Antipseudomonal Antibiotics and Combination Therapy
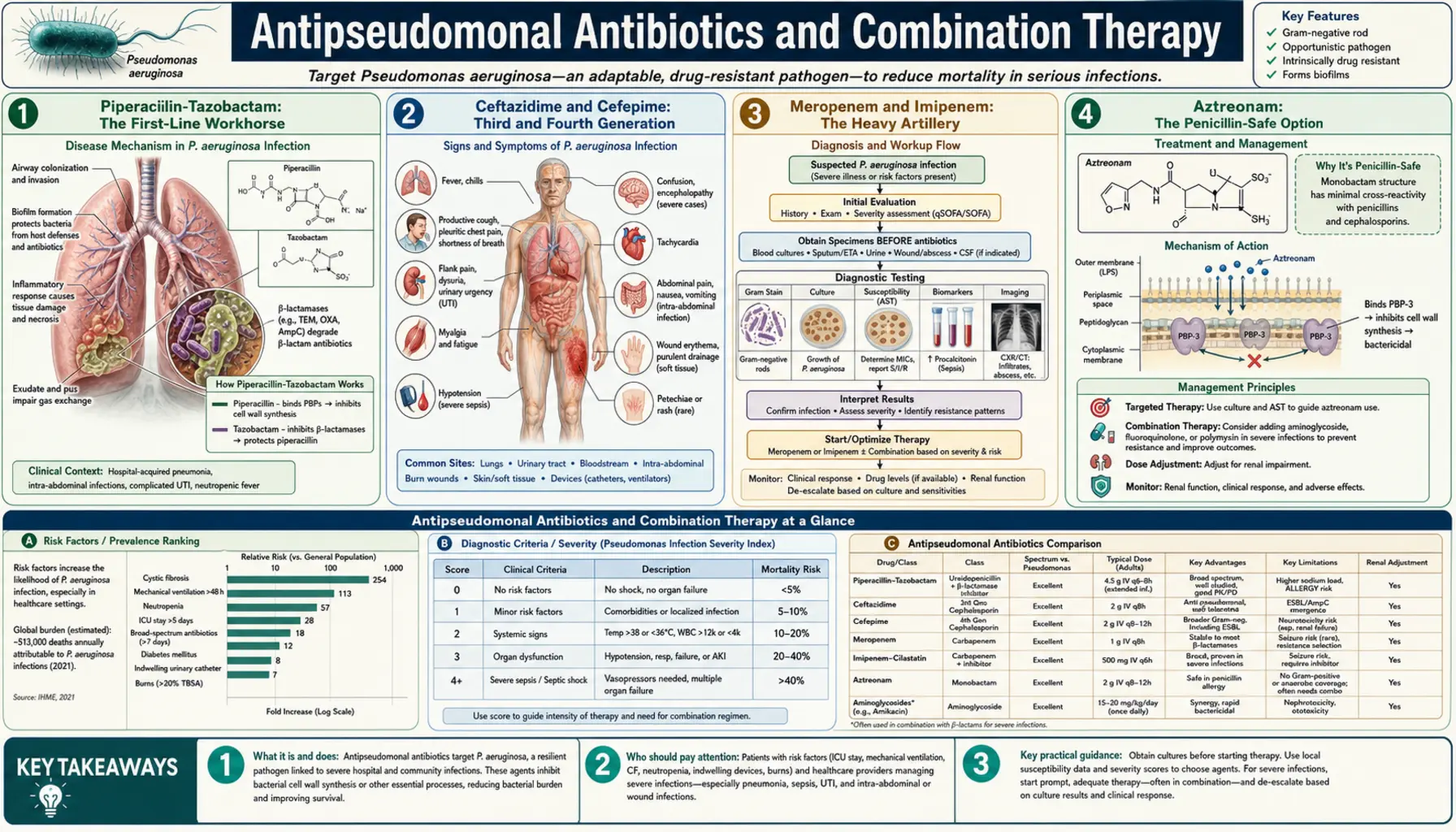
When a Pseudomonas aeruginosa infection is confirmed or strongly suspected, the antibiotic choice determines whether the patient survives. P. aeruginosa is resistant to most antibiotics by default, and the window of active drugs is narrow. This article explains each major antibiotic class used against Pseudomonas, the evidence for combination therapy, the role of inhaled antibiotics, and the key pharmacokinetic principles that separate adequate from inadequate dosing.
Table of Contents
- Piperacillin-Tazobactam: The First-Line Workhorse
- Ceftazidime and Cefepime: Third and Fourth Generation
- Meropenem and Imipenem: The Heavy Artillery
- Aztreonam: The Penicillin-Safe Option
- Tobramycin and Amikacin: Concentration-Dependent Killers
- Ciprofloxacin: Oral Step-Down and Risks
- The Combination Therapy Evidence: MERINO Trial and Beyond
- Inhaled Tobramycin and Aztreonam for CF and VAP
- Anti-Biofilm: Tobramycin Plus Ciprofloxacin Synergy
- Key Research Papers
- Featured Videos
Piperacillin-Tazobactam: The First-Line Workhorse
Piperacillin-tazobactam (pip-tazo, trade name Zosyn in the US) is the most widely used empiric antibiotic for hospital-acquired infections where P. aeruginosa is a concern. It combines piperacillin — an extended-spectrum penicillin with inherent activity against Pseudomonas — with tazobactam, a beta-lactamase inhibitor that prevents destruction of the piperacillin molecule by many beta-lactamase enzymes produced by bacteria.
Piperacillin works by binding penicillin-binding proteins (PBPs) in the bacterial cell wall, inhibiting the cross-linking of peptidoglycan strands and causing cell lysis. It is bactericidal and time-dependent: efficacy correlates with the proportion of the dosing interval during which drug concentration exceeds the minimum inhibitory concentration (MIC) — ideally above the MIC for 50% to 60% of the interval.
Standard dosing is 3.375 g or 4.5 g every 6 to 8 hours by intravenous infusion. For serious Pseudomonas infections, extended infusion — infusing the same dose over 4 hours instead of 30 minutes — achieves significantly better pharmacokinetic targets and has been associated with improved clinical outcomes in retrospective studies. ( — Search PubMed)
A major limitation: tazobactam does not inhibit AmpC beta-lactamases or metallo-beta-lactamases. Strains that have derepressed their chromosomal AmpC — increasingly common in patients who have received prior beta-lactam therapy — are resistant to pip-tazo. This is why susceptibility testing of each individual isolate is mandatory.
Ceftazidime and Cefepime: Third and Fourth Generation
Ceftazidime is a third-generation cephalosporin with excellent activity against P. aeruginosa. It was the first broad-spectrum cephalosporin with reliable antipseudomonal activity and remains widely used, particularly in combination with aminoglycosides for serious infections. Standard IV dosing is 1 to 2 g every 8 hours; extended infusion (over 3 to 4 hours) improves pharmacodynamic target attainment for strains with higher MICs.
Ceftazidime's limitation is its susceptibility to AmpC beta-lactamases. When bacteria derepress their chromosomal AmpC during treatment — which occurs in 10 to 40% of patients with serious Pseudomonas infections receiving ceftazidime — clinical failure results despite initial in vitro susceptibility. This selection of AmpC-derepressed mutants during therapy is called "inducible AmpC resistance" and is an important cause of clinical treatment failure. ( — Search PubMed)
Cefepime is a fourth-generation cephalosporin with enhanced stability against AmpC beta-lactamases compared to ceftazidime, making it a preferred option for organisms with suspected or documented AmpC derepression. It also has broader activity against gram-positive organisms. Dosing is 1 to 2 g every 8 to 12 hours IV, with extended infusion for serious infections. Cefepime at high doses in patients with renal impairment can cause neurotoxicity (encephalopathy, seizures), requiring dose adjustment and careful monitoring in critically ill patients.
Meropenem and Imipenem: The Heavy Artillery
Carbapenems are the most broad-spectrum beta-lactam antibiotics available and are reserved for serious infections, particularly when MDR organisms are suspected or confirmed. For Pseudomonas specifically:
Meropenem is the preferred carbapenem for serious Pseudomonas infections. It has lower seizure potential than imipenem at high doses, is more stable against AmpC beta-lactamases, and achieves better CNS penetration for meningitis. Standard dosing is 1 to 2 g every 8 hours by IV infusion; for MDR isolates with MIC values up to 4 mg/L, high-dose extended-infusion meropenem (2 g over 3 hours every 8 hours) significantly improves pharmacodynamic target attainment.
Imipenem-cilastatin is equally active against susceptible Pseudomonas and was historically the gold standard for serious gram-negative infections. Cilastatin blocks renal inactivation of imipenem, allowing higher urinary concentrations. The main limitation for Pseudomonas is a higher propensity to select for OprD porin loss — the primary mechanism of imipenem resistance in P. aeruginosa. Imipenem is not reliably active against strains that have lost OprD, even when MIC values are at the susceptible breakpoint.
Carbapenem resistance in P. aeruginosa is mediated by multiple mechanisms and carries an extremely limited treatment landscape. Full discussion: Drug Resistance and Novel Therapies. ( — Search PubMed)
Aztreonam: The Penicillin-Safe Option
Aztreonam is a monobactam — the only antibiotic in its class — with activity exclusively against gram-negative aerobic bacteria, including most P. aeruginosa. Its mechanism is the same as other beta-lactams (PBP inhibition), but its unique monocyclic structure means it does not cross-react with penicillin or cephalosporin antibodies. It is therefore safe to use in patients with documented severe penicillin or cephalosporin allergy.
IV aztreonam is dosed at 1 to 2 g every 6 to 8 hours for serious infections. Like other beta-lactams, extended infusion (over 3 to 4 hours) improves pharmacodynamic target attainment. Aztreonam is susceptible to metallo-beta-lactamases (MBLs) but stable against most serine carbapenemases.
Inhaled aztreonam lysinate (AZLI, brand name Cayston) is formulated specifically for inhalation in CF patients with chronic Pseudomonas lung disease, providing airway drug concentrations far exceeding achievable IV concentrations. AZLI is used in 28-day alternating cycles and has demonstrated improvement in FEV1 and quality of life compared to placebo. ( — Search PubMed)
Tobramycin and Amikacin: Concentration-Dependent Killers
Aminoglycoside antibiotics inhibit bacterial protein synthesis by binding the 30S ribosomal subunit and causing misreading of the genetic code. Unlike beta-lactams, aminoglycosides are concentration-dependent: efficacy correlates with the peak drug concentration relative to the MIC (Cmax/MIC ratio), ideally above 8:1 to 10:1. This pharmacokinetic property means aminoglycosides are most effective given as large, infrequent doses — typically once daily — rather than divided smaller doses.
Tobramycin is the preferred aminoglycoside for Pseudomonas infections. It is slightly more active than gentamicin against Pseudomonas and less nephrotoxic than gentamicin at equivalent doses. Standard once-daily dosing: 5 to 7 mg/kg IV every 24 hours, with adjustment for renal function. Therapeutic drug monitoring with peak (1 hour post-infusion) and trough (just before next dose) levels is essential to optimize efficacy and minimize nephrotoxicity and ototoxicity.
Amikacin is resistant to most aminoglycoside-modifying enzymes (AMEs) — bacterial enzymes that inactivate tobramycin and gentamicin. For tobramycin-resistant P. aeruginosa where the mechanism is AME-mediated, amikacin often retains activity. Dosing: 15 to 20 mg/kg once daily IV.
Inhaled tobramycin (TOBI) for CF: 300 mg via nebulizer or 112 mg via dry powder inhaler, twice daily in alternating 28-day on/off cycles. Inhaled delivery achieves sputum concentrations >1,000 mg/L — far exceeding the MIC of even resistant strains — while minimizing systemic exposure and toxicity. ( — Search PubMed)
Ciprofloxacin: Oral Step-Down and Risks
Ciprofloxacin inhibits DNA gyrase and topoisomerase IV, enzymes required for bacterial DNA replication and repair. It is the most active fluoroquinolone against P. aeruginosa and has the critical advantage of excellent oral bioavailability — oral ciprofloxacin achieves blood concentrations nearly identical to IV administration, making it the only oral antibiotic option for serious Pseudomonas infections in stable patients.
Despite this advantage, fluoroquinolone use against Pseudomonas must be judicious. Resistance develops through stepwise mutations in DNA gyrase (gyrA, gyrB) and topoisomerase (parC, parE) genes, combined with upregulation of efflux pumps. These mutations can emerge during treatment — ciprofloxacin monotherapy for serious Pseudomonas infections carries a 10 to 30% risk of resistance emergence during the treatment course. Fluoroquinolone resistance rates in P. aeruginosa clinical isolates have risen dramatically over the past two decades and now exceed 30% in many hospitals. ( — Search PubMed)
Clinical uses where ciprofloxacin remains appropriate: oral step-down therapy for susceptible UTIs and some susceptible lower respiratory tract infections in stable outpatients; part of combination regimens for susceptible isolates; oral suppression of chronic Pseudomonas infections in some CF patients (recognizing resistance emergence risk).
The Combination Therapy Evidence: MERINO Trial and Beyond
Combination antibiotic therapy for serious gram-negative bacteremia — using two agents simultaneously — has been debated for decades. The MERINO trial, a landmark randomized controlled trial published in 2018, addressed the specific question of piperacillin-tazobactam versus meropenem for gram-negative bacteremia, including Pseudomonas. The trial showed that pip-tazo was inferior to meropenem for treatment of bloodstream infections caused by extended-spectrum beta-lactamase (ESBL)-producing organisms and resistant gram-negatives — specifically, 30-day mortality was significantly higher in the pip-tazo arm. This finding reinforced carbapenem use as the treatment of choice when resistant gram-negatives are confirmed. ( — Search PubMed)
For the specific question of combination versus monotherapy in Pseudomonas bacteremia, multiple meta-analyses have shown no consistent mortality benefit of combination therapy over appropriate monotherapy in non-neutropenic patients. However, combination therapy does provide significantly better empiric coverage — ensuring at least one active agent is present before susceptibility results are available — and is most justified in:
- Neutropenic fever with suspected gram-negative bacteremia
- Septic shock where inadequate empiric therapy substantially increases mortality
- Hospitals or patient populations with high rates of MDR Pseudomonas
- Documented MDR isolates where synergistic combinations may be the only viable option
( — Search PubMed)
Inhaled Tobramycin and Aztreonam for CF and VAP
Inhaled antibiotics represent a fundamentally different approach to treating Pseudomonas lung infections: delivering drug directly to the site of infection at concentrations that cannot be achieved by systemic routes. The pharmacological rationale is compelling — the thick, oxygen-depleted, biofilm-containing mucus of CF airways and the endotracheal tube biofilm of ventilated patients are poorly reached by systemically administered drugs.
For CF, the clinical evidence supporting inhaled tobramycin and inhaled aztreonam lysinate is robust and practice-defining. Both agents are recommended in CF foundation guidelines as maintenance suppressive therapy for chronically infected patients. The alternating 28-day cycle approach delays resistance emergence and allows some normalization of microbiome between courses. In practice, many CF centers use TOBI and AZLI in rotation to provide year-round suppressive coverage.
For VAP, inhaled adjunctive antibiotics (inhaled tobramycin or inhaled colistin added to systemic therapy) are being evaluated in clinical trials. Early results suggest potential benefit in reducing the duration of systemic antibiotic therapy and improving microbiological outcomes in ventilated patients with Pseudomonas VAP, but the evidence is not yet definitive enough to make this standard of care. ( — Search PubMed)
Anti-Biofilm: Tobramycin Plus Ciprofloxacin Synergy
Standard antibiotic therapy targets planktonic (free-floating) bacteria, but the most clinically challenging Pseudomonas infections — CF lung disease, catheter-associated infections, chronic wounds — are biofilm infections. Within biofilms, bacteria are 10 to 1,000 times more tolerant of antibiotics, making conventional susceptibility-guided therapy inadequate.
Laboratory studies have identified the combination of tobramycin plus ciprofloxacin as having synergistic activity against P. aeruginosa biofilms specifically. The mechanism appears to involve tobramycin disrupting the outer membrane of biofilm-embedded cells (despite poor overall penetration), creating increased access for ciprofloxacin to reach its intracellular DNA gyrase targets. This combination achieves greater biofilm killing than either drug alone at equivalent concentrations. ( — Search PubMed)
In CF clinical practice, oral ciprofloxacin is often combined with inhaled tobramycin during acute pulmonary exacerbations as a partially oral regimen in patients who are not sick enough to require hospitalization but too unwell to wait for IV therapy. The evidence base for this approach is empirical rather than rigorously controlled, but it reflects the clinical reality that biofilm disruption requires multiple mechanisms acting simultaneously.
Key Research Papers
- Lodise TP, et al. Extended-infusion piperacillin-tazobactam for Pseudomonas aeruginosa: clinical outcomes. Antimicrob Agents Chemother. 2007;51(10):3674–3680. — Search PubMed
- Bush K, Jacoby GA. Updated functional classification of beta-lactamases. Antimicrob Agents Chemother. 2010;54(3):969–976. — Search PubMed
- Mouton JW, et al. Role of pharmacokinetics/pharmacodynamics in the fight against resistance. Int J Antimicrob Agents. 2018;52(6):715–721. — Search PubMed
- Oermann CM, et al. An 18-month study of the safety and efficacy of repeated courses of inhaled aztreonam lysine in CF. Pediatr Pulmonol. 2010;45(11):1121–1134. — Search PubMed
- Ramsey BW, et al. Intermittent administration of inhaled tobramycin in patients with cystic fibrosis. N Engl J Med. 1999;340(1):23–30. — Search PubMed
- Vardakas KZ, et al. Fluoroquinolones in the treatment of nosocomial pneumonia. Clin Microbiol Infect. 2009;15(9):803–813. — Search PubMed
- Harris PNA, et al. Effect of piperacillin-tazobactam vs meropenem on 30-day mortality for patients with E. coli or Klebsiella pneumoniae bloodstream infection and ceftriaxone resistance: a randomized clinical trial (MERINO). JAMA. 2018;320(10):984–994. — Search PubMed
- Paul M, et al. Beta-lactam antibiotic monotherapy versus beta-lactam-aminoglycoside combination therapy for sepsis. Cochrane Database Syst Rev. 2014;(1):CD003344. — Search PubMed
- Palmer LB, et al. Aerosolized antibiotics in the ICU: the evidence. Clin Chest Med. 2011;32(3):547–554. — Search PubMed
- Donaldson SH, et al. Mucus clearance and lung function in cystic fibrosis with hypertonic saline. N Engl J Med. 2006;354(3):241–250. — Search PubMed
Connections
- All Bacteria
- Pseudomonas aeruginosa (main page)
- Treatments Overview
- Infection Control
- Drug Resistance & Novel Therapies
- CF Lung Infections
- Sepsis
- Pneumonia
- MRSA Treatment