Realistic Weight Loss: Setting Expectations That Work
Most weight-loss attempts do not fail because of a bad diet. They fail because of a bad expectation — a number in your head that no honest plan could ever hit, set too high and too fast, so that when reality falls short you conclude the effort is not working and quit. This page is about fixing that first. It is not a diet and it is not a pep talk; it is an evidence-based reset of what real, healthy weight change actually looks like week to week. You will find the pace the science supports, the surprisingly small amount of weight loss that produces large health gains, why the scale lies to you in the first week and stalls in the middle, and how to read the many signals of progress that have nothing to do with a number. The goal is simple and kind: to replace the fantasy that sets people up to quit with a realistic picture that lets people keep going. If you have tried and struggled before, this is written for you, without shame — because the truth is more encouraging than the hype ever was.
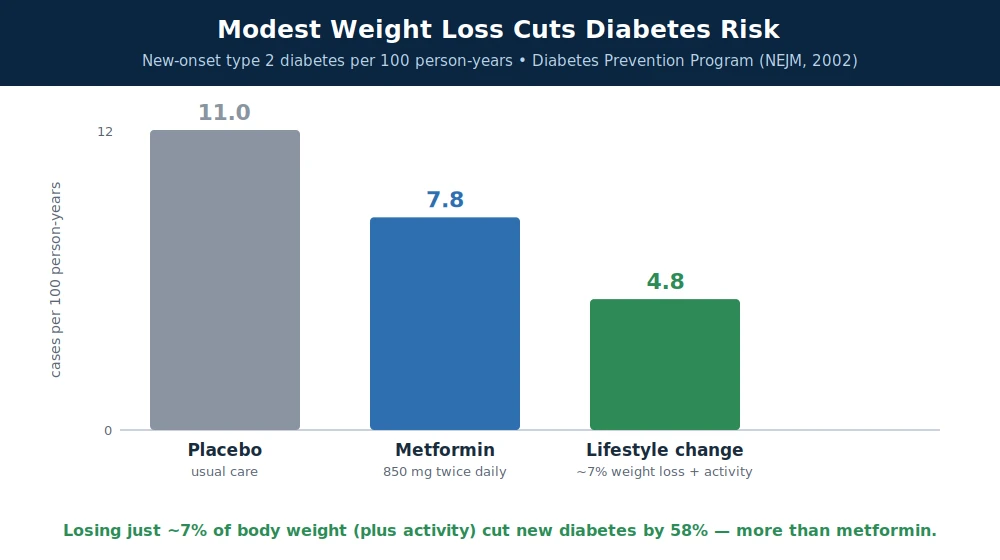
Table of Contents
- Why Unrealistic Expectations Set You Up to Quit
- A Healthy Pace: About 1 to 2 Pounds a Week
- The 5–10% That Changes Everything
- The Week-One "Whoosh" and Why Early Numbers Mislead
- Plateaus: Why They Happen and What to Do
- Non-Scale Victories and the Noisy Scale
- Escaping All-or-Nothing Thinking
- Sleep, Stress, and Mental Health
- Body Respect: Health Across a Range of Sizes
- When to Get Help: Clinicians, Dietitians, and Real Tools
- What Realistic Success Actually Looks Like
- Research Papers
- Connections
- Featured Videos
Why Unrealistic Expectations Set You Up to Quit
Start with the trap almost everyone falls into. When people begin a weight-loss effort, they usually carry a private target in their head, and research shows that target is often wildly out of reach. In a now-classic study, Gary Foster and colleagues asked people entering an obesity treatment program to name their "goal weight," their "dream weight," and the weight they would be "disappointed" to end at. On average, participants defined a disappointing outcome as losing about 17% of their body weight — a result that good clinical programs are proud to achieve. Their "dream" figure was roughly a 38% loss, which almost no treatment produces. In other words, they had pre-labeled success as failure before they began.
This matters enormously, because expectations are not harmless. If you decide in advance that a 10- or 15-pound loss "doesn't count," then when you actually lose 10 or 15 pounds — a genuine, health-improving achievement — your own mind reads it as proof that the effort is not working. That is the moment most people quit, not because their plan failed, but because it "only" delivered a realistic result. The fantasy did the damage, not the diet.
There is also a media problem behind the fantasy. The weight-loss stories that go viral are, by definition, the extreme ones: dozens of pounds in weeks, dramatic before-and-after photos, "I tried X for 30 days." These are selected because they are unusual. Comparing your ordinary, healthy progress against a highlight reel of outliers is a setup for feeling like a failure while actually succeeding. The single most useful thing you can do before changing what you eat is to change the number you are aiming for — to something a real body, over real time, can actually reach and hold.
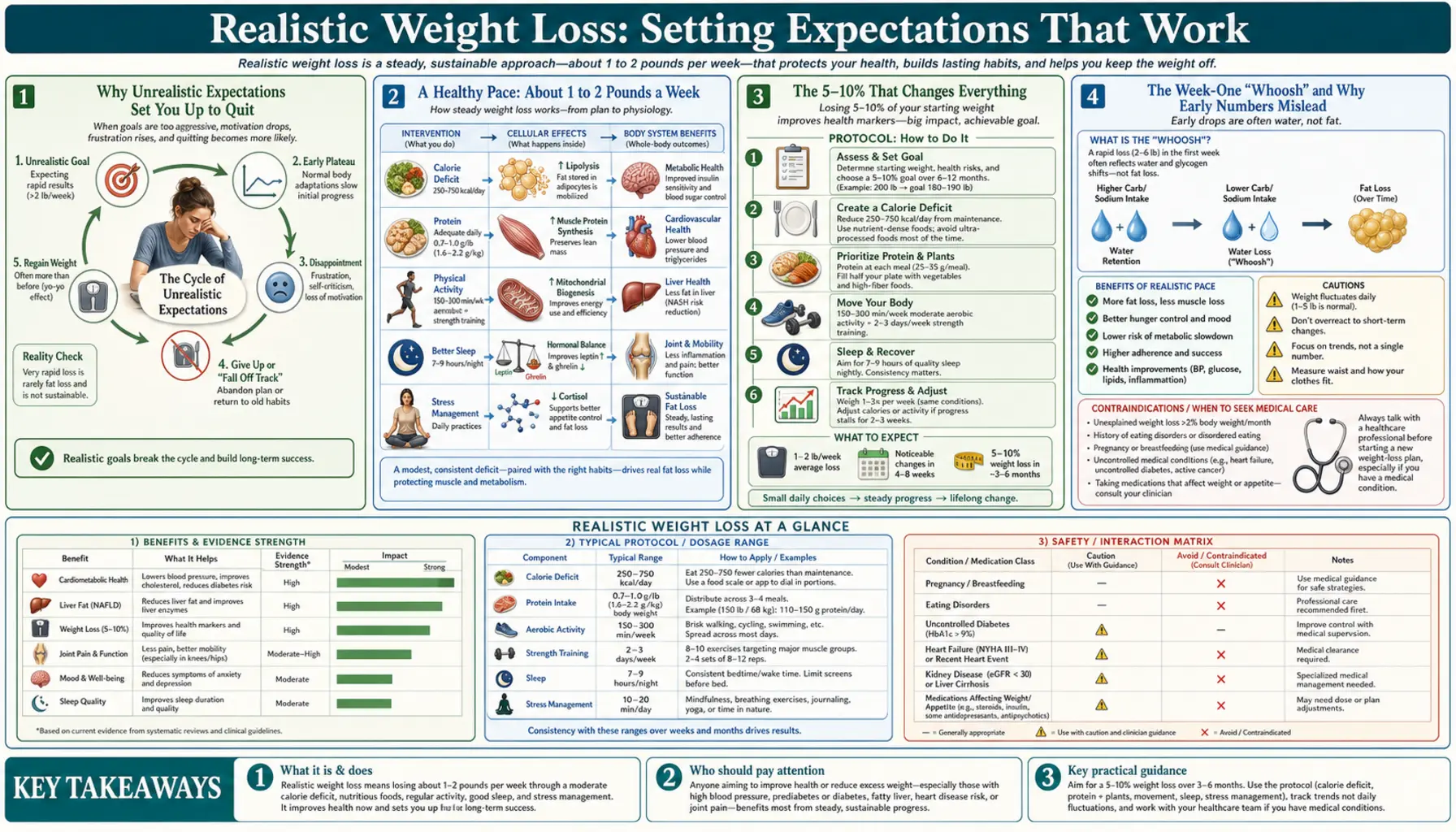
A Healthy Pace: About 1 to 2 Pounds a Week
So what is realistic? For most people, a sustainable pace of weight loss is roughly 0.5 to 1 kilogram — about 1 to 2 pounds — per week. This is the range major clinical guidelines point to, and the 2013 American Heart Association / American College of Cardiology / The Obesity Society guideline describes lifestyle programs that produce this kind of steady loss as the foundation of treatment. It sounds modest. Over a year, though, 1 to 2 pounds a week adds up to a large, meaningful change — and, crucially, a change your body and your life can actually keep.
Why not go faster? Faster is tempting, and the early scale drop from a crash approach is real. But most of what disappears in a very rapid loss is not the thing you want gone. A large share of fast early loss is water (more on that below), and aggressive, very-low-calorie dieting also tends to burn through lean muscle alongside fat. Losing muscle is doubly counterproductive: muscle is metabolically active tissue, so losing it lowers the calories you burn at rest, making the weight easier to regain and harder to lose next time.
The honest picture on speed is a little more nuanced than "slow and steady always wins." In a well-designed randomized trial, Katrina Purcell and colleagues compared rapid versus gradual weight loss and found that people in the rapid arm were actually more likely to reach their target — but both groups regained weight at a similar rate afterward, showing that how fast you take it off does not, by itself, determine whether it stays off. The reason to favor a moderate pace is not that speed is magic in reverse; it is that a moderate pace is more livable, better protects muscle, is easier to fuel with adequate nutrition, and does not depend on extreme restriction you cannot sustain. Aim for a pace you could imagine keeping for months, not one you are white-knuckling for a week.
The 5–10% That Changes Everything
Here is the single most under-appreciated fact in all of weight management, and it deserves to be shouted from the rooftops: you do not need to reach an "ideal" weight to get most of the health benefits. Losing just 5 to 10 percent of your body weight produces major improvements. For a 200-pound person, 5–10% is only 10 to 20 pounds — well inside the realistic range described above.
This is not wishful thinking; it is one of the best-replicated findings in the field. In an influential early analysis, George Blackburn laid out how a modest 5–10% loss meaningfully improves blood pressure, blood sugar, and cholesterol. Later large trials nailed it down. The landmark Diabetes Prevention Program (Knowler and colleagues) randomized more than 3,000 adults at high risk for type 2 diabetes; those in the lifestyle arm lost an average of about 7% of their body weight and cut their risk of developing diabetes by 58% — a bigger effect than the medication arm. A modest, realistic loss did what a drug could not.
The Look AHEAD trial, in people who already had type 2 diabetes, adds both encouragement and honesty. Rena Wing and colleagues showed that an intensive lifestyle program producing modest weight loss improved cardiovascular risk factors across the board — better blood sugar (lower HbA1c), blood pressure, and HDL cholesterol — and those who lost more saw larger gains. The honest footnote, reported by the Look AHEAD Research Group, is that over roughly a decade the program did not reduce the rate of heart attacks and strokes compared with standard care, even though it improved almost every risk factor and helped many people reduce medications, improve mobility, and achieve diabetes remission. The takeaway is realistic on both sides: a 5–10% loss reliably improves how your body is running — blood pressure, blood sugar, cholesterol, joint pain, sleep apnea, mobility — and that is a genuine victory worth having, even if it is not a cure for everything.
Reframe your goal around this. Instead of "I need to lose 60 pounds," a realistic and powerful first target is "I would like to lose about 5–10% and feel the difference." That target is reachable, its benefits are proven, and hitting it builds the confidence to keep going.
The Week-One "Whoosh" and Why Early Numbers Mislead
Almost everyone who cuts calories sees a dramatic drop on the scale in the first week — sometimes 4, 6, even 8 pounds. It feels fantastic, and it sets a mental pace ("if this keeps up, I'll lose 30 pounds in a month!") that no one can maintain. Understanding what that early "whoosh" actually is will save you from the crushing disappointment that arrives in week two.
Most of that first-week loss is water, not fat. Your body stores carbohydrate as glycogen in your liver and muscles, and each gram of glycogen is bound to roughly 3 to 4 grams of water. When you eat less — and especially when you cut carbohydrates — you burn through those glycogen stores, and the water they were holding is released and excreted. Cutting back on salt has a similar quick effect on water retention. The result is a fast, real, but largely fat-free drop on the scale. It is also why that pace cannot continue: once the glycogen-water buffer is gone, the scale settles down to the slower, steadier rate of actual fat loss.
This has two practical consequences. First, do not extrapolate from week one. The 1-to-2-pounds-a-week figure describes fat loss after the initial water shift, and that is the number to plan around. Second, do not panic when the same thing runs in reverse. If you have a high-carbohydrate or salty weekend, your body will re-store glycogen and water, and the scale can jump several pounds overnight. That is not fat regain — you did not eat 10,000 surplus calories — it is water. The early scale is loud and misleading in both directions. Judge your progress over weeks, not days.
Plateaus: Why They Happen and What to Do
Sooner or later, almost everyone who loses weight hits a plateau — a stretch where the scale simply stops moving even though nothing has obviously changed. This is one of the most demoralizing moments in the whole process, and it drives a lot of people to give up right before things would have kept improving. It helps enormously to understand that a plateau is normal, expected, and physiological — not a sign that you are doing something wrong.
Two forces are at work. The first is simple arithmetic. As Kevin Hall and colleagues have shown in careful models of human energy balance, a smaller body burns fewer calories. A 200-pound body needs more energy just to exist and move than a 180-pound body does. So the calorie intake that once created a deficit — and drove weight down — gradually becomes the amount that merely maintains your new, lighter weight. You have not failed; your target has moved. This also means weight loss naturally decelerates and levels off long before you might expect, which their work quantifies precisely.
The second force is metabolic adaptation (sometimes called adaptive thermogenesis): in response to weight loss and reduced intake, the body becomes somewhat more energy-efficient and burns a bit fewer calories than its new size alone would predict. A striking illustration came from Erin Fothergill and colleagues, who followed contestants from The Biggest Loser and found that their resting metabolism remained suppressed years later. That study involved extreme, rapid loss, so it is the dramatic end of the spectrum — but a gentler version of the same adaptation is part of why plateaus happen to everyone.
So what do you do? Not panic, and not crash-diet harder. Sensible responses include: giving it time (weight often resumes falling on its own after a stall of a few weeks); tightening up on portion "creep" that quietly returns as motivation dips; adding or increasing physical activity, especially resistance/strength training, which helps preserve the calorie-burning muscle that metabolic adaptation threatens; making sure you are getting enough protein and sleep; and — importantly — recognizing that a plateau can also be your body's signal that you have reached a reasonable, defensible weight. Sometimes the healthiest move is to shift from losing to maintaining for a while, then reassess. A plateau is not the end of progress; it is a normal chapter in it.
Non-Scale Victories and the Noisy Scale
If you measure your success only by the number on the scale, you are using a single noisy instrument to track a rich, multi-dimensional change — and you will often feel like you are losing when you are actually winning. The scale is worth using, but it needs to be understood for what it is.
First, the scale is noisy from day to day for reasons that have nothing to do with fat. Your weight swings with the water in your body, and that water responds to salt intake, carbohydrate intake, hormones (many women see a clear premenstrual rise of a few pounds), how recently you ate or drank, whether you have had a bowel movement, hard exercise the day before (sore muscles hold water as they repair), and even the weather. A 2-to-4-pound wobble between mornings is completely normal and is not fat gained or lost. This is why weighing yourself once and reacting is a recipe for whiplash. The research on self-weighing (reviewed by Yaguang Zheng and colleagues) suggests that regular weighing can support weight management — but the value comes from watching the trend over weeks, not from any single reading. If you weigh, weigh under consistent conditions (say, first thing in the morning) and pay attention to the moving average, not the daily blip.
Second, and more important: the scale cannot see most of what is actually improving. These are your non-scale victories, and they are often better proof of real change than pounds are:
- Energy and stamina — climbing stairs without getting winded, playing with kids or grandkids, getting through the afternoon without crashing.
- Fitness — walking farther, lifting more, moving more easily; strength and endurance you can feel.
- How your clothes fit — a belt on a new notch, a shirt that buttons comfortably. Because muscle is denser than fat, you can lose inches and change shape even when the scale is quiet.
- Lab numbers — lower blood pressure, better blood sugar and HbA1c, improved cholesterol, less fat on the liver. These are the health wins that matter most, and they often improve early.
- Sleep, mood, and joints — less snoring or sleep apnea, steadier mood, less knee and back pain, easier movement.
Keep a short list of these. On the weeks the scale stalls or ticks up, your non-scale victories are the honest evidence that your body is still getting healthier — and they are usually the changes you actually wanted in the first place.
Escaping All-or-Nothing Thinking
Perhaps the single most destructive habit in weight management is all-or-nothing thinking — the belief that you are either "on the plan" (perfect) or "off it" (failed), with nothing in between. It sounds like this: "I already ate the cookie, so the day is ruined — I'll start again Monday." One 200-calorie slip becomes a 2,000-calorie evening, then a lost week, then a lost month, then abandoning the effort entirely. The cookie was never the problem. The spiral was.
The math makes the trap obvious. A single off-plan meal, or even an off-plan day, is a rounding error against weeks and months of overall pattern. What actually determines your results is what you do most of the time, not whether any given day was flawless. Nobody eats perfectly, and no successful long-term "loser" ever did. The people who keep weight off are not the ones who never slip — they are the ones who slip and then simply resume, without the detour through guilt and self-punishment.
Practically, this means replacing the "I blew it" reflex with a boring, powerful rule: the very next choice is the only one that matters. Ate more than you meant to at lunch? The next meal is a normal, sensible meal — not a punishment fast, and not a "well, might as well" write-off. Progress is not a light switch that is either on or off; it is a dial, and one imperfect meal barely moves it. Aiming for "good enough, most of the time" is not a compromise on your goal — for almost everyone, it is the goal, because it is the only version that can be sustained for life.
Sleep, Stress, and Mental Health
Weight is not governed by willpower and forks alone. Two everyday factors — sleep and stress — quietly shape hunger, cravings, and even the composition of what you lose, and ignoring them makes an otherwise good plan much harder than it needs to be.
Sleep is the one people most often overlook. In a tightly controlled study, Arlet Nedeltcheva and colleagues put dieters on the same calorie-reduced plan but varied their sleep. When participants were short on sleep, a much larger fraction of the weight they lost came from lean tissue rather than fat, and they reported more hunger. Short sleep also nudges appetite hormones toward eating more and makes high-calorie foods more tempting the next day. In practical terms, skimping on sleep can partly undo the very effort you are making. Protecting 7 to 9 hours is not a luxury add-on to weight management; it is part of the plan.
Stress works in a parallel way. Ongoing stress raises cortisol, drives many people toward calorie-dense "comfort" foods, and disrupts sleep — a self-reinforcing loop. This is not a character flaw; it is physiology plus a food environment engineered to be soothing. That is also why practices that lower the stress load — a daily walk, breathing or meditation, time outdoors, connection with other people, or simply a realistic schedule — can support weight goals indirectly but powerfully. And when low mood, anxiety, or a difficult relationship with food is part of the picture, treating that — not just the diet — is often the missing piece. Mental health and metabolic health are not separate projects.
Body Respect: Health Across a Range of Sizes
A page about realistic expectations would be dishonest if it implied that health lives at only one number on the scale. It does not. Health is possible — and improvable — across a genuine range of body sizes, and your worth as a person has nothing to do with any of them.
This is not a soft sentiment; it is practical. Shame is a terrible long-term motivator. The evidence on weight stigma — being judged, blamed, or mistreated because of body size — shows that it does not spur healthy change; it does the opposite. Stigma is associated with more stress, more disordered and emotional eating, avoidance of exercise and even of medical care, and worse mental health. If berating ourselves worked, it would have worked by now. The healthier and more effective stance is body respect: caring for the body you have today — feeding it well, moving it, sleeping, managing stress, getting recommended screenings — regardless of where it currently sits on the scale.
Framed this way, weight loss becomes one possible tool for feeling and functioning better, not a moral test you are passing or failing. Many of the biggest wins — more energy, better blood pressure and blood sugar, stronger mood, less pain, better sleep — can begin well before you reach any "goal weight," and some are available through better habits even without much weight change at all. Treating your body as something to care for rather than something to punish is not giving up on your goals. For most people, it is what finally makes those goals reachable.
When to Get Help: Clinicians, Dietitians, and Real Tools
Trying to do everything alone, from willpower and internet advice, is the hard way — and for many people it is not the way that works. Weight regulation is biological, and struggling with it is not a personal weakness any more than needing glasses is. Reaching for real support is a smart, grown-up move, not an admission of defeat.
The most effective non-surgical approach is not a fad; it is structured behavioral weight management. As Thomas Wadden and colleagues summarize, comprehensive lifestyle programs — combining eating changes, physical activity, and behavioral skills like self-monitoring, goal-setting, and problem-solving, ideally with regular check-ins — reliably produce clinically meaningful weight loss. A registered dietitian can build an eating pattern that fits your life, budget, and preferences instead of a generic template you will abandon. A primary-care clinician can check for and treat conditions that make weight loss harder (such as thyroid problems or medication side effects) and monitor the health markers that are improving.
There are also legitimate medical tools for people who need them. The 2013 AHA/ACC/TOS obesity guideline lays out a stepped approach: lifestyle change for everyone, with the option of FDA-approved anti-obesity medications or, for people with more severe obesity or serious weight-related conditions, bariatric surgery. Modern medications, including the newer options that have changed the field, can be appropriate and effective for the right person under medical supervision. Using them is not "cheating" any more than using medication for blood pressure is; obesity is a chronic medical condition, and treating it medically is reasonable care. Consider reaching out for help if you have significant weight to lose, weight-related health problems (diabetes, high blood pressure, sleep apnea, joint disease), a history of losing and regaining, or a difficult relationship with food. The right kind of help can turn an exhausting solo battle into a manageable, supported plan.
What Realistic Success Actually Looks Like
Pulling it all together, here is a picture of success that is honest, achievable, and worth wanting — the opposite of the fantasy this page began by dismantling:
- A sane pace. Roughly 1 to 2 pounds a week after the first-week water shift, not a crash. Steady beats dramatic because steady is what stays.
- A modest, powerful target. A first goal of losing about 5–10% of your body weight — enough to meaningfully improve blood pressure, blood sugar, cholesterol, joint pain, and sleep, and enough to build real confidence.
- Weeks-not-days vision. Ignoring the daily scale noise and the week-one whoosh, watching the trend, and treating plateaus as a normal chapter rather than a failure.
- Progress you can feel. Counting non-scale victories — energy, fitness, how clothes fit, lab numbers, sleep, mood — as the real evidence they are.
- Resilience over perfection. Abandoning all-or-nothing thinking; letting one off-plan meal be exactly that, and resuming with the very next choice.
- The whole person. Protecting sleep, managing stress, tending to mental health, and respecting your body at its current size — because those are what make the eating and moving sustainable.
- Help when you need it. Leaning on clinicians, dietitians, structured programs, and, where appropriate, legitimate medical tools — without shame.
A last, gentle word. Lasting weight change is genuinely hard, and it is shaped by biology, sleep, stress, hormones, medications, income, and a food environment built to be over-eaten — not by willpower alone and never by moral failing. If you have tried many times and struggled, you are in very good company, and it is not your fault. The most encouraging fact in this entire field is also the most realistic one: you do not need a dramatic transformation to get most of the benefits. A modest, steady, sustainable change — kept up with patience and self-respect — is not a consolation prize. It is the actual win.
Research Papers
- Foster GD, Wadden TA, Vogt RA, Brewer G. What is a reasonable weight loss? Patients' expectations and evaluations of obesity treatment outcomes. Journal of Consulting and Clinical Psychology. 1997;65(1):79-85. doi:10.1037/0022-006x.65.1.79 — the classic study showing patients define even a 17% weight loss as "disappointing," documenting how unrealistic expectations undermine treatment.
- Purcell K, Sumithran P, Prendergast LA, Bouniu CJ, Delbridge E, Proietto J. The effect of rate of weight loss on long-term weight management: a randomised controlled trial. The Lancet Diabetes & Endocrinology. 2014;2(12):954-962. doi:10.1016/S2213-8587(14)70200-1 — rapid and gradual weight loss led to similar regain, showing pace alone does not determine whether weight stays off.
- Blackburn G. Effect of degree of weight loss on health benefits. Obesity Research. 1995;3(Suppl 2):211S-216S. doi:10.1002/j.1550-8528.1995.tb00466.x — foundational argument that a modest 5–10% weight loss meaningfully improves blood pressure, blood sugar, and lipids.
- Knowler WC, Barrett-Connor E, Fowler SE, et al; Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. New England Journal of Medicine. 2002;346(6):393-403. doi:10.1056/NEJMoa012512 — a ~7% lifestyle weight loss cut progression to diabetes by 58%, outperforming medication.
- Wing RR, Lang W, Wadden TA, et al; Look AHEAD Research Group. Benefits of modest weight loss in improving cardiovascular risk factors in overweight and obese individuals with type 2 diabetes. Diabetes Care. 2011;34(7):1481-1486. doi:10.2337/dc10-2415 — even modest weight loss improved blood sugar, blood pressure, and HDL cholesterol, with larger losses giving larger gains.
- The Look AHEAD Research Group. Cardiovascular effects of intensive lifestyle intervention in type 2 diabetes. New England Journal of Medicine. 2013;369(2):145-154. doi:10.1056/NEJMoa1212914 — the honest nuance: lifestyle-driven weight loss improved many risk factors but did not reduce heart attacks and strokes over ~10 years.
- Hall KD, Sacks G, Chandramohan D, et al. Quantification of the effect of energy imbalance on bodyweight. The Lancet. 2011;378(9793):826-837. doi:10.1016/S0140-6736(11)60812-X — the math of why weight loss slows and plateaus: a smaller body burns fewer calories.
- Fothergill E, Guo J, Howard L, et al. Persistent metabolic adaptation 6 years after "The Biggest Loser" competition. Obesity. 2016;24(8):1612-1619. doi:10.1002/oby.21538 — a vivid illustration of metabolic adaptation, in which resting metabolism stayed suppressed years after extreme weight loss.
- Zheng Y, Klem ML, Sereika SM, Danford CA, Ewing LJ, Burke LE. Self-weighing in weight management: a systematic literature review. Obesity. 2015;23(2):256-265. doi:10.1002/oby.20946 — regular self-weighing can support weight management when used to track the trend rather than reacting to daily noise.
- Nedeltcheva AV, Kilkus JM, Imperial J, Schoeller DA, Penev PD. Insufficient sleep undermines dietary efforts to reduce adiposity. Annals of Internal Medicine. 2010;153(7):435-441. doi:10.7326/0003-4819-153-7-201010050-00006 — on the same diet, short sleep shifted loss toward lean tissue instead of fat and increased hunger.
- Jensen MD, Ryan DH, Apovian CM, et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults. Circulation. 2014;129(25 Suppl 2):S102-S138. doi:10.1161/01.cir.0000437739.71477.ee — the major clinical guideline: modest sustained loss, comprehensive lifestyle programs, and a stepped approach to medications and surgery.
- Wadden TA, Webb VL, Moran CH, Bailer BA. Lifestyle modification for obesity: new developments in diet, physical activity, and behavior therapy. Circulation. 2012;125(9):1157-1170. doi:10.1161/CIRCULATIONAHA.111.039453 — review of structured behavioral treatment, the most effective non-surgical foundation for lasting weight management.
Connections
- Why Diets Fail
- Sleep, Stress, and Weight
- Mindful & Intuitive Eating
- Emotional Eating
- Weight Loss
- The Potato Diet for Weight Loss
- Exercise
- Fasting
- Meditation
- Endocrinology