NAC & Glutathione: The Master Antioxidant Connection
Glutathione (GSH) is the master intracellular antioxidant in every nucleated cell in the human body. It is not a vitamin, not a mineral, and not something you get directly from food in any meaningful amount — it is a tripeptide the body manufactures from three amino acids. When glutathione is plentiful, cells resist oxidative damage, detoxify electrophilic toxins, and run their mitochondria cleanly. When it runs low, the consequences cascade through aging, chronic disease, infection susceptibility, and neurodegeneration.
The single biggest lever for raising glutathione is cysteine supply, and the cleanest way to supply cysteine is N-acetylcysteine (NAC). This article explains the biochemistry, the clinical evidence that NAC actually raises glutathione in humans, how to dose it, and what cofactors (glycine, selenium) matter most.
Table of Contents
- What Is Glutathione?
- Biochemistry: Three Amino Acids, Two Steps
- Why Cysteine Is Rate-Limiting
- Why NAC Works — The Acetyl Protection Trick
- What Glutathione Does
- Conditions of Glutathione Depletion
- Evidence That Oral NAC Raises Glutathione
- GlyNAC: The Glycine + NAC Protocol
- Oral vs IV Bioavailability
- Alternatives and Cofactors
- Dosing for Glutathione Support
- Safety
- References
- Connections
- Featured Videos
What Is Glutathione?
Glutathione is a tripeptide — a small protein made of three amino acids: glutamate, cysteine, and glycine. Its full chemical name is gamma-L-glutamyl-L-cysteinyl-glycine. The name matters because glutathione's peptide bond between glutamate and cysteine is unusual — it uses glutamate's gamma-carboxyl group rather than the standard alpha-carboxyl. This gamma-bond makes glutathione resistant to most cellular peptidases, which is how the body keeps its intracellular glutathione pool stable and metabolically durable at concentrations of 1–10 millimolar — among the highest small-molecule concentrations of any cellular metabolite.
All the antioxidant chemistry happens at one specific atom: the sulfur of cysteine's thiol group (–SH). When glutathione donates an electron to neutralize a reactive oxygen species, two glutathione molecules pair up and form an oxidized dimer called GSSG (glutathione disulfide). Healthy cells maintain a GSH:GSSG ratio above 100:1. When that ratio drops below ~10:1, the cell is in severe oxidative stress.
Biochemistry: Three Amino Acids, Two Steps
Glutathione is synthesized in the cytosol of essentially every cell — the liver is the dominant systemic producer. Synthesis happens in two ATP-dependent steps:
- Step 1 (rate-limiting): Glutamate-cysteine ligase (GCL). Glutamate + cysteine + ATP → gamma-glutamylcysteine + ADP + Pi. GCL is feedback-inhibited by glutathione itself (Ki ~2.3 mM), which keeps production in check. Under oxidative stress the Nrf2/Keap1 transcription factor system induces GCL expression through antioxidant response elements (AREs) in its promoter, ramping up synthetic capacity.
- Step 2: Glutathione synthetase (GS). Gamma-glutamylcysteine + glycine + ATP → glutathione + ADP + Pi. Not rate-limiting under normal conditions, but glycine can become co-limiting in aging and protein restriction.
The gamma-glutamyl cycle (discovered by Alton Meister) describes how glutathione is continuously degraded and resynthesized. Gamma-glutamyl transpeptidase (GGT) on the outer cell membrane cleaves extracellular glutathione; the liberated cysteinylglycine is hydrolyzed to cysteine and glycine; those amino acids are re-imported for resynthesis. This is how the liver exports glutathione into bile and plasma, and how peripheral tissues (the kidney especially) recover glutathione's building blocks.
Why Cysteine Is Rate-Limiting
Of the three amino acid substrates, glutamate is abundant and not limiting, glycine is sometimes co-limiting, and cysteine is almost always rate-limiting. Three reasons:
- Free cysteine is toxic at high levels. Cysteine can act as an excitotoxin on NMDA receptors and autoxidize to cystine in the plasma, generating hydrogen peroxide. The body therefore keeps intracellular free cysteine extremely low — roughly 10–100 micromolar in hepatocytes. Cells must actively import cysteine or its oxidized dimer cystine through dedicated transporters (ASC for cysteine, xCT / system xc- for cystine).
- The thiol is vulnerable to oxidation. Free cysteine in aqueous solution at neutral pH autoxidizes to cystine in minutes to hours. Delivering reduced cysteine to cells is mechanically harder than delivering any other amino acid.
- Dietary cysteine is limited. Methionine can be converted to cysteine via the trans-sulfuration pathway, but the enzymatic flux is modest and requires pyridoxal phosphate (vitamin B6) as a cofactor.
The practical implication: whether glutathione goes up or down in a given tissue is almost always about whether cysteine supply is keeping up with demand.
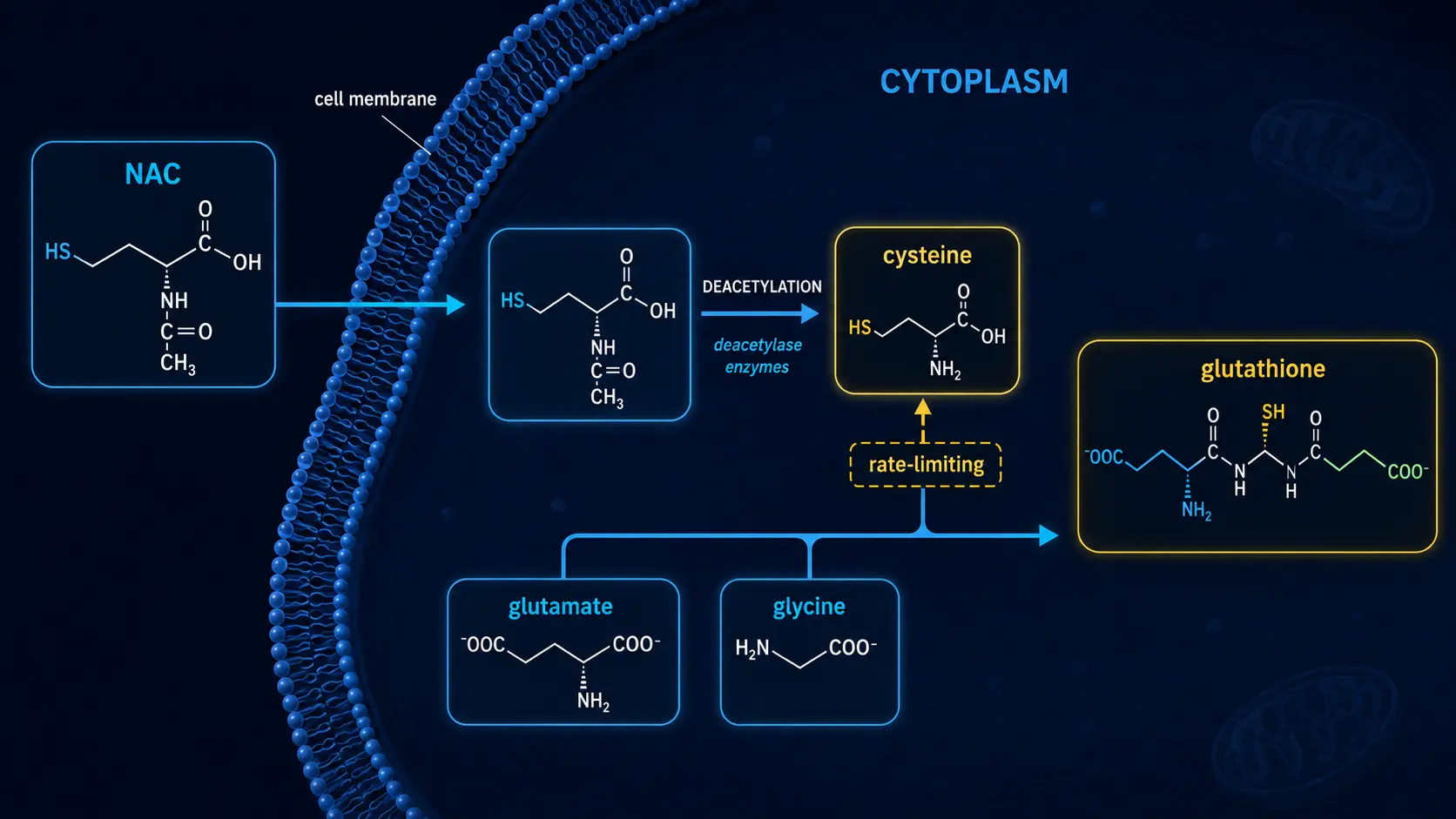
Why NAC Works — The Acetyl Protection Trick
N-acetylcysteine is just cysteine with an acetyl group (–COCH3) attached to the alpha-amino nitrogen. That single modification changes everything about its pharmacology:
- Thiol protection. The acetyl group sterically and electronically stabilizes the thiol, so NAC survives as a stable pill, capsule, or effervescent tablet at room temperature. Pure cysteine in solution oxidizes too quickly for reliable manufacturing.
- Reduced toxicity. NAC does not carry cysteine's excitotoxic liability because the acetylated amine can't interact with NMDA receptors the same way.
- Better oral tolerability. Free cysteine at supplemental doses causes GI distress and has a stronger sulfur odor. NAC is by no means odorless (it still smells like rotten eggs) but it is tolerated well enough for multi-gram daily dosing.
- Deacetylation in vivo. Once absorbed, NAC is rapidly deacetylated by cellular acylase I — most heavily in liver, kidney, and small intestine — to release free cysteine exactly where it is needed. The acetyl group has done its job of getting cysteine through manufacturing, storage, packaging, swallowing, digestion, and absorption.
Beyond its prodrug role, NAC has two direct activities of its own: it is a mucolytic (cleaving disulfide bonds in mucus glycoproteins — the basis of its original 1963 respiratory use) and a direct antioxidant (its free thiol scavenges hydroxyl radicals and hypochlorous acid without needing to be converted to glutathione first).
What Glutathione Does
Master Antioxidant
Glutathione is the substrate for glutathione peroxidase (GPx), a selenium-dependent enzyme family that reduces hydrogen peroxide to water and lipid hydroperoxides to lipid alcohols. This is the body's primary defense against peroxide-mediated oxidative injury. Oxidized glutathione (GSSG) is recycled back to GSH by glutathione reductase, which uses NADPH from the pentose phosphate pathway.
Phase II Detoxification (Liver)
Glutathione S-transferases (GSTs) conjugate glutathione to electrophilic xenobiotics — including the reactive acetaminophen metabolite NAPQI, aflatoxin epoxides, many chemotherapy drugs, and environmental pollutants. The resulting glutathione-conjugate is exported, converted to a mercapturic acid, and excreted in urine. This is why NAC is the FDA-approved acetaminophen antidote: it replenishes the glutathione needed to neutralize NAPQI before it can bind hepatocyte proteins.
Immune Cell Function
T lymphocytes, natural killer cells, and macrophages require high intracellular glutathione for proliferation, cytokine production, and cytotoxic function. Low glutathione biases the Th1/Th2 balance toward Th2 dominance, impairs IL-2 signaling, and reduces antigen-presenting capability.
Mitochondrial Protection
Mitochondria have a separate glutathione pool imported across the inner membrane via dicarboxylate and 2-oxoglutarate carriers. This pool detoxifies the superoxide continuously generated at Complex I and Complex III of the electron transport chain. Mitochondrial glutathione depletion is a central event in acetaminophen hepatotoxicity, ischemia-reperfusion injury, and neurodegenerative disease.
Regenerating Other Antioxidants
Glutathione recycles oxidized vitamin C (dehydroascorbate) back to reduced ascorbate, and indirectly regenerates vitamin E. This puts GSH at the top of the cellular antioxidant hierarchy.
Conditions of Glutathione Depletion
- Aging. Erythrocyte and tissue glutathione fall roughly 30–50% between ages 20 and 80. Reduced GCL expression and reduced cysteine + glycine flux are the mechanisms.
- HIV infection. Plasma and lymphocyte glutathione are markedly low; Herzenberg and colleagues showed that low glutathione predicts HIV mortality independent of CD4 count.
- Chronic alcoholism. Ethanol depletes hepatic mitochondrial glutathione by 40–60% through CYP2E1-generated ROS and reduced cysteine availability from malnutrition.
- Acetaminophen overdose. CYP2E1 oxidizes 5–10% of a dose to NAPQI, which depletes glutathione rapidly; centrilobular necrosis follows.
- COPD, cystic fibrosis, chronic lung inflammation. Cigarette smoke and chronic neutrophilic inflammation consume airway glutathione.
- Type 2 diabetes, metabolic syndrome, cardiovascular disease. Hyperglycemia-driven mitochondrial superoxide depletes glutathione systemically.
- Chronic kidney disease and hemodialysis. Dialysis membranes, chronic iron therapy, and uremia all consume glutathione.
- Parkinson's disease and Alzheimer's disease. Substantia nigra and hippocampal glutathione are reduced early in both diseases.
- Critical illness, sepsis, major surgery, burns, chemotherapy. Acute consumption outpaces synthesis.
- Genetic. GCLC promoter polymorphisms, glutathione synthetase deficiency (rare).
- Nutritional. Chronic protein malnutrition, low-selenium diets (impaired GPx), low-B6 (blocked transsulfuration).
Evidence That Oral NAC Raises Glutathione
This is the key empirical question — does oral NAC actually raise glutathione in humans, or just raise plasma NAC?
Healthy Adults
- Kleinveld 1992 (Eur J Clin Pharmacol): 600 mg oral NAC raised plasma free cysteine within 1–2 hours and modestly raised plasma glutathione.
- Bridgeman 1991 (Thorax): 600 mg NAC three times daily for 5 days in healthy subjects significantly raised bronchoalveolar lavage glutathione — proving oral NAC reaches the lung in active form.
Aging — The Sekhar Studies
Rajagopal Sekhar at Baylor College of Medicine has led a landmark research program on age-related glutathione deficiency. In American Journal of Clinical Nutrition 2011, he showed elderly subjects (mean age 73) had erythrocyte glutathione ~53% lower than young controls. Supplementing cysteine (as NAC) plus glycine for just 14 days restored glutathione to young-adult levels (+94.6%) and cut F2-isoprostanes (a marker of lipid peroxidation) by 50%.
The 2021 follow-up in Clinical and Translational Medicine used 8 g/day glycine plus 8 g/day NAC (the GlyNAC protocol) for 16 weeks in older adults. It restored glutathione, reduced oxidative stress, improved mitochondrial function, and produced measurable gains in cognition, gait speed, and muscle strength.
HIV — The Herzenberg Studies
Leonard and Leonore Herzenberg at Stanford showed in PNAS 1997 that HIV patients had severely depleted T-cell glutathione and that NAC 3,200–8,000 mg/day for 8 weeks restored T-cell glutathione toward normal. A retrospective survival analysis found 2-year mortality of 40% in low-glutathione patients versus 8% in replenished patients — a striking result that helped establish NAC as a credible HIV adjunct.
COPD
The PANTHEON trial (Zheng 2014, Lancet Respir Med) showed NAC 600 mg twice daily reduced COPD exacerbations by 22% over 1 year — most likely through raised airway glutathione and reduced oxidative stress. This is a large, rigorous outcome-level confirmation of biological activity.
Psychiatric
Berk's schizophrenia trial (2008, Biol Psychiatry) used NAC 2 g/day for 24 weeks and showed PANSS-measurable symptom improvement, with mechanistic underpinning in reduced cortical glutathione (measured by magnetic resonance spectroscopy in schizophrenia) being restored.
Summary
Across oral doses of 600–2,400 mg/day, most studies report a 30–90% rise in whole-blood or erythrocyte glutathione within 2–8 weeks. Plasma free cysteine roughly doubles within 1–2 hours after each dose. The "low bioavailability" of intact NAC (4–10%) is misleading because the liver and gut aggressively deacetylate NAC to cysteine, which is used directly for glutathione synthesis where it is needed — not as a free NAC molecule circulating in plasma.
GlyNAC: The Glycine + NAC Protocol
The most interesting recent development in glutathione nutrition is the recognition that glycine is co-limiting with cysteine in aging and chronic disease — not just cysteine. Sekhar's GlyNAC protocol adds glycine 3–8 g/day to NAC 600–8,000 mg/day, producing synergistic glutathione restoration beyond what NAC alone can achieve. In a 16-week open-label pilot in older adults, GlyNAC improved:
- Erythrocyte glutathione (restored to young-adult levels)
- Mitochondrial fatty-acid oxidation (measured by respirometry)
- Endothelial function (flow-mediated dilation)
- Insulin resistance (HOMA-IR)
- Muscle strength (grip, 6-minute walk)
- Cognitive processing speed
- Inflammatory markers (IL-6, TNF-alpha)
Randomized follow-up trials are ongoing. For now, a reasonable supplemental translation is NAC 600–1,200 mg twice daily plus glycine 3 g at bedtime, both of which are cheap, well-tolerated, and supported by mechanistic data. Glycine at 3 g before bed has the bonus of promoting sleep onset.
Oral vs IV Bioavailability
Oral NAC. Intact-molecule bioavailability is 4–10% due to extensive first-pass metabolism (Borgstrom 1986, Eur J Clin Pharmacol). Tmax is 1–2 hours. Plasma half-life of total NAC is 2–6 hours, shorter for the reduced form. But because gut and liver deacetylate NAC directly into the cysteine and glutathione pools, the "low bioavailability" figure understates therapeutic effect.
IV NAC. 100% bioavailability, reserved for hospital settings like acetaminophen overdose (300 mg/kg total over 21 hours in the Prescott regimen). Plasma concentrations are 10-fold higher than with oral dosing.
CNS penetration. Cysteine crosses the blood-brain barrier slowly via the ASC transporter. Brain glutathione does rise measurably on magnetic resonance spectroscopy after oral NAC in Parkinson's and Gaucher disease patients (Holmay 2013, Clin Neuropharmacol). This supports NAC's psychiatric-neurological applications.
Alternatives and Cofactors
- Liposomal glutathione. Sinha 2018 (Eur J Clin Nutr): 500 mg/day liposomal glutathione raised blood glutathione ~40% at 1 month and doubled NK-cell activity. More efficient per milligram than oral non-liposomal glutathione.
- Direct oral glutathione (non-liposomal). Richie 2015 (Eur J Nutr): 250 or 1,000 mg/day for 6 months raised blood and lymphocyte glutathione — disproving the older dogma that oral GSH is entirely hydrolyzed in the gut.
- Whey protein. Rich in cysteine and glutamylcysteine, especially in undenatured preparations. Micke 2001 (Eur J Nutr): 40 g/day whey protein isolate raised lymphocyte glutathione in HIV and hepatitis patients.
- Glycine. Essential for Step 2 of glutathione synthesis; co-limiting with cysteine in aging. 3–8 g/day.
- Selenium. Required cofactor for glutathione peroxidase. RDA 55 micrograms, upper limit 400 micrograms. Brazil nuts, seafood, and organ meats are dietary sources.
- Alpha-lipoic acid. 300–600 mg/day. Regenerates glutathione indirectly and recycles other antioxidants.
- Sulforaphane (broccoli sprouts). A potent Nrf2 activator; induces the GCL gene rather than supplying substrate — a complementary mechanism to NAC.
- Silymarin (milk thistle). Raises hepatic glutathione by roughly 35% in animal and some human studies.
- Curcumin, resveratrol, EGCG (green tea). Mild Nrf2 activators.
- Dietary cysteine/methionine. Eggs, poultry, fish, legumes, garlic, onions, cruciferous vegetables.
Dosing for Glutathione Support
- General antioxidant / preventive: 600–1,200 mg/day in divided doses. Most effective as 600 mg BID.
- Active immune/respiratory support (COPD dose): 600 mg twice daily (PANTHEON-validated).
- Psychiatric adjunct: 2,000–2,400 mg/day divided, 8–12 weeks minimum for effect.
- GlyNAC protocol (Sekhar): NAC 100 mg/kg/day plus glycine ~50 mg/kg/day, typically 8 g each in a 70–80 kg adult.
- Timing: With or without food. Empty stomach absorbs slightly faster; with food reduces nausea.
- Form: Effervescent tablets and oral solutions are better tolerated than capsules because the sulfurous odor drives nausea.
Safety
- Most common: nausea, dyspepsia, diarrhea, sulfurous odor/taste. Usually mild and dose-related.
- Inhaled NAC: can trigger bronchospasm in asthmatics; pre-treat with a bronchodilator.
- IV NAC: anaphylactoid (histamine-mediated) reactions in 10–20% during first loading infusion.
- Drug interaction — nitroglycerin: enhanced vasodilation and potential severe hypotension. Always disclose nitrate use to your physician before starting NAC.
- Theoretical: chelates copper and zinc in very large doses; avoid combining with nitroglycerin.
- No tolerance, dependence, or withdrawal. NAC does not require dose escalation over time.
The FDA has taken an ambiguous position on NAC's status as a dietary supplement since 2020 because of its approved drug history, but has exercised enforcement discretion. It has been sold over-the-counter in Europe for decades as a mucolytic.
References
- Sekhar RV, Patel SG, Guthikonda AP, et al. Deficient synthesis of glutathione underlies oxidative stress in aging and can be corrected by dietary cysteine and glycine supplementation. Am J Clin Nutr 2011;94(3):847–853. PMID 21795440.
- Kumar P, Liu C, Hsu JW, et al. Glycine and N-acetylcysteine (GlyNAC) supplementation in older adults improves glutathione deficiency, oxidative stress, mitochondrial dysfunction, inflammation, insulin resistance, endothelial dysfunction, genotoxicity, muscle strength, and cognition. Clin Transl Med 2021;11(3):e372. PMID 33783984.
- Herzenberg LA, De Rosa SC, Dubs JG, et al. Glutathione deficiency is associated with impaired survival in HIV disease. PNAS 1997;94(5):1967–1972. PMID 9050888.
- De Rosa SC, Zaretsky MD, Dubs JG, et al. N-acetylcysteine replenishes glutathione in HIV infection. Eur J Clin Invest 2000;30(10):915–929. PMID 11029607.
- Bridgeman MM, Marsden M, MacNee W, Flenley DC, Ryle AP. Cysteine and glutathione concentrations in plasma and bronchoalveolar lavage fluid after treatment with NAC. Thorax 1991;46(1):39–42. PMID 1871695.
- Kleinveld HA, Demacker PN, Stalenhoef AF. Failure of NAC to reduce LDL oxidizability in healthy subjects. Eur J Clin Pharmacol 1992;43(6):639–642. PMID 1493845.
- Borgstrom L, Kagedal B, Paulsen O. Pharmacokinetics of NAC in man. Eur J Clin Pharmacol 1986;31(2):217–222. PMID 3803419.
- Olsson B, Johansson M, Gabrielsson J, Bolme P. Pharmacokinetics and bioavailability of reduced and oxidized NAC. Eur J Clin Pharmacol 1988;34(1):77–82. PMID 3360052.
- Lu SC. Glutathione synthesis. Biochim Biophys Acta 2013;1830(5):3143–3153. PMID 22995213.
- Lu SC. Regulation of glutathione synthesis. Mol Aspects Med 2009;30(1–2):42–59. PMID 18601945.
- Droge W, Breitkreutz R. Glutathione and immune function. Proc Nutr Soc 2000;59(4):595–600. PMID 11115795.
- Mari M, Morales A, Colell A, Garcia-Ruiz C, Fernandez-Checa JC. Mitochondrial glutathione, a key survival antioxidant. Antioxid Redox Signal 2009;11(11):2685–2700. PMID 19558212.
- Holmay MJ, Terpstra M, Coles LD, et al. NAC boosts brain and blood glutathione in Gaucher and Parkinson diseases. Clin Neuropharmacol 2013;36(4):103–106. PMID 23860343.
- Sinha R, Sinha I, Calcagnotto A, et al. Oral supplementation with liposomal glutathione elevates body stores of glutathione and markers of immune function. Eur J Clin Nutr 2018;72(1):105–111. PMID 28853742.
- Richie JP Jr, Nichenametla S, Neidig W, et al. RCT of oral glutathione supplementation on body stores of glutathione. Eur J Nutr 2015;54(2):251–263. PMID 24791752.
- Micke P, Beeh KM, Buhl R. Effects of long-term supplementation with whey proteins on plasma glutathione levels of HIV-infected patients. Eur J Nutr 2002;41(1):12–18. PMID 11990003.
- Atkuri KR, Mantovani JJ, Herzenberg LA. NAC — a safe antidote for cysteine/glutathione deficiency. Curr Opin Pharmacol 2007;7(4):355–359. PMID 17602868.
- Prescott LF, Park J, Ballantyne A, Adriaenssens P, Proudfoot AT. Treatment of paracetamol overdose with NAC. Lancet 1977;2(8035):432–434. PMID 71287.
- Zheng JP, Wen FQ, Bai CX, et al. Twice daily NAC 600 mg for exacerbations of COPD (PANTHEON). Lancet Respir Med 2014;2(3):187–194. PMID 24621680.
- Tirouvanziam R, Conrad CK, Bottiglieri T, Herzenberg LA, Moss RB, Herzenberg LA. High-dose oral NAC, a glutathione prodrug, modulates inflammation in cystic fibrosis. PNAS 2006;103(12):4628–4633. PMID 16537378.
Research Papers
Selected PubMed topic searches relevant to glutathione biology, NAC-driven glutathione repletion, and downstream antioxidant effects.
- PubMed: NAC and glutathione synthesis
- PubMed: Glutathione peroxidase and oxidative stress
- PubMed: Glutathione S-transferase and detoxification
- PubMed: Glutathione and hepatocyte function
- PubMed: Glutathione decline with aging
- PubMed: Oral glutathione bioavailability
- PubMed: Liposomal glutathione absorption
- PubMed: Glycine and glutathione synthesis
- PubMed: Glutamate-cysteine ligase (GCLC)
- PubMed: Nrf2 and glutathione antioxidant response
- PubMed: Glutathione and neurodegeneration
- PubMed: Glutathione and mitochondrial function
Connections
- NAC Overview
- NAC & Kidney Health
- NAC & Liver Health
- NAC & Respiratory Health
- Cysteine
- Glycine
- Glutamine
- Selenium
- Vitamin C
- Vitamin E
- Longevity Protocols
- Liver Cleansing
Featured Videos

NAC & Glutathione Are Transforming Aging! New Study

The Truth About Glutathione For Skin Whitening

What Happens to Your BODY When You Use GLUTATHIONE?

The BEST Form of Glutathione - IV, IM, SQ, or LIPOSOMAL

Doctor V - Is Glutathione safe? | Skin Of Colour | Brown Or Black Skin

Dr. Anderson REVEALS The 5 MISTAKES You’re Making When Taking GLUTATHIONE
Glutathione Detox: The Science of Glutathione and Alcohol – Thomas DeLauer

The BEST Glutathione: Oral vs IV vs Topical vs Liposomal

Glutathione: Secret Weapon For Immunity, Anti-Aging, Arthritis, Muscle Recovery, and More!
Here’s the Best Form of Glutathione | Stop Wasting Your Money!

🔥Best Glutathione Tablets for Skin Whitening [Most Effective & Affordable Picks] | Clinic Eximus

THE TRUTH ABOUT GLUTATHIONE FOR SKIN WHITENING| DR DRAY
Glutathione - The Tripeptide Antioxidant & Reducing Agent

Glutathione Benefits | Must See!

Liposomal Glutathione Benefits: Gut, Immunity and more!

Glutathione for Skin Whitening: What you NEED to KNOW