N-Acetylcysteine (NAC) Research
N-Acetylcysteine (NAC) is the acetylated form of the amino acid L-cysteine and one of the most rigorously studied small molecules in all of medicine. It has been used clinically since the early 1960s — first as an inhaled mucolytic (Mucomyst, 1963) and then as the FDA-approved antidote for acetaminophen (paracetamol) overdose, where it has essentially eliminated mortality when given within the first 8–10 hours. Beyond these two classic indications, the past three decades have produced a remarkable volume of research into NAC's role in kidney health, liver health, respiratory disease, psychiatric disorders, fertility, and cardiovascular medicine.
The core reason for this breadth is deceptively simple: NAC is a prodrug for glutathione, the body's master intracellular antioxidant. Cysteine is the rate-limiting substrate for glutathione synthesis, and almost every chronic disease of aging involves some form of glutathione depletion. NAC bypasses the bottleneck, protects the cysteine thiol from oxidation, and lets cells rebuild their antioxidant defenses. Layered on top of this, NAC directly scavenges reactive oxygen species, cleaves disulfide bonds in mucus, modulates the cystine-glutamate antiporter in the brain, and donates sulfhydryl groups to recycle nitric oxide from organic nitrates.
Research Topics
NAC & Kidney Health
The most important NAC remedy article, covering the full arc of kidney-protective research: contrast-induced nephropathy prevention (the story from Tepel 2000 through the landmark PRESERVE and ACT trials), chronic kidney disease and hemodialysis oxidative stress, cystinuria stone prevention, diabetic nephropathy, sepsis and cardiac-surgery acute kidney injury, and the rhabdomyolysis use case. Includes Tepel's 2003 hemodialysis cardiovascular trial that remains one of the most influential secondary-prevention studies in nephrology.
- Mechanism: glutathione replenishment, medullary vasodilation, NF-kB suppression
- The full contrast-nephropathy story: Tepel, REMEDIAL, ACT, PRESERVE
- Cystine stone prevention via thiol-disulfide exchange
- Dosing protocols — oral vs IV — for every indication
NAC & Glutathione (the Master Antioxidant)
Why cysteine is the rate-limiting step, how NAC delivers it safely, and the evidence that oral NAC actually raises whole-blood and tissue glutathione. Covers the Sekhar GlyNAC work on restoring old-age glutathione deficits, Herzenberg's HIV studies, liposomal glutathione comparisons, and the role of selenium and glycine as cofactors. Explains why "low bioavailability" of intact NAC does not mean low efficacy.
- Glutathione biochemistry: gamma-glutamyl-cysteine-glycine, GSH/GSSG redox cycle
- Why acetylation protects cysteine — and what happens after absorption
- Sekhar's GlyNAC protocol: restoring elderly glutathione to young-adult levels
- Alternatives: liposomal GSH, whey protein, glycine, selenium, sulforaphane
NAC & Liver Health
The FDA-approved use of NAC for acetaminophen overdose is just the beginning. Covers the Lee 2009 Gastroenterology trial showing NAC improves transplant-free survival in non-acetaminophen acute liver failure, the Nguyen-Khac 2011 NEJM trial showing one-month mortality in severe alcoholic hepatitis dropped from 24% to 8% with adjunctive NAC, and evidence in NAFLD/NASH, drug-induced liver injury, and hepatic ischemia-reperfusion during transplantation.
- NAPQI mechanism and why glutathione depletion kills the liver
- The 21-hour IV Prescott protocol and the 72-hour oral Smilkstein protocol
- Rumack-Matthew nomogram interpretation
- Alcoholic hepatitis: the Nguyen-Khac combination with prednisolone
NAC & Respiratory Health
From mucus-thinning scissors to COPD exacerbation reduction. Covers the PANTHEON trial establishing 600 mg twice daily as the evidence-based COPD dose (22% reduction in exacerbations), the Cochrane meta-analysis of mucolytics, the BENE trial in bronchiectasis, the nuanced IPF story (IFIGENIA vs PANTHER-IPF), and De Flora's classic 1997 trial showing NAC attenuates influenza symptoms without preventing infection.
- Three mechanisms: disulfide cleavage, glutathione restoration, ROS scavenging
- Evidence-based COPD dose: 600 mg twice daily
- Cystic fibrosis, chronic bronchitis, and bronchiectasis
- Why inhaled NAC can cause bronchospasm in asthmatics
NAC & Mental Health
The psychiatric literature on NAC is one of the most surprising in medicine. Covers Berk's schizophrenia and bipolar depression trials, the Grant 2009 trichotillomania trial that launched the field, OCD augmentation studies, Gray's landmark adolescent cannabis cessation trial, cocaine and nicotine addiction work, Hardan's Stanford autism irritability trial, and Back's PTSD-substance-use study. Explains the glutamate-homeostasis hypothesis via the cystine-glutamate antiporter.
- Glutamate modulation through system xc- and mGluR2/3 signaling
- Strongest evidence: trichotillomania, excoriation disorder, schizophrenia adjunct
- Addiction: cocaine, cannabis (adolescent), nicotine, gambling
- Autism spectrum disorder: Hardan's ABC-Irritability data
NAC, Fertility & PCOS
A strong body of RCT evidence in reproductive medicine. Covers Safarinejad's male-factor trials (sperm count, motility, morphology, DNA fragmentation), the Rizk-Badawy-Salehpour triad on NAC + clomiphene for clomiphene-resistant PCOS (ovulation odds ratio 8.4), NAC vs metformin comparative data, the Amin 2008 recurrent pregnancy loss trial (live birth rate nearly tripled), and Porpora's endometriosis observational work showing measurable shrinkage of ovarian endometriomas.
- Oxidative stress in sperm, oocyte, and endometrium
- PCOS: NAC + clomiphene in clomiphene-resistant anovulation
- Recurrent pregnancy loss — Amin 2008 with folic acid
- Endometriosis: Porpora's 3-days-a-week protocol
NAC & Cardiovascular Health
The classic cardiovascular use of NAC is preventing nitrate tolerance (Packer 1987, Horowitz 1988). Beyond that, the NACIAM trial in STEMI patients showed a 5.5 percentage-point absolute reduction in MRI-measured infarct size when NAC was added to primary PCI. Homocysteine lowering, endothelial function restoration, and the nuanced lipid effects (HDL up, LDL unchanged) are covered. The nitroglycerin interaction — enhanced vasodilation, potential hypotension — is a genuine clinical concern patients must understand.
- Nitrate tolerance reversal: the original cardiovascular indication
- NACIAM: 5.5% absolute infarct-size reduction in acute MI
- Homocysteine lowering via disulfide displacement
- Critical interaction with nitroglycerin — severe hypotension risk
Common Themes Across All Indications
- Glutathione replenishment — NAC → deacetylation → cysteine → the rate-limiting step of glutathione synthesis. Tissues recover their antioxidant capacity within days.
- Direct thiol antioxidant action — the free -SH group scavenges hydroxyl radicals, hypochlorous acid, and reactive nitrogen species independently of glutathione.
- Disulfide exchange — NAC cleaves S–S bonds in mucus glycoproteins (mucolytic effect), in plasma protein-homocysteine disulfides (homocysteine lowering), and in cystine crystals (kidney stone prevention).
- Nitric oxide donation — S-nitrosothiol formation with NO creates a stable NO reservoir that restores endothelial function and reverses nitrate tolerance.
- Glutamate homeostasis — in the brain, cystine exchanges for glutamate via system xc-, which normalizes extrasynaptic glutamate tone and underpins the psychiatric benefits.
- NF-kB suppression — cellular redox state is tightly coupled to inflammatory transcription, so glutathione restoration automatically lowers cytokine output.
Dosing at a Glance
- General antioxidant / glutathione support: 600–1,200 mg/day orally, usually divided twice daily
- COPD (PANTHEON-validated): 600 mg twice daily (1,200 mg/day)
- Psychiatric adjunct: 2,000–2,400 mg/day divided, for at least 8–12 weeks
- PCOS ovulation induction: 1,200 mg/day on cycle days 3–7 alongside clomiphene
- Male fertility: 600 mg once daily for 3–6 months
- Cystinuria stones: 1–3 g/day divided
- Acetaminophen overdose (IV, hospital only): 150 mg/kg over 1 h → 50 mg/kg over 4 h → 100 mg/kg over 16 h
Oral bioavailability of the intact NAC molecule is only 4–10% because of extensive first-pass deacetylation — but the deacetylation products (free cysteine and glutathione) are themselves the active species, so "low bioavailability" is misleading. Taking NAC with or without food is acceptable; effervescent and oral-solution forms are better tolerated than capsules because the sulfurous odor can drive nausea.
Safety Profile
- Common: nausea, dyspepsia, diarrhea, characteristic rotten-egg sulfur taste — typically mild and dose-related.
- Intravenous: anaphylactoid (histamine-mediated, non-IgE) reactions in ~10–20% during the first loading infusion — typically rash, flushing, bronchospasm; managed by slowing or pausing the drip.
- Asthma: inhaled or nebulized NAC can provoke bronchospasm — pre-treat with a short-acting bronchodilator.
- Critical drug interaction: NAC potentiates nitroglycerin-induced vasodilation. Patients on chronic nitrates must know this before adding NAC.
- Pregnancy: Category B. NAC has been used at very high IV doses in pregnant women for acetaminophen overdose without teratogenic signal.
The FDA has, from 2020 onward, taken an ambiguous position on NAC's status as a dietary supplement (because of its approved drug pedigree) but has exercised enforcement discretion. In Europe it has been sold over-the-counter as a mucolytic for decades.
Related Pages on This Site
- Cysteine — the parent amino acid
- Glycine — the co-limiting amino acid for glutathione synthesis
- Selenium — essential cofactor for glutathione peroxidase
- Liver Cleansing
- Detox Protocols
- Longevity Protocols
Research Papers
Selected PubMed topic searches across the major clinical applications of N-acetylcysteine.
- PubMed: NAC and glutathione synthesis
- PubMed: NAC and acetaminophen hepatotoxicity
- PubMed: NAC and COPD/chronic bronchitis
- PubMed: NAC in PCOS and ovulation
- PubMed: NAC in OCD and trichotillomania
- PubMed: NAC and contrast-induced nephropathy
- PubMed: NAC and nitrate tolerance
- PubMed: NAC in bipolar depression
- PubMed: NAC in pulmonary fibrosis
- PubMed: NAC and homocysteine
- PubMed: NAC and sperm quality/fertility
- PubMed: NAC in autism-associated irritability
Connections
- NAC and Glutathione
- NAC and Liver Health
- NAC and Kidney Health
- NAC and Respiratory Health
- NAC and Mental Health
- NAC and Cardiovascular Health
- NAC, Fertility and PCOS
- Cysteine
- Glycine
- Liver Cleansing
- Bryan Ardis — Detox & Recovery — NAC as the glutathione foundation in the post-spike recovery stack
- Bryan Ardis — Vaccine-Injury Recovery
Featured Videos
NAC--(N-Acetylcysteine) Potent Antioxidant and Anti-Inflammatory

The REAL Reasons To Use N-Acetylcysteine (NAC)
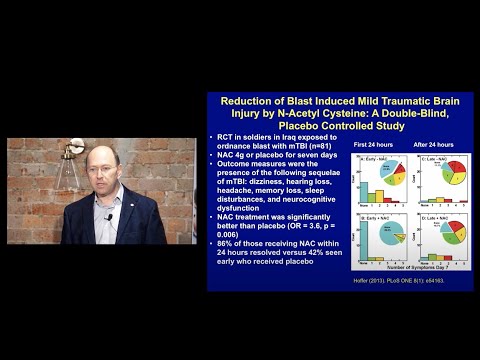
Applications of N-Acetylcysteine (NAC) - From Addiction to Autism By Prof Berk

What You ACTUALLY Need to Know About N-Acetylcysteine (NAC)
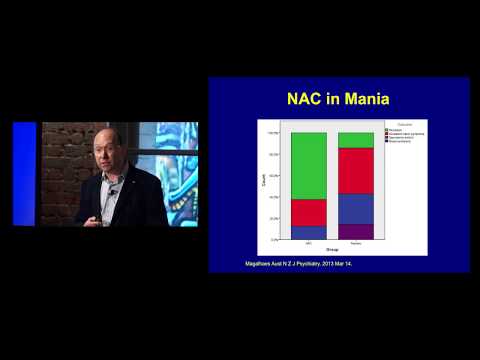
N-Acetylcysteine (NAC) in Schizophrenia and Bipolar Disorder- Prof Michael Berk
How much N-Acetylcysteine (NAC) should I take for illness prevention?

Georgina Oliver - An Update on Inflammation and N-acetylcysteine (NAC) in OCD.

NAC Attack—A Multicenter Placebo-Controlled Clinical Trial to Test Oral N-Acetylcysteine in Patient
10 AMAZING Benefits of NAC (N-Acetylcysteine) Supplements