Valine for Muscle Protein Synthesis
Valine is one of the three branched-chain amino acids (BCAAs), the structural and signaling trio that constitutes roughly one-third of skeletal muscle protein. The conventional 2:1:1 leucine:isoleucine:valine ratio in BCAA supplements is not arbitrary — it mirrors the relative abundance of these three amino acids in muscle tissue itself. Yet valine is the most frequently shortchanged member of the trio, especially in leucine-only "anabolic activator" supplements that promise mTOR signaling but ignore the substrate-availability problem. The Harper imbalance hypothesis, formulated by Alfred Harper in the 1960s, demonstrated that excess leucine alone can paradoxically depress growth in animal models by competitively depleting plasma valine and isoleucine. This page explains why balanced BCAA intake matters more than leucine maximalism, how valine specifically contributes to mTOR activation, and the clinical contexts where the 2:1:1 ratio has been validated.
Table of Contents
- Valine as One of Three BCAAs
- The 2:1:1 Leucine:Isoleucine:Valine Ratio Rationale
- Valine's Role in mTOR Signaling and Protein Synthesis
- The Harper BCAA Imbalance Hypothesis
- The Leucine-Only Supplementation Trap
- Valine in Muscle Tissue Composition
- Post-Exercise Recovery and Soreness Reduction
- Sarcopenia and the Aging Muscle
- Clinical Applications: Cachexia, Trauma, ICU
- Practical Dosing Strategies
- Key Research Papers
- Connections
- Featured Videos
Valine as One of Three BCAAs
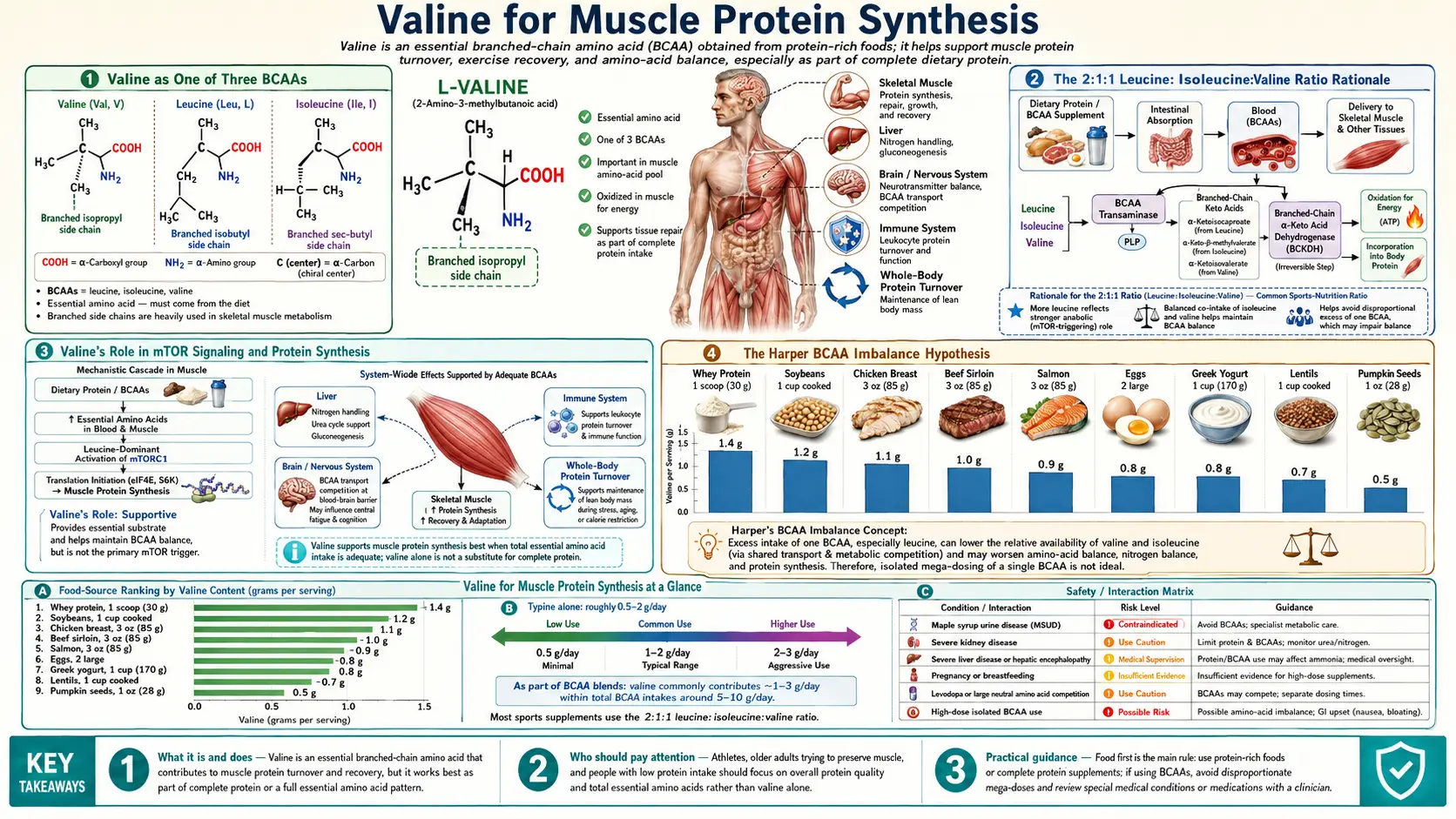
The three branched-chain amino acids — leucine, isoleucine, and valine — share a defining structural feature: a non-linear, branched aliphatic side chain that distinguishes them from the other 17 proteinogenic amino acids. The branching is what gives them both their name and their distinctive metabolic behavior. Unlike most amino acids, which are processed first by the liver upon absorption, BCAAs largely bypass first-pass hepatic metabolism and are instead taken up directly by skeletal muscle, where the enzymes that initiate their catabolism (branched-chain aminotransferase, BCAT2, and the rate-limiting branched-chain alpha-ketoacid dehydrogenase, BCKAD complex) are most abundant.
This direct muscular routing is what makes BCAAs especially relevant to athletic and clinical contexts where rapid amino acid availability at the muscle is required. Within the trio, each amino acid plays a partially distinct role: leucine is the principal anabolic signaling amino acid, the most potent activator of the mTOR (mechanistic target of rapamycin) pathway; isoleucine contributes to glucose uptake by muscle through both insulin-dependent and insulin-independent pathways; valine serves both as a substrate for protein synthesis and as a metabolic feedstock for the TCA cycle via succinyl-CoA. All three are essential amino acids — the human body cannot synthesize them de novo and must obtain them through diet or supplementation.
Yet the three are not interchangeable. The supplement industry has historically over-emphasized leucine because of its singular role in mTOR activation, leading to a series of products marketed as "leucine boosters" or "anabolic activators" that contain little or no valine and isoleucine. The biochemistry of muscle protein synthesis, however, requires substrate from all three plus the other six essential amino acids — mTOR activation without substrate availability is like turning on a factory's power without delivering the raw materials. This substrate-vs-signal distinction is central to understanding why balanced BCAA intake matters more than leucine maximalism.
The 2:1:1 Leucine:Isoleucine:Valine Ratio Rationale
The standard BCAA supplement ratio of 2:1:1 (leucine:isoleucine:valine) is not arbitrary; it reflects the approximate ratio of these three amino acids in human skeletal muscle protein. When muscle is broken down (analyzed by hydrolysis and amino acid quantification), the BCAA content typically falls in the range of 20-22% leucine, 10-12% isoleucine, and 10-12% valine relative to total amino acid content. The 2:1:1 ratio therefore approximately mirrors the substrate composition of the tissue being built.
Some product lines have promoted alternative ratios — 4:1:1, 8:1:1, even 10:1:1 — on the theory that more leucine is always better for mTOR activation. The clinical evidence does not support these higher ratios. A 2017 systematic review of BCAA supplementation trials found no consistent advantage for ratios above 2:1:1 in terms of muscle protein synthesis, recovery, or hypertrophy outcomes. The downside of high-leucine ratios is precisely the Harper imbalance problem: by saturating the BCAT2 enzyme with leucine, the metabolism of valine and isoleucine is competitively inhibited, and plasma levels of both drop. The mTOR pathway may be activated, but the actual substrates for new muscle protein become limiting.
A practical implication: when comparing BCAA supplements, the ratio is just as important as the total dose. A 5-gram serving at 2:1:1 (2.5g leucine, 1.25g isoleucine, 1.25g valine) is more bioavailable as muscle substrate than a 5-gram serving at 4:1:1 (3.33g leucine, 0.83g isoleucine, 0.83g valine), despite the lower absolute leucine content in the former. Whole food protein (whey, casein, egg, meat) provides BCAAs in approximately the 2:1:1 ratio naturally, which is one of several reasons that food-source protein consistently outperforms isolated BCAA supplements in muscle synthesis trials.
Valine's Role in mTOR Signaling and Protein Synthesis
The mTOR pathway is the central regulator of cellular anabolism. mTOR exists in two complexes: mTORC1 (rapamycin-sensitive, the canonical anabolic kinase) and mTORC2 (less rapamycin-sensitive, involved in cytoskeletal regulation and Akt signaling). Muscle protein synthesis is driven primarily through mTORC1, which when active phosphorylates two key downstream targets: 4E-BP1 (releasing eIF4E to initiate cap-dependent mRNA translation) and p70S6K (activating the ribosomal S6 kinase to increase translation throughput).
Leucine is the dominant amino acid signal to mTORC1. Leucine is sensed by Sestrin2, a cytoplasmic leucine sensor that, when leucine-loaded, releases its inhibition of GATOR2, which in turn permits Rag GTPases to recruit mTORC1 to the lysosomal surface where it can be activated by Rheb. This is a beautifully specific molecular sensing mechanism, and it is why leucine alone can transiently activate the pathway. However, sustained mTORC1 activity and actual protein synthesis require additional inputs: insulin signaling, mechanical load (exercise), energy status (low AMP/ATP ratio), and — critically — substrate availability of all the amino acids required to build the protein being synthesized.
Valine's role here is principally as substrate. When mTORC1 fires and ribosomes begin translating muscle protein mRNAs, the elongation step requires charged tRNAs for every codon, including valine codons (GUU, GUC, GUA, GUG — four of the 64 possible codons in the genetic code, used wherever a valine residue appears in the protein sequence). If valine-tRNA pools are depleted, elongation stalls at valine codons, and the ribosome cannot complete the protein. The classic experimental demonstration of this is the General Amino Acid Control (GAAC) response: when any one essential amino acid runs low, uncharged tRNA accumulates, which activates the GCN2 kinase, which phosphorylates eIF2alpha, which globally suppresses cap-dependent translation. The net result is that valine deficiency — even with abundant leucine and mTOR signaling — can dramatically reduce overall protein synthesis output.
Valine also contributes a second, more recently appreciated function in the mTOR pathway: Sestrin2 leucine sensing is competitive with valine and isoleucine at the binding site. While leucine binds Sestrin2 with the highest affinity, valine and isoleucine bind with lower but non-negligible affinity. This may explain why mixed BCAA supplements produce a longer and more sustained mTOR activation than equivalent leucine-only doses — the trio collectively maintains Sestrin2 in a "loaded" state for longer.
The Harper BCAA Imbalance Hypothesis
The most consequential discovery in BCAA nutrition was made by Alfred Harper at the University of Wisconsin in a series of experiments in the 1950s and 1960s. Harper was studying amino acid imbalance — specifically, why adding a single amino acid to an otherwise marginally adequate diet sometimes produced growth depression in rats rather than the expected improvement. His seminal observation was that excess dietary leucine caused growth depression that could be reversed by adding valine and isoleucine. This finding became known as the "BCAA antagonism" or "Harper imbalance hypothesis."
The mechanism Harper proposed, later confirmed at the molecular level, is competitive: all three BCAAs share the same transamination enzyme (branched-chain aminotransferase, BCAT) and the same rate-limiting dehydrogenase complex (BCKAD). When dietary leucine is in large excess, it competitively saturates these enzymes, accelerating its own catabolism and incidentally accelerating the catabolism of any valine and isoleucine present. The net effect is that excess leucine literally depletes the body's pools of valine and isoleucine, creating a functional deficiency of two essential amino acids even when total nitrogen intake is adequate.
This is biochemically counterintuitive but practically important. The Harper effect has been replicated in multiple species (rat, pig, chicken, human) and across multiple endpoints (growth rate, plasma amino acid concentrations, muscle protein synthesis rates, hepatic protein turnover). In the contemporary human literature, the most thoroughly documented manifestation is in patients with chronic kidney disease on low-protein diets supplemented with keto-analogs of leucine — these patients exhibit reproducible drops in plasma valine and isoleucine and require explicit valine and isoleucine supplementation to maintain balance.
The Harper hypothesis also explains a longstanding observation in protein quality scoring: the "limiting amino acid" concept. In any given protein source, the amino acid present in lowest amount relative to requirement sets the upper limit on how much of that protein can actually be used for synthesis. The other amino acids, even if present in abundance, are degraded for energy rather than incorporated into new tissue. Valine is rarely the limiting amino acid in animal proteins, but in some plant proteins (particularly maize) it can become co-limiting alongside lysine, which is why traditional cuisines that pair maize with legumes (Mexican beans and corn, for example) produce a more complete amino acid profile than either food alone.
The Leucine-Only Supplementation Trap
Despite four decades of accumulated evidence supporting balanced BCAA intake, the supplement market continues to feature leucine-only and high-leucine-ratio products marketed for muscle building. The rationale presented to consumers focuses on mTOR activation: "leucine is the only amino acid that directly activates mTOR, so just take leucine." This framing is technically true about the signaling step but ignores the substrate-availability step.
The practical consequence of leucine-only supplementation in humans has been examined in several controlled trials. A 2017 study by Moberg and colleagues in American Journal of Physiology — Endocrinology and Metabolism compared post-exercise muscle protein synthesis after leucine alone vs full BCAAs (leucine + isoleucine + valine) vs essential amino acids (EAAs, all nine). The result: leucine alone produced a transient mTOR activation peak comparable to BCAAs and EAAs, but the actual integrated muscle protein synthesis over the recovery period was significantly lower with leucine alone than with BCAAs, and lower with BCAAs than with full EAAs. The leucine-only signal was present; the substrate to act on it was not.
For the athlete or patient choosing supplements, the practical takeaway is straightforward: balanced BCAA at 2:1:1 outperforms leucine alone; whole-protein EAA-complete sources outperform isolated BCAA. Whey protein, casein, egg protein, and high-quality meat or fish provide all nine essential amino acids in roughly the proportions needed for muscle synthesis, with the BCAA fraction naturally at 2:1:1. Isolated BCAAs are most useful in narrow contexts: intra-workout sipping when whole protein would cause gastrointestinal distress; specific clinical situations like cirrhotic encephalopathy where the BCAA-to-aromatic ratio matters; or supplementation of a marginally low-protein diet (e.g., some endurance-sport contexts during caloric restriction).
Valine in Muscle Tissue Composition
Quantitatively, valine constitutes approximately 5-6% of total amino acid residues in human skeletal muscle protein by weight. Across the major myofibrillar proteins:
- Myosin heavy chain (the most abundant muscle protein, the molecular motor of contraction): approximately 5.5% valine residues
- Actin (the second most abundant, the thin-filament protein): approximately 4.5% valine residues
- Titin (the largest known protein, the molecular spring providing passive tension): approximately 6.2% valine residues
- Troponin and tropomyosin (the regulatory proteins of the thin filament): approximately 5-7% valine residues
A 70-kg adult with approximately 28 kg of skeletal muscle (40% of body weight) carries roughly 5.6 kg of muscle protein, of which approximately 310 grams is valine residues. The daily turnover rate of muscle protein in a healthy adult is approximately 1-2%, meaning roughly 3-6 grams of valine residues are synthesized into muscle protein each day, and an approximately equal amount is liberated by proteolysis and either recycled (through reincorporation) or catabolized to succinyl-CoA via the BCKAD pathway.
This continuous turnover is the basis for the dietary valine requirement (~26 mg/kg/day per WHO, or ~1.8 g/day for a 70-kg adult). The requirement scales with muscle mass and with the rate of muscle remodeling: athletes engaged in heavy resistance training have approximately 50-100% higher muscle protein turnover and correspondingly higher valine (and overall BCAA) requirements. Patients in catabolic states (sepsis, severe burn, post-surgical recovery, advanced cancer cachexia) may have 200-300% higher turnover, justifying targeted BCAA supplementation as part of medical nutrition therapy.
Post-Exercise Recovery and Soreness Reduction
Resistance exercise produces microscopic damage to muscle fibers, particularly at the Z-disc and sarcomeric junctions, which is the structural basis for delayed-onset muscle soreness (DOMS) experienced 24-72 hours after a novel or intense training bout. The repair of this damage requires both mTOR signaling (to upregulate translation) and amino acid substrate (to provide the building blocks of new sarcomeric protein).
BCAA supplementation has been studied extensively for its effect on DOMS, with mixed but generally favorable results. A 2017 meta-analysis by Fouré and Bendahan pooled 15 randomized trials of BCAA supplementation around resistance exercise and found a modest but statistically significant reduction in DOMS severity (effect size approximately 0.5 standard deviations) and a small reduction in creatine kinase release (a marker of muscle damage). The benefit was most pronounced when BCAAs were taken before and during exercise, less pronounced when taken only after exercise, and was potentiated by adequate total protein intake.
Within the BCAA effect, valine's specific contribution is harder to dissect because human studies typically administer the trio together. Animal studies that have separated the BCAAs suggest that the soreness-reduction effect requires all three components, consistent with the substrate availability argument: damaged sarcomeres need to be rebuilt, and rebuilding requires balanced amino acid supply.
Practical recommendation for athletes: rather than dosing pure BCAA, prioritize total daily protein intake at 1.6-2.2 g/kg body weight per the contemporary recommendations from the International Society of Sports Nutrition, with protein evenly distributed across 4-5 meals containing 25-40 g of high-quality protein each. This pattern provides ample BCAA in the 2:1:1 ratio naturally and outperforms isolated BCAA supplementation in nearly all controlled comparisons.
Sarcopenia and the Aging Muscle
Sarcopenia — the progressive age-related loss of muscle mass, strength, and function — is a major contributor to frailty, falls, and loss of independence in older adults. By age 80, the average person has lost approximately 30% of the muscle mass present at age 30. The mechanism is partly anabolic resistance: older muscle requires higher amino acid concentrations to achieve the same mTOR activation and protein synthesis response that younger muscle achieves at lower concentrations. The protein RDA of 0.8 g/kg/day, set decades ago for healthy adults, is now widely recognized as inadequate for older adults, with most contemporary guidelines suggesting 1.0-1.2 g/kg/day as a minimum and 1.2-1.6 g/kg/day for older adults engaged in any form of physical training or recovering from illness.
Within this elevated protein requirement, the BCAA fraction — and valine specifically — remains in the same approximately 2:1:1 ratio as the muscle being preserved. Some clinical trials have tested whether leucine fortification (adding pure leucine to meals) can overcome anabolic resistance in older adults; results have been mixed, with some trials showing acute mTOR activation but limited long-term effects on muscle mass. As with younger adults, the limitation appears to be substrate, not signal: leucine fortification without proportional valine and isoleucine produces transient signaling without sustained synthesis.
The HMB (beta-hydroxy-beta-methylbutyrate) supplement — a leucine metabolite — has been studied as an alternative anabolic intervention in sarcopenia, particularly during periods of bed rest. Some evidence supports modest preservation of muscle mass during forced immobilization, though the effect is small compared to resistance exercise itself. For most older adults, the highest-yield interventions remain (1) progressive resistance training, (2) adequate total protein at 1.2-1.6 g/kg/day in 25-40g doses per meal, and (3) sufficient vitamin D status — in that order. Isolated BCAA or leucine supplementation is a distant fourth-line consideration.
Clinical Applications: Cachexia, Trauma, ICU
In severe catabolic illness — advanced cancer cachexia, major trauma, severe burns, sepsis with prolonged ICU stay — the body's muscle protein turnover dramatically accelerates, with proteolysis outpacing synthesis and producing rapid lean tissue loss. BCAA-enriched nutrition has been studied in each of these contexts:
- Cancer cachexia — trials of BCAA-enriched oral nutrition supplements (typically 5-10 g BCAA in 2:1:1 ratio added to standard supplements) have shown modest preservation of lean body mass and improvement in some quality-of-life measures, though effects on overall mortality have been inconsistent. The European Society for Clinical Nutrition and Metabolism (ESPEN) cancer cachexia guidelines do not strongly recommend BCAA enrichment as standard but consider it reasonable in selected patients.
- Major trauma and post-surgical recovery — BCAA-enriched parenteral nutrition was extensively studied in the 1980s and 1990s in surgical and trauma ICU contexts. Most trials showed improved nitrogen balance with BCAA enrichment but only marginal improvements in clinical outcomes, leading current ICU nutrition guidelines (ASPEN/SCCM) to recommend standard protein dosing (1.2-2.0 g/kg/day) rather than BCAA-specific formulations as the primary intervention.
- Severe burns — burn patients have among the highest documented protein requirements (up to 2.5-3 g/kg/day), and BCAA-enriched formulas have been used historically. Modern burn nutrition emphasizes total energy and protein adequacy with high-biological-value whole protein sources over BCAA-specific enrichment.
- Sepsis — the role of BCAAs in sepsis is more uncertain. Some animal studies suggest that elevated plasma BCAAs may exacerbate insulin resistance and worsen outcomes in sepsis; clinical guidelines do not recommend BCAA-enriched feeding for sepsis routinely.
The thread running through these clinical contexts is the same as in athletic supplementation: substrate adequacy through total protein intake is more impactful than isolated BCAA dosing, and balanced BCAA outperforms isolated leucine when supplementation is used.
Practical Dosing Strategies
For most adults pursuing muscle health, the most effective valine "supplementation" is simply adequate dietary protein in the 2:1:1 BCAA ratio that occurs naturally in animal proteins and many plant proteins. Some practical anchors:
- General adult requirement (sedentary): WHO 26 mg/kg/day of valine, approximately 1.8 g/day for a 70-kg adult, met by ~80 g of total protein from mixed sources.
- Recreationally active adult: 1.2-1.6 g/kg/day total protein, distributed across 4-5 meals of 25-40 g protein each. Valine intake of approximately 3-5 g/day at this protein level, no supplementation needed.
- Strength/hypertrophy athlete: 1.6-2.2 g/kg/day total protein. If isolated BCAA is used (typically not necessary), 5-10 g of 2:1:1 BCAA around training; not before bed, not on rest days.
- Endurance athlete: 1.2-1.8 g/kg/day total protein. BCAAs (5-10 g of 2:1:1) sipped intra-workout may modestly reduce perceived exertion and central fatigue; no clear muscle synthesis benefit.
- Older adult (60+): 1.2-1.6 g/kg/day total protein, with at least 30 g of high-quality protein per meal to overcome anabolic resistance. Leucine fortification (e.g., 2-3 g leucine added per meal) has been tested with mixed results; balanced BCAA or whole-protein approach is preferable.
- Cirrhosis / hepatic encephalopathy: under medical supervision, BCAA-enriched formulas (Marchesini protocol) at 0.25 g/kg/day BCAA in 2:1:1 ratio, divided into evening dose to maintain overnight nitrogen balance.
A practical sanity check: if you are eating a varied diet that includes any combination of meat, fish, eggs, dairy, legumes, soy, or quinoa providing your total daily protein target, you are getting more than enough valine. Isolated valine supplements (sold as a standalone amino acid) are essentially never warranted outside of metabolic disorder management.
Key Research Papers
- Harper AE, Benevenga NJ, Wohlhueter RM (1970). Effects of ingestion of disproportionate amounts of amino acids. Physiological Reviews. — PubMed
- Moberg M et al. (2016). Activation of mTORC1 by leucine is potentiated by branched-chain amino acids and even more so by essential amino acids following resistance exercise. American Journal of Physiology — Cell Physiology. — PubMed
- Wolfson RL et al. (2016). Sestrin2 is a leucine sensor for the mTORC1 pathway. Science. — PubMed
- Fouré A, Bendahan D (2017). Is branched-chain amino acids supplementation an efficient nutritional strategy to alleviate skeletal muscle damage? A systematic review. Nutrients. — PubMed
- Jackman SR et al. (2017). Branched-chain amino acid ingestion stimulates muscle myofibrillar protein synthesis following resistance exercise in humans. Frontiers in Physiology. — PubMed
- Plotkin DL et al. (2021). Isolated leucine and branched-chain amino acid supplementation for enhancing muscular strength and hypertrophy: a narrative review. International Journal of Sport Nutrition and Exercise Metabolism. — PubMed
- Wilkinson DJ et al. (2013). Effects of leucine and its metabolite beta-hydroxy-beta-methylbutyrate on human skeletal muscle protein metabolism. Journal of Physiology. — PubMed
- Drummond MJ, Rasmussen BB (2008). Leucine-enriched nutrients and the regulation of mammalian target of rapamycin signalling and human skeletal muscle protein synthesis. Current Opinion in Clinical Nutrition and Metabolic Care. — PubMed
- Phillips SM (2017). Current concepts and unresolved questions in dietary protein requirements and supplements in adults. Frontiers in Nutrition. — PubMed
- Wagenmakers AJ (1998). Muscle amino acid metabolism at rest and during exercise: role in human physiology and metabolism. Exercise and Sport Sciences Reviews. — PubMed
- Volpi E et al. (2003). Essential amino acids are primarily responsible for the amino acid stimulation of muscle protein anabolism in healthy elderly adults. American Journal of Clinical Nutrition. — PubMed
- Bauer J et al. (2013). Evidence-based recommendations for optimal dietary protein intake in older people: a position paper from the PROT-AGE Study Group. JAMDA. — PubMed
PubMed Topic Searches
- PubMed: BCAA ratio and muscle synthesis
- PubMed: Harper BCAA antagonism
- PubMed: Sestrin2 leucine sensing
- PubMed: Valine and muscle protein synthesis
- PubMed: BCAA and sarcopenia
Connections
- Valine Overview
- Valine Benefits Hub
- Valine for Energy Metabolism
- Valine for Cognitive Performance
- Valine for Nitrogen Balance & Wound Healing
- Leucine (BCAA Partner)
- Isoleucine (BCAA Partner)
- Glutamine
- Alanine
- Arginine
- All Amino Acids
- Eggs
- Exercise
- Fatigue