Valine for Nitrogen Balance and Wound Healing
Surgical recovery, traumatic injury, severe burns, and chronic wasting diseases share a common biochemical signature: negative nitrogen balance, in which urinary nitrogen excretion exceeds dietary nitrogen intake. Net protein loss in this state runs at 50-100 g/day in major trauma and up to 200 g/day in extensive burns — equivalent to losing a quarter of total muscle mass per month if uncorrected. Valine's contribution to reversing this loss operates through three connected mechanisms: (1) direct substrate for accelerated tissue synthesis at wounds and surgical sites; (2) nitrogen donor to muscle glutamine pool, the dominant amino acid exported from muscle to gut and immune cells during healing; (3) BCAA-mediated suppression of muscle proteolysis through mTOR signaling. The Marchesini studies and other BCAA-enriched parenteral and oral nutrition trials in cirrhosis, trauma, and surgical recovery have established that targeted BCAA support can shift the nitrogen balance toward positive faster than equivalent-nitrogen non-BCAA-enriched feeding. This page covers the biochemistry, the clinical evidence, and the practical applications.
Table of Contents
- Nitrogen Balance: The Basic Concept
- Negative Nitrogen Balance in Catabolic States
- Valine as Direct Substrate for Tissue Synthesis
- Valine Contribution to Muscle Glutamine
- BCAA-Enriched Parenteral Nutrition for Cirrhosis
- The Marchesini Long-Term Oral BCAA Protocol
- Trauma and Burn Applications
- Perioperative Nutrition and Surgical Recovery
- Mechanisms of BCAA Contribution to Wound Healing
- Cautions and Contraindications
- Key Research Papers
- Connections
- Featured Videos
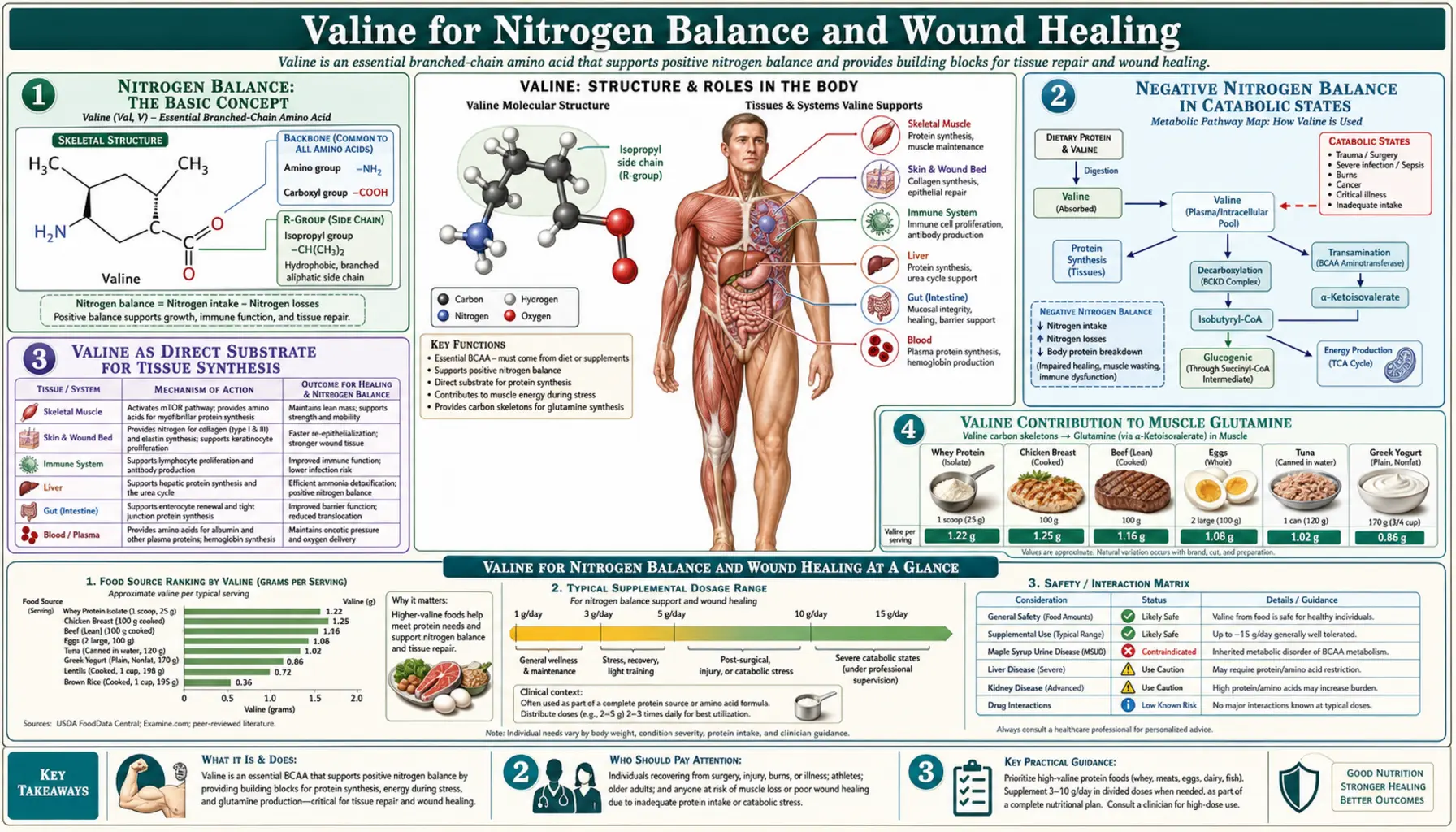
Nitrogen Balance: The Basic Concept
Nitrogen balance is the simplest quantitative way to assess net protein utilization in the body. Because nitrogen is present at approximately 16% of the mass of all amino acids and is essentially absent from carbohydrates and fats, measuring nitrogen intake and excretion gives a usable measure of net protein anabolism (positive balance, more protein synthesized than degraded) or net protein catabolism (negative balance, more degraded than synthesized).
Nitrogen balance is calculated as:
Nitrogen balance = (dietary protein g/day ÷ 6.25) − (urinary urea nitrogen + fecal N + integumentary N losses)
The factor 6.25 converts dietary protein grams to dietary nitrogen grams (assuming 16% N content). Urinary urea nitrogen (UUN) is the dominant excretory route and the most-measured component, captured by 24-hour urine collection. Fecal nitrogen losses average about 1-2 g/day in healthy adults; integumentary losses (skin, hair, nails) approximately 0.5 g/day. A standard adjustment of 4 g/day total non-urinary loss is often used.
Positive nitrogen balance occurs during growth (children, adolescents), pregnancy, lactation, recovery from illness or injury, and during anabolic training with adequate protein. Negative balance occurs during fasting, severe illness, immobilization, aging (slowly), and frank protein malnutrition. The biological imperative for any patient in catabolic illness is to reverse negative nitrogen balance as quickly as possible, because sustained loss of structural and functional protein from muscle, immune system, and visceral organs compounds morbidity and mortality.
For most healthy adults, nitrogen balance approximates zero at a protein intake of about 0.8 g/kg/day, which is the basis of the RDA. However, this is the intake required to prevent loss in healthy young adults at rest. For older adults, athletes, and patients in any catabolic state, the requirement is substantially higher (1.0-2.0 g/kg/day depending on context). Insufficient intake leads to sustained negative balance and progressive lean tissue loss.
Negative Nitrogen Balance in Catabolic States
Several clinical states produce sustained negative nitrogen balance even with feeding:
- Major trauma — multi-system trauma (motor vehicle accidents, falls from height, polytrauma) drives nitrogen loss of 15-30 g/day for 7-14 days post-injury. Total protein loss across this acute phase can reach 200-400 grams — equivalent to several pounds of muscle.
- Severe burns — extensive burns (>40% body surface area) produce the most extreme catabolism documented in clinical medicine, with nitrogen losses of 30-50 g/day for weeks or months. Burn patients require 2-3 g/kg/day protein intake just to approach nitrogen balance, and often run negative even at maximal feeding.
- Sepsis with prolonged ICU stay — severe sepsis triggers a cytokine-mediated catabolic cascade involving IL-6, TNF-alpha, and cortisol, driving nitrogen loss of 15-25 g/day for the duration of acute illness. Long-term ICU survivors often emerge with 20-30% loss of lean body mass (ICU-acquired weakness).
- Cancer cachexia — advanced cancer of certain types (pancreatic, lung, gastric, head/neck) produces a chronic catabolic state with progressive muscle and adipose loss, mediated by both tumor-derived factors (proteolysis-inducing factor) and host inflammatory cytokines. Cachexia accounts for an estimated 20-40% of cancer deaths.
- Cirrhosis — advanced liver disease produces a chronic low-grade catabolic state through altered amino acid metabolism, hyperammonemia, and frequent intercurrent illnesses. Sarcopenia is present in 40-70% of cirrhotic patients awaiting liver transplant and is a strong independent predictor of post-transplant outcomes.
- Major surgery — uncomplicated elective surgery produces transient negative nitrogen balance lasting 3-7 days post-op. Complicated or prolonged surgery extends this period considerably.
- Prolonged immobilization / bed rest — even without illness, simple bed rest produces measurable protein loss within days, accelerating in older adults.
The endocrine signature of these states is consistent: elevated cortisol, glucagon, and catecholamines, often with insulin resistance, driving net muscle proteolysis. The amino acids released — particularly the BCAAs, glutamine, and alanine — are exported from muscle to support gluconeogenesis, immune cell proliferation, wound healing, and hepatic acute-phase protein synthesis. The total protein lost from muscle far exceeds what is used productively at these other sites; the inefficiency is part of why catabolic illness produces such rapid and substantial wasting.
Valine as Direct Substrate for Tissue Synthesis
The reparative processes triggered by wounding, surgery, or trauma all require new protein synthesis at the affected tissue, plus accelerated protein synthesis at related organs (liver for acute-phase proteins, bone marrow for hematopoiesis, gut for mucosal repair, immune cells for inflammatory response). Each of these synthetic processes requires the full panel of essential amino acids, and valine's 5-6% representation in tissue protein means valine is required in roughly the same proportion.
The specific tissues most rapidly synthesizing during healing include:
- Skin and connective tissue at wound sites — keratinocytes, fibroblasts, and vascular endothelium proliferating to close wounds. Collagen synthesis is the dominant volumetric protein contribution; collagen contains a modest valine fraction (~2-4% depending on type), so collagen-rich tissue synthesis is less valine-demanding than muscle synthesis.
- Skeletal muscle at sites of damage (sarcomeric remodeling after exercise; muscle regeneration after laceration, contusion, or surgical incision) — valine fraction approximately 5-6% as noted above.
- Hepatic acute-phase proteins — C-reactive protein, fibrinogen, haptoglobin, complement proteins, alpha-1 antitrypsin, ceruloplasmin. These rise dramatically in acute inflammation and require substrate amino acids from the dietary or muscle pool.
- Immune cell expansion — activated B and T lymphocytes, neutrophils, macrophages, all undergoing rapid proliferation with concomitant protein synthesis demands.
- Erythropoiesis — in patients with significant blood loss or anemia of chronic disease, bone marrow erythropoiesis requires not only iron but adequate amino acid substrate for globin synthesis. Hemoglobin has a notable valine content (the alpha chain has approximately 5-6% valine residues, the beta chain similar).
The famous "Valine 6 to Glutamate" mutation in beta-globin produces sickle cell disease — a glutamate-to-valine substitution at position 6 of the beta chain alters the protein's polymerization properties and produces the characteristic deoxy-hemoglobin polymer and red cell sickling. This is one of the most-cited examples in introductory biochemistry of how a single amino acid substitution can produce dramatic phenotypic consequences, and the substituted amino acid is valine specifically because of its hydrophobic, branched side chain that fits a complementary pocket on adjacent beta chains and drives polymerization.
The bottom line: any condition that increases the rate of tissue synthesis — healing, recovery, growth, athletic training — increases the absolute demand for valine alongside other amino acids. The 2:1:1 BCAA pattern in muscle composition means valine demand parallels leucine and isoleucine demand in synthesis-favoring states.
Valine Contribution to Muscle Glutamine
Glutamine is the most abundant free amino acid in the body and the dominant amino acid exported from skeletal muscle during catabolic illness. Plasma glutamine concentrations are approximately 600-700 µmol/L — far higher than any other amino acid. Glutamine plays multiple critical roles in catabolic states:
- Fuel for rapidly dividing cells — enterocytes (gut lining cells), lymphocytes, macrophages, and tumor cells preferentially consume glutamine as fuel, oxidizing it through glutaminolysis to alpha-ketoglutarate and then TCA cycle
- Nitrogen carrier — glutamine transports nitrogen from peripheral tissues to liver and kidney for disposal as urea or ammonia
- Acid-base regulation — renal ammonia generation from glutamine is the major adaptive response to metabolic acidosis
- Nucleotide synthesis substrate — glutamine's amide nitrogen feeds purine and pyrimidine synthesis in proliferating cells
- Glutathione precursor — via glutamate, glutamine indirectly supplies the rate-limiting amino acid for glutathione synthesis
- Gut mucosal integrity — enterocyte glutamine consumption supports the structural integrity of the intestinal lining and is a primary reason for enteral nutrition's superiority over parenteral nutrition in critical illness
Glutamine is conventionally classified as a "conditionally essential" amino acid — the body can synthesize it from glutamate and ammonia in healthy states, but synthesis becomes inadequate during catabolic stress, and plasma glutamine often falls into low-normal or frankly deficient ranges in severe illness. Glutamine supplementation has been tested in numerous ICU and trauma trials with mixed results — some early benefits suggested but later large-scale trials (REDOXS, MetaPlus) showed potential harm in some severely ill populations, leading to current guidelines that recommend against parenteral glutamine in shock/multi-organ failure but permit it selectively in trauma and burn patients.
The valine connection is that BCAA transamination in skeletal muscle is a major nitrogen source for muscle glutamine synthesis. The BCAT2 enzyme transfers the amino group from valine (and leucine and isoleucine) to alpha-ketoglutarate, forming glutamate. Glutamate is then amidated by glutamine synthetase (using a second nitrogen from ammonia) to form glutamine. The net effect: valine catabolism provides one of the two nitrogens in every glutamine molecule synthesized by muscle.
This biochemistry means that adequate BCAA intake during catabolic illness supports glutamine synthesis at the periphery. BCAA-enriched feeding has been proposed and tested as an indirect way to support glutamine without the safety concerns of pure glutamine infusion. The data are suggestive but not definitive; current clinical practice incorporates this rationale in choosing BCAA-enriched enteral formulas for selected high-catabolic patients.
BCAA-Enriched Parenteral Nutrition for Cirrhosis
The first clinical condition where BCAA-enriched nutrition was systematically studied was hepatic encephalopathy in cirrhosis. Building on the Fischer-Baldessarini observation of altered amino acid profiles in liver failure, Fischer and colleagues at Harvard developed BCAA-enriched parenteral formulas (initially HepatAmine, later commercial variants) and tested them in randomized trials starting in the 1970s.
The rationale combined two mechanisms: (1) restoring the BCAA-to-AAA ratio (Fischer ratio) to normalize neurotransmitter precursor balance and reduce encephalopathic symptoms; (2) providing readily-utilizable nitrogen substrate that bypasses the failing liver, since BCAAs are primarily metabolized in peripheral muscle rather than liver.
The intravenous BCAA-enriched formulations typically contain 35-45% BCAAs by amino acid content (compared to about 18-20% in standard amino acid solutions), reflecting the 2:1:1 ratio at higher absolute concentrations. Trials in acute hepatic encephalopathy showed:
- Faster resolution of encephalopathy (mental status normalization) in BCAA-enriched arm vs standard amino acid arm
- Improved nitrogen balance (less negative or more positive) in BCAA-enriched feeding
- Reduced plasma aromatic amino acid concentrations and partial normalization of the Fischer ratio
- No clear mortality benefit in early trials (mortality in advanced cirrhosis is driven by liver failure itself more than by encephalopathy)
European guidelines (ESPEN) recommend BCAA-enriched parenteral nutrition as an option in cirrhotic patients with encephalopathy who require IV nutrition support. North American guidelines (ASPEN) take a more permissive but less recommendational stance, considering it appropriate for selected patients but not standard of care.
The Marchesini Long-Term Oral BCAA Protocol
The most influential outpatient application of BCAA nutrition for cirrhosis came from Giulio Marchesini and colleagues in Bologna, who designed and tested a long-term oral BCAA supplementation regimen for cirrhotic patients with prior hepatic encephalopathy. The Marchesini 2003 Gastroenterology trial enrolled 174 patients with advanced cirrhosis and a history of encephalopathy and randomized them to:
- BCAA supplement: 12.45 g/day BCAA in 2:1:1 ratio, divided three times daily
- Lactoalbumin (an isonitrogenous control providing equivalent total amino acid nitrogen)
- Maltodextrin (a calorie-matched non-protein control)
The primary endpoint was a composite of death, liver-related mortality, severity of decompensation, and hospital admissions over 12 months of treatment. Key findings:
- BCAA supplementation significantly reduced the composite endpoint compared to maltodextrin
- Numerical advantage of BCAA over lactoalbumin was present but smaller and not statistically significant on the primary endpoint
- Improvements in serum albumin, lean body mass, and quality-of-life scores favored the BCAA arm
- Recurrence of overt hepatic encephalopathy was reduced in the BCAA group
- Adherence was a significant challenge — BCAA supplements have an unpleasant bitter taste, and a substantial fraction of randomized patients did not maintain protocol intake
The Marchesini protocol has been replicated and extended in subsequent trials, with a 2017 Cochrane Review (Gluud et al.) confirming benefit for hepatic encephalopathy outcomes from long-term oral BCAA supplementation in cirrhosis. The mechanism connects directly to the nitrogen balance and substrate-availability themes of this page: BCAA supplementation provides muscle-utilizable nitrogen substrate that bypasses the failing liver, supports lean tissue preservation in chronically catabolic patients, and improves the BCAA-to-AAA ratio for neurological benefit.
Practical Marchesini-style regimen for outpatient cirrhotic patients with encephalopathy history:
- 0.25 g/kg/day BCAA in 2:1:1 ratio (typically 12-20 g/day total)
- Divided three times daily, taken with meals
- Continued indefinitely as part of medical nutrition therapy
- Total daily protein target maintained at 1.0-1.2 g/kg/day (the historical "protein restriction" for hepatic encephalopathy is now considered counterproductive in most patients)
- Late-evening snack with carbohydrate plus BCAA dose, to interrupt overnight catabolism and protect lean mass
Trauma and Burn Applications
The trauma/burn literature for BCAA-enriched nutrition is older and the conclusions more mixed than the cirrhosis literature. Multiple trials in the 1980s and 1990s tested BCAA-enriched parenteral nutrition vs standard amino acid PN in trauma and burn patients, with most showing modest improvements in nitrogen balance but inconsistent effects on harder clinical endpoints (infection rate, ventilator days, ICU length of stay, mortality).
Contemporary critical care nutrition guidelines from ASPEN and SCCM do not strongly recommend BCAA-enriched formulas as standard for trauma or burn patients. Instead, the guidelines emphasize:
- Adequate total protein delivery (1.2-2.0 g/kg/day for trauma; up to 2.5-3.0 g/kg/day for severe burns)
- Preference for enteral over parenteral route when feasible
- Early initiation of nutrition (within 24-48 hours)
- Adequate energy delivery (25-30 kcal/kg/day for trauma; higher for burns)
The supplemental contribution of BCAA-enrichment to these total-protein goals is now seen as marginal — adequate total protein from any high-biological-value source provides ample BCAAs in the 2:1:1 ratio naturally, without the need for BCAA-enriched formulations. The exception remains hepatic encephalopathy and certain hyperammonemic states, where BCAA-enrichment has more specific physiological rationale.
For burn patients specifically, the modern emphasis is on glutamine repletion (enteral glutamine 0.3-0.5 g/kg/day has been shown to improve outcomes in burns specifically, distinct from the lack of benefit in general ICU populations) and ample whole-protein delivery. BCAA-enriched formulas have largely been deprecated in modern burn nutrition.
Perioperative Nutrition and Surgical Recovery
Enhanced Recovery After Surgery (ERAS) protocols have transformed perioperative nutrition over the past two decades. Traditional preoperative fasting from midnight has been replaced by carbohydrate-rich clear fluids up to 2 hours before surgery, and early postoperative oral feeding (within hours) has been adopted in most major procedures. Within this framework, nutritional optimization has shifted to:
- Preoperative protein loading — sarcopenic or undernourished patients identified at the preop assessment benefit from 2-4 weeks of supplemental protein (1.5-2.0 g/kg/day) before elective surgery to optimize lean mass and postoperative recovery
- Immune-enhanced enteral formulas — formulas combining glutamine, arginine, omega-3 fatty acids, and nucleotides have shown benefit in reducing postoperative infections in selected populations (head/neck and GI cancer surgery), though the effect size is modest and not all subgroups benefit
- Early postoperative protein resumption — advancing to full protein intake within 24-48 hours postop, supported by oral or enteral feeding, accelerates return of nitrogen balance
- BCAA supplementation in specific contexts — cirrhotic patients undergoing hepatectomy or liver transplant evaluation; sarcopenic elderly patients undergoing major surgery; some bariatric surgery populations
The specific role of BCAA supplementation in surgical recovery has been studied in hepatic surgery extensively. Studies of BCAA-enriched oral nutrition for 1-2 weeks postoperatively in patients undergoing hepatectomy for hepatocellular carcinoma have shown improvements in albumin recovery, ascites resolution, and quality-of-life scores. Japanese liver surgery centers have integrated BCAA supplementation into standard postoperative care for these patients; Western centers vary in adoption.
For most elective surgery in well-nourished patients, the contribution of BCAA-enrichment beyond adequate total protein is small. Where BCAA-enrichment matters most is in patients who enter surgery in a sarcopenic, sub-optimally nourished, or otherwise catabolically primed state, and where the postoperative course is expected to be prolonged or complicated.
Mechanisms of BCAA Contribution to Wound Healing
At the wound site, several specific BCAA-related mechanisms have been characterized:
- Direct substrate for collagen, elastin, fibrin, and cellular protein synthesis at the wound. Although collagen itself is relatively valine-poor (collagen is rich in glycine, proline, and hydroxyproline), the surrounding cellular machinery synthesizing collagen requires standard amino acid substrate composition.
- mTOR-mediated promotion of fibroblast proliferation at the wound site. Local leucine concentrations at wound exudate are typically elevated due to the rapid proteolysis of damaged tissue, supporting an anabolic local environment.
- Immune cell support — wound macrophages and neutrophils consume substantial amino acid substrate during the acute inflammatory phase. Adequate BCAA availability supports this immune response.
- Reduced peripheral proteolysis — oral BCAA intake reduces the muscle proteolysis that would otherwise mobilize amino acids for the wound. This is "spared" muscle protein.
- Glutamine support — via the transamination pathway discussed above, BCAAs contribute nitrogen to glutamine synthesis, and glutamine is preferentially consumed by enterocytes (maintaining gut barrier function during illness) and immune cells (supporting host defense).
- Insulin sensitization in some contexts — BCAA + arginine combination has been shown to improve glucose tolerance in some surgical contexts, indirectly supporting wound healing (hyperglycemia impairs wound healing).
- HMB (beta-hydroxy-beta-methylbutyrate) — the leucine metabolite has been studied specifically for wound healing in chronic pressure ulcers and surgical wounds, with some evidence of benefit. HMB is produced endogenously from approximately 5% of dietary leucine, so adequate leucine intake (and balanced BCAA intake) supports HMB availability.
Practical wound nutrition recommendations, integrating these mechanisms:
- Adequate total protein at 1.2-1.5 g/kg/day for adults with significant wounds, higher (1.5-2.0 g/kg/day) for chronic non-healing wounds or pressure ulcers
- Adequate caloric intake — protein cannot be efficiently used for tissue synthesis if total energy intake is insufficient
- Vitamin C, zinc, and adequate iron status for collagen synthesis and cellular proliferation
- Arginine supplementation in some contexts (oral wound nutrition formulas) for nitric oxide-mediated vasodilation and immune support
- For chronic pressure ulcers, oral HMB-arginine-glutamine combinations (e.g., the Juven product) have RCT evidence for accelerated healing
Cautions and Contraindications
- Maple syrup urine disease and related BCAA metabolism disorders — absolute contraindication. BCAA supplements cannot be given to patients with MSUD, propionic acidemia, methylmalonic acidemia, or isovaleric acidemia outside of carefully managed metabolic disease centers with specialized formulations.
- Acute hepatic failure with severe hyperammonemia — the standard advice is to avoid high-protein loading, including BCAA loading, in acute hepatic failure with grade 3-4 encephalopathy. BCAA-enriched parenteral nutrition may be appropriate in this context if total protein delivery is being maintained, but the situation requires hepatology and nutrition team management.
- Chronic kidney disease (advanced stages) — high amino acid intake increases nitrogen load on impaired kidneys. Stage 3+ CKD patients should consult nephrology before adding BCAA supplements; very-low-protein diets with keto-analog supplementation (a specialized approach) include BCAA keto-analogs specifically to avoid the Harper imbalance problem.
- Insulin resistance and type 2 diabetes — while moderate dietary BCAA from food sources is not harmful, chronic high-dose BCAA supplementation in obese insulin-resistant patients should be approached with caution. The Wang/Newgard biomarker work showed elevated plasma BCAAs associated with insulin resistance; whether this is causal or consequential is debated, but pushing BCAAs higher in this population may not be optimal.
- Pregnancy and lactation — dietary BCAA intake is appropriate and required, but pharmacological-dose BCAA supplementation is not well-studied in pregnancy. Pregnant and breastfeeding women should rely on food sources rather than supplements unless specifically indicated.
- Pediatric use — BCAA supplementation outside of clinical management of specific disorders is not recommended in children. Children's amino acid requirements are met by normal dietary protein.
Key Research Papers
- Marchesini G et al. (2003). Nutritional supplementation with branched-chain amino acids in advanced cirrhosis: a double-blind, randomized trial. Gastroenterology. — PubMed
- Gluud LL et al. (2017). Branched-chain amino acids for people with hepatic encephalopathy (Cochrane Review). — PubMed
- Fischer JE et al. (1976). The role of plasma amino acids in hepatic encephalopathy. Surgery. — PubMed
- Plauth M et al. (2019). ESPEN guideline on clinical nutrition in liver disease. Clinical Nutrition. — PubMed
- Williams JZ, Barbul A (2003). Nutrition and wound healing. Surgical Clinics of North America. — PubMed
- Wischmeyer PE et al. (2013). Glutamine in the critically ill. Current Opinion in Critical Care. — PubMed
- Heyland D et al. (2013). A randomized trial of glutamine and antioxidants in critically ill patients (REDOXS). NEJM. — PubMed
- Stehle P et al. (2017). Glutamine dipeptide-supplemented parenteral nutrition improves the clinical outcomes of critically ill patients: a systematic evaluation of randomised controlled trials. Clinical Nutrition ESPEN. — PubMed
- Posthauer ME et al. (2015). The role of nutrition for pressure ulcer management. Advances in Skin & Wound Care. — PubMed
- Sallé A et al. (2008). Beta-hydroxy-beta-methylbutyrate, arginine and glutamine supplementation in pressure ulcer healing. Journal of Parenteral and Enteral Nutrition. — PubMed
- Singer P et al. (2019). ESPEN guideline on clinical nutrition in the intensive care unit. Clinical Nutrition. — PubMed
- Tsien C et al. (2015). Late evening snack: exploiting a period of anabolic opportunity in cirrhosis. Journal of Gastroenterology and Hepatology. — PubMed
PubMed Topic Searches
- PubMed: BCAA for cirrhosis
- PubMed: BCAA and nitrogen balance
- PubMed: Marchesini long-term oral BCAA
- PubMed: Glutamine and BCAA in critical care
- PubMed: HMB and wound healing
Connections
- Valine Overview
- Valine Benefits Hub
- Valine for Muscle Protein Synthesis
- Valine for Energy Metabolism
- Valine for Cognitive Performance
- Leucine (BCAA Partner)
- Isoleucine (BCAA Partner)
- Glutamine
- Arginine
- Alanine
- Liver Disease
- Vitamin C (Collagen Synthesis)
- Zinc (Wound Healing)
- All Amino Acids