Carnitine, Fat Metabolism & Weight: An Honest Look
This is the most important honest correction in the entire Carnitine section. Carnitine is genuinely required to transport fat into mitochondria to be burned — that fact is undisputed and is why it sells so well as a "fat burner." But being required for a process is not the same as controlling its speed. In healthy, well-nourished people, muscle carnitine is already saturated, endogenous synthesis covers any gap, and adding more does not accelerate fat loss. The controlled weight-loss trials confirm this: the pooled effect is small, the studies are of low-to-moderate quality, and much of the apparent benefit comes from special populations (people with obesity, fatty liver, or metabolic disease) rather than from carnitine acting as a fat-melting supplement. If a product promises that carnitine will "torch" your body fat, the science does not support it.
Interactive Visualization Fat Burning & Ketosis — what actually happens Follow a fatty acid out of a fat cell to the mitochondrial gate and find it padlocked by insulin. Drop the carbs, open CPT1, and watch the liver start making ketones. Launch →
Table of Contents
- The "Fat Burner" Claim and Where It Comes From
- Necessary Is Not the Same as Rate-Limiting
- Why Healthy People Are Already Saturated
- What the Weight-Loss Meta-Analyses Actually Show
- Reading the Small "Positive" Effect Honestly
- Where a Genuine Deficiency Changes the Picture
- Special Populations Worth Distinguishing
- Fat Oxidation During Exercise vs Weight Loss Over Time
- Honest Bottom Line & Practical Guidance
- Key Research Papers
- Connections
- Featured Videos
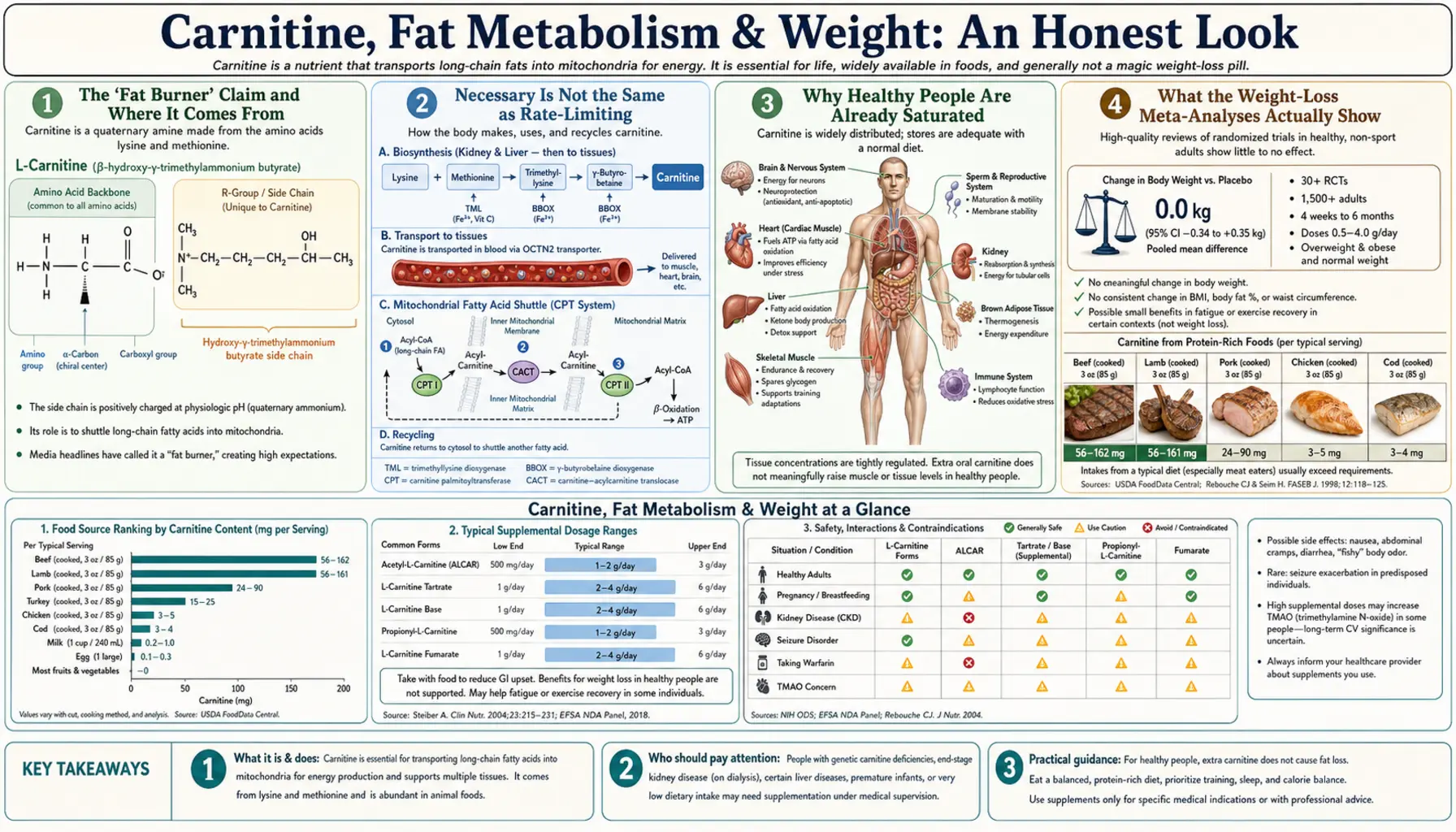
The "Fat Burner" Claim and Where It Comes From
Walk down any supplement aisle and carnitine is sold as a fat-loss aid, often paired with promises about "boosting metabolism" and "turning fat into energy." The claim is not invented from nothing — it grows out of a real and correct piece of biochemistry. As detailed on the Benefits hub, long-chain fatty acids cannot enter the mitochondrion to be oxidized unless carnitine carries them across the inner membrane. No carnitine, no long-chain fat burning. That is textbook and true.
The marketing then makes a leap that sounds reasonable but is biologically wrong: if carnitine is the gatekeeper for fat burning, adding more carnitine should open the gate wider and burn more fat. This is the single most common error in supplement reasoning, and unpacking it is the whole point of this page.
Necessary Is Not the Same as Rate-Limiting
Think of a busy highway toll plaza. The toll booths are necessary — no car reaches the highway without passing one. But if the booths already have more open lanes than there are cars, building extra booths does nothing to speed up traffic. The bottleneck is the number of cars arriving, the highway's capacity downstream, or the on-ramp — not the booths, which have spare capacity sitting idle.
Carnitine in a healthy person is exactly that over-built toll plaza. The carnitine shuttle has far more capacity than the muscle's normal rate of fat oxidation demands. The actual limits on how much fat you burn are set elsewhere: total energy balance (calories in versus out), exercise intensity and duration, mitochondrial density, hormone levels (insulin, catecholamines, thyroid), and how much fat is being released from fat cells in the first place. Carnitine sits downstream of all of these with room to spare. Adding more toll booths — more carnitine — cannot pull more cars onto the highway.
This is the same principle that governs the exercise-and-recovery story. A nutrient produces a benefit only where its supply is genuinely limiting the outcome. Fat burning in a well-fed adult is not carnitine-limited, so supplementing it does not increase fat loss.
Why Healthy People Are Already Saturated
Three facts converge to keep a healthy person's carnitine status full without any supplement:
- The body makes its own. Roughly a quarter of your carnitine is synthesized in the liver and kidneys from lysine and methionine, with the rate adjusting to need. A shortfall in diet is largely compensated internally.
- The kidney is a tight recycler. Healthy kidneys reabsorb over 90% of filtered carnitine, so the body holds onto what it has rather than wasting it.
- Muscle uptake is capped. As covered on the exercise page, skeletal muscle carnitine barely moves in response to oral supplements unless a demanding insulin-spiking, high-carbohydrate loading protocol is followed for months. You cannot simply "top up" the tissue that would need to change for fat burning to increase.
Put together, these mean that for an omnivorous, healthy adult, tissue carnitine is essentially maxed out already. There is no empty tank for a supplement to fill, and therefore no metabolic lever for it to pull.
What the Weight-Loss Meta-Analyses Actually Show
Two systematic reviews are usually cited in this debate, and reading them carefully is far more useful than reading any product label.
Pooyandjoo et al. (Obesity Reviews, 2016) pooled nine randomized controlled trials of L-carnitine and reported that, on average, the carnitine groups lost about 1.3 kg (roughly 3 pounds) more than control groups. At first glance that looks like a win. But the authors themselves flagged that the effect shrank over time, that the trials were heterogeneous, and — crucially — that many participants were people with obesity or metabolic conditions, not healthy-weight adults. A three-pound average difference, concentrated in metabolically compromised people and fading with longer follow-up, is not the "fat-torching" effect the supplement industry implies.
Talenezhad et al. (Clinical Nutrition ESPEN, 2020) looked more broadly at weight and body composition across 37 trials. It found a statistically significant but small reduction in body weight, body-mass index, and fat mass with carnitine — while explicitly rating the overall quality of evidence as low to moderate and noting that effects were most apparent in specific subgroups (again, people with overweight, obesity, or related metabolic disease). The authors stopped well short of endorsing carnitine as a general weight-loss agent.
The honest reading of both papers is the same: any measurable effect is small, uncertain, and concentrated in metabolically unhealthy populations — not evidence that carnitine burns fat in an average, well-nourished person trying to lean out.
Reading the Small "Positive" Effect Honestly
When a meta-analysis of supplements shows a small positive number, good skepticism asks four questions before believing it:
- Who was studied? If the effect lives in people with obesity, fatty liver, or type 2 diabetes, it may reflect correcting a relative carnitine shortfall in metabolically stressed tissue — not a fat-loss mechanism available to healthy dieters. This is exactly the pattern in the carnitine trials.
- How large is "significant"? Statistical significance is not clinical meaning. A one-to-three-pound average difference, often over many weeks, is within the noise of ordinary diet adherence and water-weight fluctuation.
- How good were the trials? Both major reviews rated the evidence low-to-moderate quality, with risk of bias and heterogeneity. Low-quality trials tend to overstate effects, which regress toward null as better studies appear.
- Was diet controlled? Many trials combined carnitine with calorie restriction or exercise. Attributing the weight change to carnitine rather than to the diet-and-exercise program is a classic confound.
Apply these filters and the carnitine weight-loss literature deflates from "proven fat burner" to "possible small effect in specific patients, uncertain quality, easily confounded." That is the accurate description.
Where a Genuine Deficiency Changes the Picture
None of this means carnitine is inert. It means the benefit requires a genuine shortfall — a tank that is actually low. In true carnitine deficiency, restoring supply is unambiguously therapeutic, and metabolism can improve substantially. Deficiency states include:
- Primary carnitine deficiency — an inherited defect in the OCTN2 transporter that prevents tissues from taking up carnitine; a serious medical condition requiring lifelong supplementation.
- Secondary deficiency from certain medications (notably valproic acid and some antibiotics like pivmecillinam), hemodialysis (which strips carnitine from the blood), severe malabsorption, and some inborn metabolic errors.
- Marginal status in strict vegetarians and vegans, who get little dietary carnitine — though healthy plant-based eaters usually maintain adequate levels through efficient synthesis and renal conservation, so routine supplementation is not automatically needed.
The key distinction is medical, not cosmetic. Carnitine corrects deficiency; it does not create a metabolic advantage where none is lacking.
Special Populations Worth Distinguishing
A few groups sit between "healthy and saturated" and "frankly deficient," and they are where the modest trial signals cluster:
- Obesity and insulin resistance. Metabolically stressed muscle and liver may have relatively lower functional carnitine and impaired fat oxidation. This is the most plausible explanation for why the meta-analytic effect concentrates here — carnitine may partly restore a blunted process rather than super-charge a normal one.
- Non-alcoholic fatty liver disease (NAFLD). Some trials suggest carnitine may improve liver enzymes and fat handling in NAFLD, again likely by supporting impaired hepatic fat oxidation rather than by general fat burning.
- Type 2 diabetes. Carnitine and acetyl-L-carnitine have been studied for insulin sensitivity and diabetic complications with mixed results; the neuropathy data (acetyl-L-carnitine) are covered on the Forms & TMAO page.
- Older adults. Carnitine status and mitochondrial fat oxidation decline with age; small trials suggest carnitine may reduce fatigue and modestly improve body composition in the elderly — a distinct scenario from a young, healthy person seeking fat loss.
Fat Oxidation During Exercise vs Weight Loss Over Time
A subtle point trips up many discussions: even if a supplement nudged fat oxidation during a single workout, that would not automatically produce fat loss over weeks. Body-fat change is governed by total energy balance across days and months. Burning a slightly higher fraction of fat during one hour of exercise, while glucose gets burned more later, nets out to little difference in stored fat if total calories are unchanged. The body defends its energy stores through many compensatory mechanisms.
This is why the acute "fat oxidation" studies so often cited in marketing do not translate into the weight-loss numbers people expect — and why even the honest, months-long muscle-loading protocol from the exercise page shifts fuel selection without turning carnitine into a weight-loss drug. Fat loss is won at the level of sustained calorie deficit, protein intake, sleep, and consistent activity — not by shuttling a bit more fat into an already-unlimited mitochondrial gate.
Honest Bottom Line & Practical Guidance
- For a healthy person seeking weight loss: carnitine is not a proven fat burner. Expect little to nothing beyond what diet and exercise deliver. Spend your money and attention on a sustainable calorie deficit, adequate protein, and consistent movement.
- For people with obesity, NAFLD, or metabolic disease: there is a small, uncertain signal of benefit, best pursued as part of medical care rather than as a standalone product.
- For genuine deficiency (inherited, dialysis, valproate, severe malabsorption): supplementation is medically indicated and can be important — this is a diagnosis-driven use, not a wellness purchase.
- Whole-food context: if you want dietary carnitine, red meat and dairy such as beef and milk are the richest sources — but eating them for carnitine specifically is unnecessary for most people.
- Safety and the gut question: doses used in trials (often 2–3 g/day) are generally well tolerated; the microbiome-and-TMAO consideration is covered on the Forms & TMAO page.
The most valuable thing this page can give you is a filter: whenever a supplement is sold because it is "necessary" for a desirable process, ask whether it is actually the limiting factor for you. For carnitine and fat loss in healthy people, it is not. This is educational information, not medical advice.
Key Research Papers
- Pooyandjoo M, Nouhi M, Shab-Bidar S, Djafarian K, Olyaeemanesh A (2016). The effect of (L-)carnitine on weight loss in adults: a systematic review and meta-analysis of randomized controlled trials. Obesity Reviews. — PubMed 27335245
- Talenezhad N, Mohammadi M, Ramezani-Jolfaie N, Mozaffari-Khosravi H, Salehi-Abargouei A (2020). Effects of l-carnitine supplementation on weight loss and body composition: a systematic review and meta-analysis of randomized controlled clinical trials. Clinical Nutrition ESPEN. — PubMed 32359762
- Wall BT, Stephens FB, Constantin-Teodosiu D, Marimuthu K, Macdonald IA, Greenhaff PL (2011). Chronic oral ingestion of L-carnitine and carbohydrate increases muscle carnitine content and alters muscle fuel metabolism during exercise in humans. Journal of Physiology. — PubMed 21224234
- Stephens FB, Constantin-Teodosiu D, Greenhaff PL (2007). New insights concerning the role of carnitine in the regulation of fuel metabolism in skeletal muscle. Journal of Physiology. — PubMed 17331998
- Malaguarnera M et al. (2007). L-Carnitine treatment reduces severity of physical and mental fatigue and increases cognitive functions in centenarians. American Journal of Clinical Nutrition. — PubMed 18065594
PubMed Topic Searches
- PubMed: Carnitine weight-loss trials
- PubMed: Carnitine body composition
- PubMed: Carnitine fat oxidation in obesity
- PubMed: Carnitine and NAFLD
- PubMed: Primary carnitine deficiency
- PubMed: Carnitine and insulin resistance
External Resources
- NIH Office of Dietary Supplements — Carnitine (Weight Loss section)
- Linus Pauling Institute — L-Carnitine
- MedlinePlus — L-Carnitine (uses and evidence)
Connections
- Fat Burning & Ketosis — interactive animation
- Carnitine Benefits Hub
- Carnitine (Main Page)
- Exercise & Recovery
- Forms & the TMAO Question
- Lysine (Precursor)
- Methionine (Precursor)
- All Amino Acids
- Type 2 Diabetes
- Mediterranean Diet
- Exercise
- Beef (Dietary Source)
- Milk (Dietary Source)
- Avocado
- Iron (Carnitine Synthesis)
- Vitamin C (Carnitine Synthesis)