Liver Extract
Liver extract is one of the rare old remedies that actually earned a Nobel Prize. A century ago, before anyone knew what vitamin B12 was, doctors discovered that feeding patients enormous amounts of raw liver — and later a concentrated liver extract injected into a vein — could rescue people dying of pernicious anemia, a disease that had been a certain death sentence. It worked, and it worked for a real, knowable reason: liver is extraordinarily rich in the very nutrient those patients couldn't absorb on their own. This page tells that genuine medical-history story honestly, explains what liver extract actually contains, and is clear about why modern medicine has replaced the crude extract with cleaner, safer treatments — and where today's "desiccated liver" supplements fit, including the real safety risks (too much vitamin A and iron) that the marketing tends to leave out. Note that this page is about the therapeutic extract as a remedy; if you're interested in eating liver as a nutrient-dense food, see the dedicated Beef Liver page.
Table of Contents
- Historical Medical Use (the 1926 U.S. Dispensatory)
- The 1934 Nobel Prize Story
- What Liver Extract Actually Is
- Why It Worked & What Replaced It
- Modern Desiccated-Liver Supplements (Honestly)
- How It's Used Today
- Safety, Cautions & Myths
- Diagnose the Anemia First
- Key Research Papers
- Connections
- Featured Videos
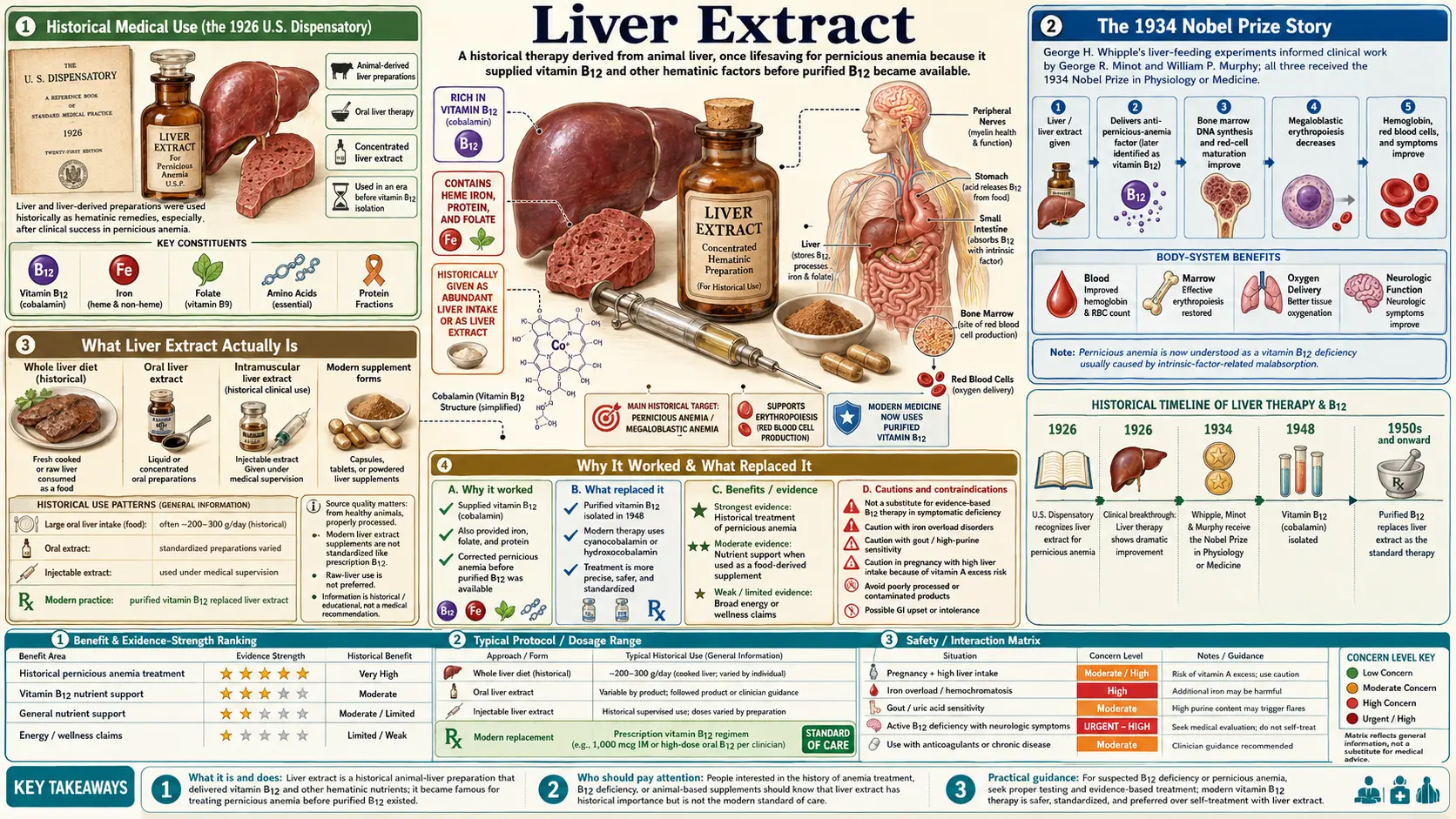
Historical Medical Use (the 1926 U.S. Dispensatory)
In the 1920s, around the time the 21st edition of the United States Dispensatory (Wood & LaWall, 1926) catalogued the era's standard medicines, liver and concentrated liver preparations were entering the pharmacopeia for one overwhelming purpose: the treatment of anemia, and above all the deadly form then called pernicious anemia. The understanding of the day was practical rather than molecular — physicians could see that liver was unusually rich in the "anti-anemic factor," and that giving it to patients rebuilt their blood. They knew liver carried a lot of iron and some unidentified substance that the bone marrow desperately needed to make red blood cells; they did not yet know that substance was vitamin B12, which would not be isolated for more than two decades.
This is the honest historical framing the rest of this page builds on: doctors of 1926 used liver and liver extract for anemia, and they were largely right to. Unlike many remedies of that era, this one was not folklore that later collapsed under scrutiny — it was an early, empirical version of a treatment we still use today, just in a purer form. The belief that "liver is rich in iron and the blood-building factor, with natural cofactors" was, in its plain outline, correct. What changed was not whether it works but how precisely we can now deliver the active ingredient.
The 1934 Nobel Prize Story
To appreciate liver extract, you have to understand how terrifying pernicious anemia was before the 1920s. "Pernicious" literally means deadly, and the name was earned: patients grew progressively weaker, pale, breathless, and confused as their blood failed, and the disease was essentially always fatal. There was no treatment that reliably worked.
Three American researchers changed that. Building on George Whipple's experiments showing that liver in the diet sped the recovery of blood in anemic dogs, two Boston physicians, George Minot and William Murphy, took the radical step of feeding their pernicious-anemia patients massive daily amounts of raw or lightly cooked liver — roughly half a pound a day. The results, reported in 1926, were astonishing: patients who had been dying began to recover, their red blood cell counts climbing back toward normal. A uniformly lethal disease had become treatable with food.
Eating half a pound of raw liver every day for life is, understandably, hard to stomach. The next advance, led by the chemist Edwin Cohn, was to concentrate the active material into a potent liver extract — a fraction many times stronger than the raw organ — that could be given in far smaller amounts, and eventually injected. This made the treatment practical and is the "liver extract" the era's medicine cabinets and the Dispensatory referred to.
In 1934, the Nobel Prize in Physiology or Medicine was awarded jointly to George Whipple, George Minot, and William Murphy "for their discoveries concerning liver therapy in cases of anaemia." It remains one of the clearest examples in medicine of an empirical food remedy being validated, refined, and honored at the highest level — and then, fittingly, superseded once science caught up to why it worked.
What Liver Extract Actually Is
Liver is the body's nutrient warehouse — for animals as much as for us — so an extract or a dried (desiccated) preparation of it is essentially a concentrated multi-nutrient. The components that made it an anti-anemia treatment, and that still matter nutritionally, are:
- Vitamin B12 (cobalamin) — this is the real hero of the story. Liver is one of the richest natural sources of B12 on earth, and B12 is precisely what pernicious-anemia patients are missing. The vitamin is needed for the bone marrow to mature red blood cells and for the protective myelin sheath around nerves. (See the dedicated Vitamin B12 page.)
- Heme iron — liver supplies iron in the heme form, the same form found in blood, which the gut absorbs far more readily than the non-heme iron in plants or in many iron tablets. Iron is the raw material for hemoglobin, the oxygen-carrying pigment in red cells. (See Iron.)
- Folate (vitamin B9) — liver is also rich in folate, the other key vitamin for making red blood cells. Folate and B12 work as partners in the same DNA-building pathway, which is why deficiency of either produces a similar "megaloblastic" anemia with large, immature red cells. (See Vitamin B9 (Folate).)
- Preformed vitamin A (retinol) — liver stores vitamin A in very high concentrations. This is genuinely useful nutritionally, but it is also the source of one of the supplement's biggest safety problems, covered below.
- Other cofactors — copper, riboflavin (B2), and other B vitamins that support red-cell production, plus protein. These are the "natural cofactors" the old descriptions referred to — real, but not magical.
The historical injectable liver extract was a purified fraction concentrated for its anti-anemia potency. Today's over-the-counter "desiccated liver" is different: it is simply whole liver, dried and powdered into capsules or tablets, so it carries the whole nutrient profile — including the parts (vitamin A, iron) you may not want in large, daily amounts.
Why It Worked & What Replaced It
The reason liver therapy worked turned out to be elegantly simple, and it took another generation of science to reveal it. In 1948, researchers in the United States and Britain independently isolated the pure red, cobalt-containing crystalline compound responsible for the anti-anemia effect: vitamin B12. The British chemist Dorothy Hodgkin later solved its complex molecular structure using X-ray crystallography, work that contributed to her own Nobel Prize in Chemistry in 1964. Liver had simply been a very rich, if crude, delivery vehicle for this one vitamin.
This discovery also explained why pernicious anemia happened in the first place. Most people absorb B12 from food using a stomach protein called intrinsic factor. In pernicious anemia, an autoimmune process attacks the stomach lining and shuts down intrinsic factor, so dietary B12 — and the B12 in oral liver extract — can't be absorbed normally through the gut. Minot and Murphy's enormous liver doses worked partly by sheer force of quantity (a small fraction gets absorbed even without intrinsic factor) and by also supplying iron and folate. But it was an indirect, brute-force solution to a problem we can now address directly.
Once pure B12 was available, the logic was obvious: instead of feeding (or injecting) crude liver, just give the patient the actual vitamin. B12 injections bypass the broken gut entirely, and we now also know that high-dose oral B12 can work for many people because a small percentage is absorbed by simple diffusion that doesn't need intrinsic factor. For iron-deficiency anemia, modern iron supplements (and, when needed, intravenous iron) deliver a precise, measured dose. In every respect — purity, accuracy of dosing, convenience, and safety — these modern treatments outperform crude liver extract. That is why injectable liver extract, the toast of 1934, has essentially vanished from medicine: not because it failed, but because we learned exactly what in it was doing the work and isolated it.
Modern Desiccated-Liver Supplements (Honestly)
You can still buy liver as a supplement today — usually desiccated (dried) beef liver in capsules or tablets, often marketed to athletes, people on low-energy diets, or those seeking a "whole-food" source of iron and B vitamins. Here's an honest appraisal.
What's genuinely true: desiccated liver is a legitimate, nutrient-dense whole food in concentrated form. It really does provide bioavailable B12, heme iron, folate, vitamin A, and copper. For someone who can't or won't eat liver as food but wants those nutrients from an animal source, it's a real option, and the heme iron in particular is absorbed better than the iron in many plant-based or non-heme tablets.
What's overstated: the marketing often wraps desiccated liver in vague "energy," "detox," "vitality," or "ancestral superfood" language, and sometimes implies it treats fatigue or anemia on its own. It is a food supplement, not a therapy for a diagnosed deficiency. If you actually have B12-deficiency or iron-deficiency anemia, the correct treatment is a measured, monitored dose of B12 or iron prescribed after testing — not a guess-dose of liver capsules. The "natural cofactors make it work better than a vitamin" claim is mostly marketing: the science behind B12 and iron treatment is built on the isolated nutrients, which is exactly what cured the disease once we had them.
The catch that marketing skips: because desiccated liver carries the whole liver, it also concentrates two things that can build up to harmful levels — preformed vitamin A and iron. Unlike most water-soluble vitamins, both of these are stored in the body and can accumulate. That turns the supplement's main selling point (it's loaded with nutrients) into its main risk if taken in large amounts, long-term, or by the wrong person. The safety section below covers this in detail.
How It's Used Today
In mainstream medicine, crude liver extract is no longer a standard treatment for anemia — it has been replaced entirely by B12 and iron. The contemporary "uses" of liver preparations are essentially nutritional:
- As a food. Eating modest portions of liver (a serving every week or two) is a time-honored, inexpensive way to get B12, heme iron, folate, and vitamin A from whole food. This is the most sensible and best-understood "use," and it's covered on the Beef Liver page.
- As a desiccated-liver supplement. Some people take capsules as a convenient animal-source multivitamin-like product. If you choose this, treat it like a potent nutrient source, not a casual daily habit: keep portions modest, account for the vitamin A and iron it contributes (alongside any other supplements and your diet), and choose a reputable brand that tests for contaminants.
- Realistic dosing. There is no medically established "dose" of liver extract for anemia, precisely because medicine moved to B12 and iron instead. For desiccated-liver supplements, more is not better — the limiting factors are the vitamin A and iron loads, not the B vitamins. Anyone using liver therapeutically for a blood problem should be working with a clinician on tested B12/iron levels rather than self-dosing an organ powder.
For an actual diagnosed deficiency, the modern standard is straightforward and far safer: B12 (injections for malabsorption or autoimmune pernicious anemia; high-dose oral tablets for many dietary or milder cases) and, for iron deficiency, an appropriate iron regimen, with the underlying cause investigated.
Safety, Cautions & Myths
This is the part the "ancestral superfood" marketing tends to leave out, and it's the most important section on the page. Liver and desiccated-liver supplements are powerful because they're nutrient-dense — and that same density is exactly what makes overuse risky.
- Vitamin A overload (hypervitaminosis A). Liver is one of the most concentrated sources of preformed vitamin A (retinol) in the human diet. Preformed vitamin A is fat-soluble and stored in the body, so it can build to toxic levels over time. Chronic excess can cause headaches, bone and joint pain, hair loss, liver damage, and elevated pressure around the brain. Large amounts are also a serious concern in pregnancy, where excess preformed vitamin A is linked to birth defects — which is why pregnant women are generally advised to limit liver and to avoid high-dose liver/retinol supplements. Stacking desiccated-liver capsules on top of an already vitamin-A-rich diet or a separate vitamin A or cod-liver-oil supplement is how people get into trouble.
- Iron overload. Liver provides highly absorbable heme iron. For most people that's a benefit, but iron, too, is stored rather than freely excreted, and the body has no efficient way to get rid of an excess. Routinely taking iron-rich supplements you don't need can contribute to overload, and the lining of the gut, joints, liver, heart, and pancreas pay the price. This is especially dangerous for people with hereditary hemochromatosis, a common genetic condition in which the body absorbs and accumulates too much iron; for them, liver and iron supplements can be actively harmful and should generally be avoided. (See the Hemochromatosis page.) Men and postmenopausal women, who don't lose iron through menstruation, are also more prone to accumulation and should not take iron-loaded supplements without a reason.
- Sourcing and contaminant quality matters. The liver is a metabolic and filtering organ, and supplement quality varies. Choose products from reputable manufacturers that test for heavy metals and contaminants, ideally from healthy, well-raised animals. "Natural" does not mean "automatically clean."
- Myth: "the natural cofactors make it work better than the isolated vitamin." The cure for pernicious anemia is built on isolated B12 — purifying the active factor is precisely what turned a brute-force food remedy into a precise medicine. Liver is a fine food source of B12 and iron, but the claim that crude liver is therapeutically superior to proper B12 or iron treatment is not supported.
- Myth: "liver detoxes you." No. Eating liver does not "cleanse" the human liver or "flush toxins." It's a nutrient-dense food, full stop — and one whose nutrients can accumulate, which is closer to the opposite of the detox marketing.
- The cause of anemia must be diagnosed first. This is the single most important safety point, expanded in the next section.
Diagnose the Anemia First
It is tempting, when you feel tired and run-down, to reach for a "blood-building" supplement like liver capsules. But fatigue is not a diagnosis, and anemia has several very different causes that need different treatments — and one of them (iron) can be made worse by guessing wrong.
- Iron-deficiency anemia needs iron — but it also needs an explanation. In adults, especially men and postmenopausal women, unexplained iron deficiency can be the first sign of bleeding somewhere in the gut, including from an ulcer or a cancer. Pouring iron in without finding the source can mask a serious problem.
- B12-deficiency anemia needs B12, and the form of treatment depends on why you're low — autoimmune pernicious anemia and other malabsorption usually need injections or high-dose oral B12, not a food source you can't absorb well.
- Folate-deficiency anemia needs folate. Importantly, taking folate when the real problem is B12 can paper over the blood test while nerve damage from B12 deficiency silently progresses — a classic trap.
- Anemia of chronic disease (from inflammation, kidney disease, or other illness) often does not respond to more iron at all, and may even be harmed by it.
The practical takeaway: if you're anemic or persistently fatigued, get a blood test that distinguishes these causes before self-treating. Liver, liver extract, and desiccated-liver capsules are food-level nutrient sources — useful in the right context, but no substitute for finding out what's actually wrong.
Key Research Papers
The original 1926 liver-therapy reports and the 1948 isolation of vitamin B12 predate digital DOIs, so those are given as authoritative archive and topic-search links; the modern reviews of B12, iron, and iron overload are linked by verified DOI.
- The Nobel Prize in Physiology or Medicine 1934 — George H. Whipple, George R. Minot, and William P. Murphy, "for their discoveries concerning liver therapy in cases of anaemia." NobelPrize.org (official archive). — The primary record of the prize that recognized liver therapy for anemia.
- Minot GR, Murphy WP. Treatment of Pernicious Anemia by a Special Diet (1926). JAMA, 87:470–476. — The landmark report that a liver-rich diet reverses pernicious anemia (PubMed topic search; the original paper predates DOIs).
- Rickes EL, Brink NG, Koniuszy FR, Wood TR, Folkers K. Crystalline Vitamin B12 (1948). Science, 107:396–397. — The isolation of the pure anti-anemia factor from liver, explaining why liver therapy worked (PubMed topic search).
- Stabler SP. (2013). Vitamin B12 Deficiency. New England Journal of Medicine, 368(2):149–160. — A modern clinical review of how B12 deficiency is diagnosed and treated, including oral versus injectable therapy. (VERIFIED)
- Carmel R. (2000). Current Concepts in Cobalamin Deficiency. Annual Review of Medicine, 51:357–375. — A thorough overview of B12 (cobalamin) deficiency, pernicious anemia, and intrinsic-factor biology. (VERIFIED)
- Hunt A, Harrington D, Robinson S. (2014). Vitamin B12 deficiency. BMJ, 349:g5226. — A practical clinical summary of recognizing and managing B12 deficiency. (VERIFIED)
- Lopez A, Cacoub P, Macdougall IC, Peyrin-Biroulet L. (2016). Iron deficiency anaemia. The Lancet, 387(10021):907–916. — A comprehensive review of the causes, diagnosis, and modern treatment of iron-deficiency anemia. (VERIFIED)
- Andrews NC. (1999). Disorders of Iron Metabolism. New England Journal of Medicine, 341(26):1986–1995. — A foundational review of how the body handles iron, including deficiency and overload. (VERIFIED)
- Fleming RE, Ponka P. (2012). Iron Overload in Human Disease. New England Journal of Medicine, 366(4):348–359. — Explains how excess iron accumulates and damages organs — the basis of the overload warning for liver/iron supplements. (VERIFIED)
- Meynard D, Babitt JL, Lin HY. (2014). The liver: conductor of systemic iron balance. Blood, 123(2):168–176. — How the body regulates iron levels (the hepcidin system), relevant to why iron overload is hard to reverse. (VERIFIED)
Live PubMed Searches
- Liver extract and pernicious anemia (history)
- Vitamin B12 deficiency: oral vs injectable treatment
- Desiccated liver supplements and vitamin A toxicity
- Hereditary hemochromatosis and dietary iron
Connections
- Beef Liver (the food)
- Vitamin B12 (Cobalamin)
- Vitamin B9 (Folate)
- Iron
- Anemia
- Hemochromatosis
- Hematology
- All Remedies