates to patient isolates by molecular typing.
- Retrospective contact tracing: Identify all patients who shared the space with confirmed cases or who might have had exposure to the identified environmental source.
- Implement enhanced control measures: Depending on findings — enhanced environmental cleaning, point-of-use water filters, decommissioning of contaminated equipment, increased surveillance cultures, enhanced hand hygiene monitoring.
- Continue surveillance until outbreak is over: Define clear criteria for declaring the outbreak over — typically no new cases for two consecutive incubation periods with confirmed enhanced controls in place.
( — Search PubMed)
Key Research Papers
- WHO. WHO Guidelines on Hand Hygiene in Health Care. Geneva: World Health Organization; 2009. — Search PubMed
- Siegel JD, et al. 2007 Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Healthcare Settings. Am J Infect Control. 2007;35(10 Suppl 2):S65–164. — Search PubMed
- Friedman ND, Kaye KS, Stout JE, et al. Health care-associated bloodstream infections in adults. Ann Intern Med. 2002;137(10):791–797. — Search PubMed
- Hota S, et al. Outbreak of carbapenem-resistant Pseudomonas aeruginosa traced to a contaminated sink drain. Infect Control Hosp Epidemiol. 2009;30(9):834–839. — Search PubMed
- Caporali A, et al. International collaborative study on the epidemiology of carbapenem non-susceptible Pseudomonas aeruginosa. Eur J Clin Microbiol Infect Dis. 2012;31(6):1139–1148. — Search PubMed
- Kallet RH. Evidence-based management of acute lung injury and ARDS. Respir Care. 2004;49(7):793–809. — Search PubMed
- Muscedere J, et al. Comprehensive evidence-based clinical practice guidelines for ventilator-associated pneumonia: prevention. J Crit Care. 2008;23(1):126–137. — Search PubMed
- Kalil AC, et al. Management of adults with hospital-acquired and ventilator-associated pneumonia. Clin Infect Dis. 2016;63(5):e61–e111. — Search PubMed
- Klompas M, et al. Strategies to prevent ventilator-associated pneumonia in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol. 2014;35(8):915–936. — Search PubMed
- Drevinek P, et al. Whole-genome sequencing as a direct diagnostic tool in a nosocomial cluster of Pseudomonas aeruginosa. J Clin Microbiol. 2018;56(12):e01198-18. — Search PubMed
Connections
- All Bacteria
- Pseudomonas aeruginosa (main page)
- Treatments Overview
- Antibiotic Treatment
- Drug Resistance & Novel Therapies
- Burn & ICU Infections
- Staph: Decolonization & Control
- Sepsis
- Pneumonia