Pseudomonas aeruginosa in Burn Wounds and ICU Infections
Burn injuries and intensive care settings bring patients face to face with one of the most dangerous hospital pathogens in existence. Pseudomonas aeruginosa has evolved specifically to thrive in wounded tissue, hospital equipment, and the weakened immune environments of critically ill patients. Understanding how it attacks, what the warning signs look like, and what can be done to prevent and treat these infections is critical knowledge for patients, families, and healthcare providers.
Table of Contents
- Why Burns Are a Perfect Target for Pseudomonas
- From Colonization to Invasion: How Burn Infections Progress
- Pyocyanin and the Green-Black Eschar
- Burn Wound Bacteremia and Sepsis
- Ventilator-Associated Pneumonia in the ICU
- Hot Tub Folliculitis: The Community Setting
- Swimmer's Ear and Malignant Otitis Externa
- Diabetic Foot Ulcers and Chronic Wounds
- Topical Wound Management Strategies
- Key Research Papers
- Featured Videos
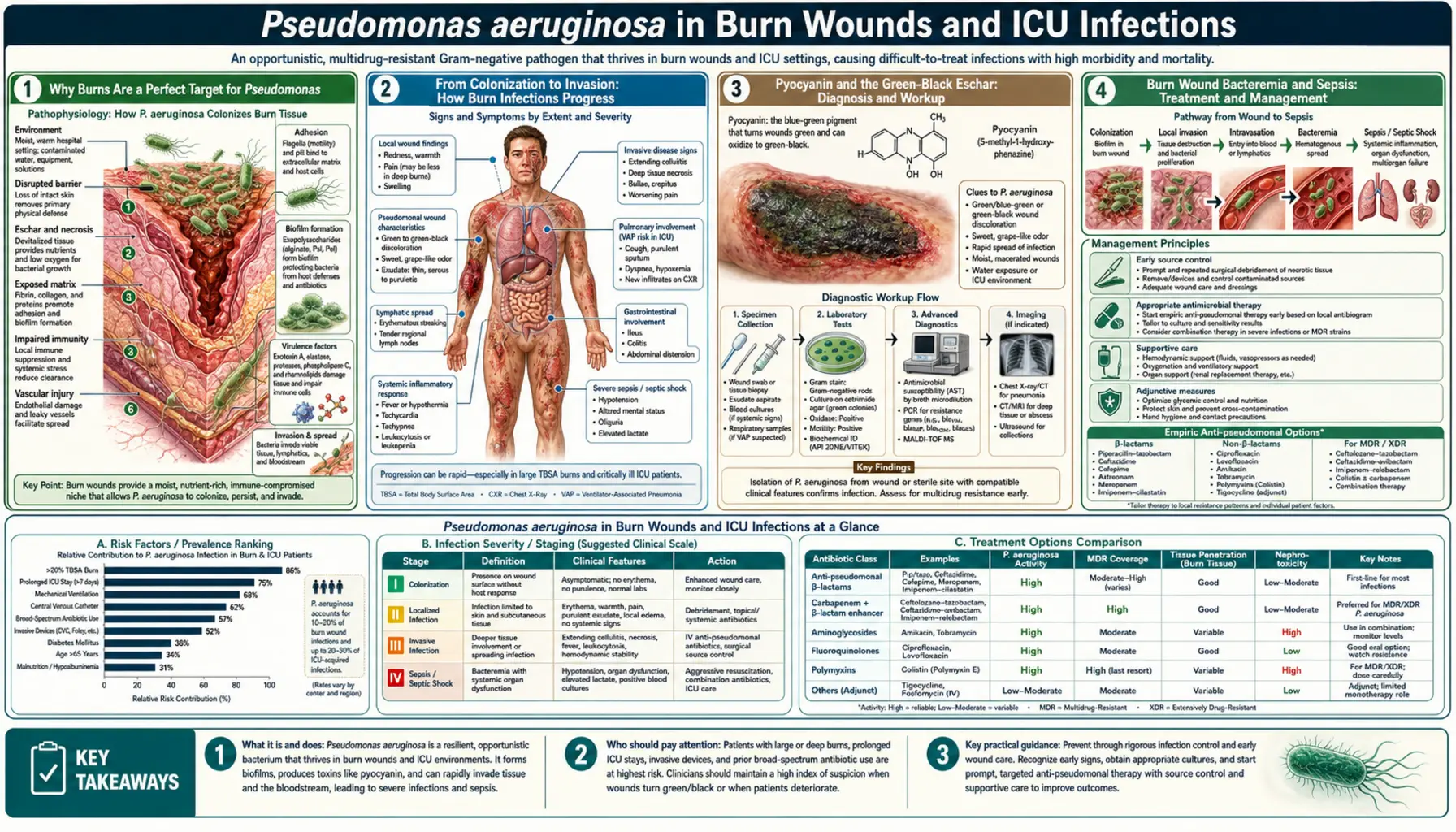
Why Burns Are a Perfect Target for Pseudomonas
A burn wound is, from a microbiological perspective, a nutrient-rich, protein-filled, avascular environment. Blood vessels in burned tissue are destroyed or occluded, which means that both the immune system's cellular defenders (neutrophils, macrophages) and any antibiotics administered intravenously cannot reach the wound in adequate concentrations. The dead tissue — called eschar — provides abundant protein and carbohydrate for bacterial growth with essentially no host defenses to counter it.
P. aeruginosa is particularly well adapted to this environment for several reasons. It can grow across a wide temperature range (4–42°C), can use an enormous variety of organic compounds as food, and can form biofilms on almost any surface, including necrotic tissue. It also survives in the moist, warm microenvironment of a burn unit better than most organisms, persisting on sink surfaces, wound dressings, hydrotherapy equipment, and the hands of healthcare workers.
The organism's ubiquity in hospital environments combined with the vulnerability of burn patients creates a very high-risk intersection. Burn wound colonization with P. aeruginosa typically occurs within 48 to 72 hours of injury, regardless of antibiotic prophylaxis. The clinical question is always whether colonization will remain superficial or progress to invasive infection. ( — Search PubMed)
From Colonization to Invasion: How Burn Infections Progress
The natural history of Pseudomonas burn wound infection moves through identifiable stages:
- Surface colonization: The burn eschar surface is colonized but organisms have not penetrated into the viable tissue beneath. Wound swab cultures will be positive, but there are no systemic signs of infection. This stage is inevitable and expected.
- Deep colonization: Organisms penetrate into the deeper layers of the eschar and necrotic tissue but have not reached the viable dermis. Wound biopsy quantitative cultures typically show 10,000 to 100,000 colony-forming units per gram of tissue — below the threshold of invasive infection but concerning.
- Invasive infection: When quantitative cultures exceed 100,000 (10⁵) CFU per gram, organisms have penetrated the eschar-viable tissue interface and are actively invading living tissue. This is burn wound infection in the true clinical sense. Histological examination of wound biopsies shows organisms invading viable dermis and subcutaneous tissue. Systemic signs typically appear: fever or hypothermia, tachycardia, and evidence of hemodynamic instability.
- Septicemia: Organisms enter the bloodstream from the wound, leading to Pseudomonas bacteremia and, in severe cases, septic shock with multi-organ failure. This is the most life-threatening stage.
The risk of progression from colonization to invasive infection depends on multiple factors: burn size (larger burns confer higher risk), burn depth (full-thickness burns are more susceptible), patient age and immune status, time elapsed since injury, antibiotic pressure (which can select for resistant organisms), and the virulence characteristics of the colonizing strain. ( — Search PubMed)
Pyocyanin and the Green-Black Eschar
One of the earliest and most visible signs of Pseudomonas colonization in a burn wound is a change in wound color. As the organism grows and produces its characteristic blue-green pigment pyocyanin, wound dressings and the eschar surface develop a blue-green to green-gray coloration. This color change was noted as long ago as the American Civil War, when surgical dressings stained blue-green by Pseudomonas were observed in field hospitals — and paradoxically, soldiers with this "blue pus" sometimes seemed to heal better, because the antibacterial compounds produced by Pseudomonas were killing other, more immediately dangerous wound pathogens like Staphylococcus aureus.
Modern understanding is more nuanced. Pyocyanin is a potent virulence factor that generates reactive oxygen species within host cells, disrupts mitochondrial electron transport, depletes the antioxidant glutathione, inactivates the host enzyme catalase, and suppresses neutrophil function by inducing apoptosis. It also impairs the beating of respiratory cilia, which is relevant in patients who develop Pseudomonas pneumonia superimposed on burn injury.
As invasive infection develops, the wound may develop a characteristic black discoloration — ecthyma gangrenosum of the wound — reflecting ischemic necrosis caused by bacterial invasion of blood vessel walls. The organism produces proteases (LasB elastase) that degrade the structural proteins holding blood vessel walls together, causing local vascular thrombosis and tissue death. The development of new black eschar in a previously stable wound is an important clinical warning sign. ( — Search PubMed)
Burn Wound Bacteremia and Sepsis
When P. aeruginosa invades beyond the wound and enters the bloodstream, the patient enters a critical phase. Pseudomonas bacteremia in burn patients carries mortality rates that historically exceeded 50% and remain very high despite modern critical care. The clinical presentation is that of gram-negative bacteremia: high fever or hypothermia, rigors, tachycardia, hypotension, and evidence of end-organ dysfunction (rising creatinine, altered mental status, liver enzyme elevation).
The skin lesions of Pseudomonas bacteremia — ecthyma gangrenosum — may appear at sites distant from the original burn wound, on unburned skin. These hemorrhagic, black-centered ulcers represent bacterial invasion of blood vessel walls at any site the organism seeds during bacteremia. Their appearance in a burn patient is a marker of systemic dissemination and a medical emergency requiring immediate blood cultures and empiric antipseudomonal therapy.
Exotoxin A produced by P. aeruginosa during bacteremia contributes to the severity of septic shock. This toxin, the most potent virulence factor of the organism, inactivates the host protein synthesis machinery (elongation factor 2), causing widespread cell death in multiple organs. High serum concentrations of anti-exotoxin A antibodies in burn patients correlate with improved survival, and this observation has driven interest in passive immunization strategies. ( — Search PubMed)
Ventilator-Associated Pneumonia in the ICU
Ventilator-associated pneumonia (VAP) is defined as pneumonia developing more than 48 hours after endotracheal intubation. P. aeruginosa is consistently among the top two or three pathogens in VAP, accounting for 15 to 25% of cases in most series. The mortality of Pseudomonas VAP is consistently higher than VAP caused by other organisms, ranging from 30 to 70% in published studies.
Several mechanisms explain why mechanically ventilated patients are so vulnerable:
- The endotracheal tube bypasses upper airway defenses (nose, larynx, gag reflex) and provides a direct conduit from the environment to the lower respiratory tract.
- P. aeruginosa forms biofilms on the inner surface of the endotracheal tube within hours of intubation. These biofilms shed bacterial emboli with each ventilator breath, continuously inoculating the lower airway.
- Sedation and analgesia impair cough, the primary mechanical defense for clearing the lower airways.
- Aspiration of oropharyngeal secretions pooled above the endotracheal tube cuff is a major route of inoculation. ICU patients are colonized in the oropharynx with gram-negative organisms within 24 to 48 hours of admission.
- Critically ill patients have globally impaired immune function due to the combined effects of their underlying illness, surgical stress, malnutrition, hyperglycemia, and the immunosuppressive effects of some medications.
Clinical diagnosis of VAP is challenging. The classic criteria — new or worsening pulmonary infiltrate, fever, leukocytosis, and purulent sputum — lack specificity in ICU patients, who may have pulmonary infiltrates from many non-infectious causes. Quantitative bronchoalveolar lavage cultures with a threshold of 10,000 CFU/mL are the diagnostic gold standard. ( — Search PubMed)
Hot Tub Folliculitis: The Community Setting
Hot tub folliculitis is the most common Pseudomonas infection affecting otherwise healthy people. It occurs when people are exposed to hot tubs, swimming pools, water parks, or even contaminated homemade water slides where chlorination is inadequate. Hot water depletes chlorine 3 to 4 times faster than cold water, meaning hot tubs require more frequent monitoring and chlorine addition than pools.
The infection begins when P. aeruginosa growing in the water penetrates hair follicles, particularly in areas covered by a swimsuit (which keeps contaminated water in close contact with skin for extended periods). Symptoms begin 8 to 48 hours after exposure: an itchy, red rash of small papules and pustules centered on hair follicles, predominantly on the trunk, buttocks, and areas under the swimsuit. The palms and soles are typically spared.
Hot tub folliculitis is self-limiting in healthy people and resolves without antibiotics within 7 to 10 days. Symptomatic relief with topical antiseptics or mild topical antibiotic preparations is reasonable. The key management point is prevention: owners and managers of hot tubs must maintain proper water chemistry (pH 7.2–7.8, free chlorine above 3 mg/L), test the water regularly, and avoid overcrowding that rapidly depletes chlorine. ( — Search PubMed)
Swimmer's Ear and Malignant Otitis Externa
Otitis externa (swimmer's ear) is the most common clinical presentation of P. aeruginosa in immunocompetent patients. The external ear canal is normally protected by its acidic pH (maintained by cerumen), its waxy, hydrophobic environment, and a thin layer of mucus with antimicrobial peptides. Prolonged water exposure disrupts all of these protective factors: it raises pH, washes out cerumen, and creates a moist environment conducive to bacterial growth.
Classic otitis externa presents with ear pain that worsens with movement of the tragus (the small cartilage in front of the ear canal) or pinna, itching, and sometimes a clear or slightly cloudy discharge. The canal is red and edematous. Most cases respond promptly to topical antibiotic-steroid combinations (ciprofloxacin-dexamethasone or polymyxin B-neomycin-hydrocortisone otic drops).
Malignant (necrotizing) otitis externa is an entirely different disease. It occurs almost exclusively in elderly diabetic patients or those with severe immunocompromise. P. aeruginosa invades through the floor of the external auditory canal into cartilage, bone, and the soft tissue of the skull base. The hallmarks are severe, constant pain disproportionate to the visible ear inflammation, granulation tissue at the bony-cartilaginous junction of the external canal, and progressive cranial nerve palsies (facial nerve is most commonly affected, but lower cranial nerves can be involved). Radiographic imaging (CT and MRI) shows skull base erosion. Treatment requires prolonged intravenous antipseudomonal antibiotics, often for 6 to 8 weeks, and mortality remains significant. ( — Search PubMed)
Diabetic Foot Ulcers and Chronic Wounds
Diabetic foot ulcers and other chronic wounds (venous leg ulcers, pressure injuries) are frequently colonized with P. aeruginosa, which is detected in approximately 25 to 50% of chronic wound samples using molecular culture methods. The combination of peripheral neuropathy (loss of protective sensation), peripheral vascular disease (impaired blood flow), and hyperglycemia (impairs neutrophil function and facilitates bacterial growth) makes diabetic patients particularly susceptible.
P. aeruginosa in chronic wounds forms polymicrobial biofilms in community with other organisms such as Staphylococcus aureus, anaerobes, and streptococci. The presence of P. aeruginosa in a diabetic foot ulcer is associated with delayed wound healing, increased wound depth, and higher rates of amputation. The organism produces enzymes (elastase, protease, pyocyanin) that directly damage wound tissue and impair the normal wound healing cascade. ( — Search PubMed)
Management of Pseudomonas-infected diabetic foot ulcers requires aggressive wound debridement to remove the biofilm physically, appropriate systemic antibiotics guided by susceptibility testing, and optimization of blood glucose control. Topical agents with anti-Pseudomonal activity, including silver-containing dressings and medical-grade honey preparations, have evidence supporting their use as adjuncts to systemic therapy.
Topical Wound Management Strategies
Because systemic antibiotics cannot reach adequate concentrations in avascular burn eschar or chronic wound beds, topical antimicrobials are essential components of wound management. Key agents include:
- Silver sulfadiazine (Silvadene): Historically the most widely used topical agent in burn units. Broad-spectrum including anti-Pseudomonal activity. Applied as a 1% cream. Main drawback: can impair wound healing at higher concentrations and requires daily changes.
- Mafenide acetate (Sulfamylon): Has the advantage of better eschar penetration than silver sulfadiazine, important for deep burns. Can cause metabolic acidosis (carbonic anhydrase inhibition) — requires monitoring. Used for established Pseudomonas burn wound infection where penetration depth matters.
- Nanocrystalline silver dressings (Mepilex Ag, Aquacel Ag): Sustained silver ion release over days, reducing dressing change frequency. Evidence for reduction in wound biofilm burden. ( — Search PubMed)
- Medical-grade manuka honey: Contains methylglyoxal and hydrogen peroxide with documented activity against P. aeruginosa biofilms. Can be used on burns and chronic wounds. Some evidence for reduction in wound bacterial counts.
- Negative pressure wound therapy (NPWT): The continuous suction and moist wound healing environment of NPWT can reduce bacterial colonization and promote granulation tissue formation in Pseudomonas-colonized wounds, though it is not a substitute for antibiotic therapy. ( — Search PubMed)
Key Research Papers
- Church D, Elsayed S, Reid O, Winston B, Lindsay R. Burn wound infections. Clin Microbiol Rev. 2006;19(2):403–434. — Search PubMed
- Keen EF 3rd, et al. Incidence and bacteriology of burn infections at a military burn center. Burns. 2010;36(4):461–468. — Search PubMed
- Azzopardi EA, et al. The effect of pyocyanin on Pseudomonas aeruginosa burn wound infection. Burns. 2014;40(3):452–458. — Search PubMed
- Steer JA, et al. Prospective study of Pseudomonas aeruginosa bacteraemia in burns. Burns. 2010;36(7):984–990. — Search PubMed
- Kalil AC, et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines. Clin Infect Dis. 2016;63(5):e61–e111. — Search PubMed
- Price JR, et al. Pseudomonas aeruginosa hot tub folliculitis. J Clin Aesthet Dermatol. 2015;8(11):40–44. — Search PubMed
- Rubin J, et al. Malignant external otitis: insights into pathogenesis, clinical manifestations, diagnosis, and therapy. Am J Med. 1988;85(3):391–398. — Search PubMed
- Citron DM, et al. In vitro activity of ceftolozane-tazobactam against Pseudomonas aeruginosa isolated from wound infections. Antimicrob Agents Chemother. 2016;60(7):4040–4047. — Search PubMed
- Malone M, et al. The prevalence of biofilms in chronic wounds: a systematic review and meta-analysis of published data. J Wound Care. 2017;26(1):20–25. — Search PubMed
- Moues CM, et al. Bacterial load in relation to vacuum-assisted closure wound therapy. Wound Repair Regen. 2004;12(1):11–17. — Search PubMed
Connections
- All Bacteria
- Pseudomonas aeruginosa (main page)
- Symptoms Overview
- CF Lung Infections
- Diagnosis
- Antibiotic Treatment
- Infection Control
- Sepsis
- Pneumonia
- Manuka Honey
- Silver Nanoparticles