Activated Charcoal
Activated charcoal is one of the rare old remedies that turned out to be genuinely important — but for a much narrower job than the modern wellness aisle suggests. In the 1926 U.S. Dispensatory, doctors gave it for food poisoning, gas, and "toxins," and the core idea was sound: charcoal is a sponge for poisons. Today it is a real piece of emergency medicine. In a hospital, when someone has swallowed too much of certain pills or poisons, a single dose of activated charcoal given soon after — ideally within an hour — can soak up the drug before the body absorbs it. That is its proven, lifesaving use. What it is not is a daily "detox" or "cleanse." Taken regularly with food and pills, it does nothing helpful and can quietly soak up your nutrients and your medications instead — including birth control. This page separates the real emergency medicine from the marketing, and lays out the safety facts the trendy lemonade ads leave out.
If you suspect a poisoning or overdose, this is a medical emergency. In the United States call Poison Control at 1-800-222-1222 (free, 24/7) or 911 right now. Do not give activated charcoal at home unless a poison-control specialist or clinician tells you to — given wrong, it can be dangerous.
Table of Contents
- What Activated Charcoal Actually Is
- Historical Medical Use (1926 U.S. Dispensatory)
- Poisoning & Overdose: The Real Emergency Use
- What It Binds — and What It Does Not
- Intestinal Gas & Bloating
- The "Detox," "Cleanse" & Whitening Myths
- How It's Used Today
- Safety, Cautions & Myths
- Key Research Papers
- Connections
- Featured Videos
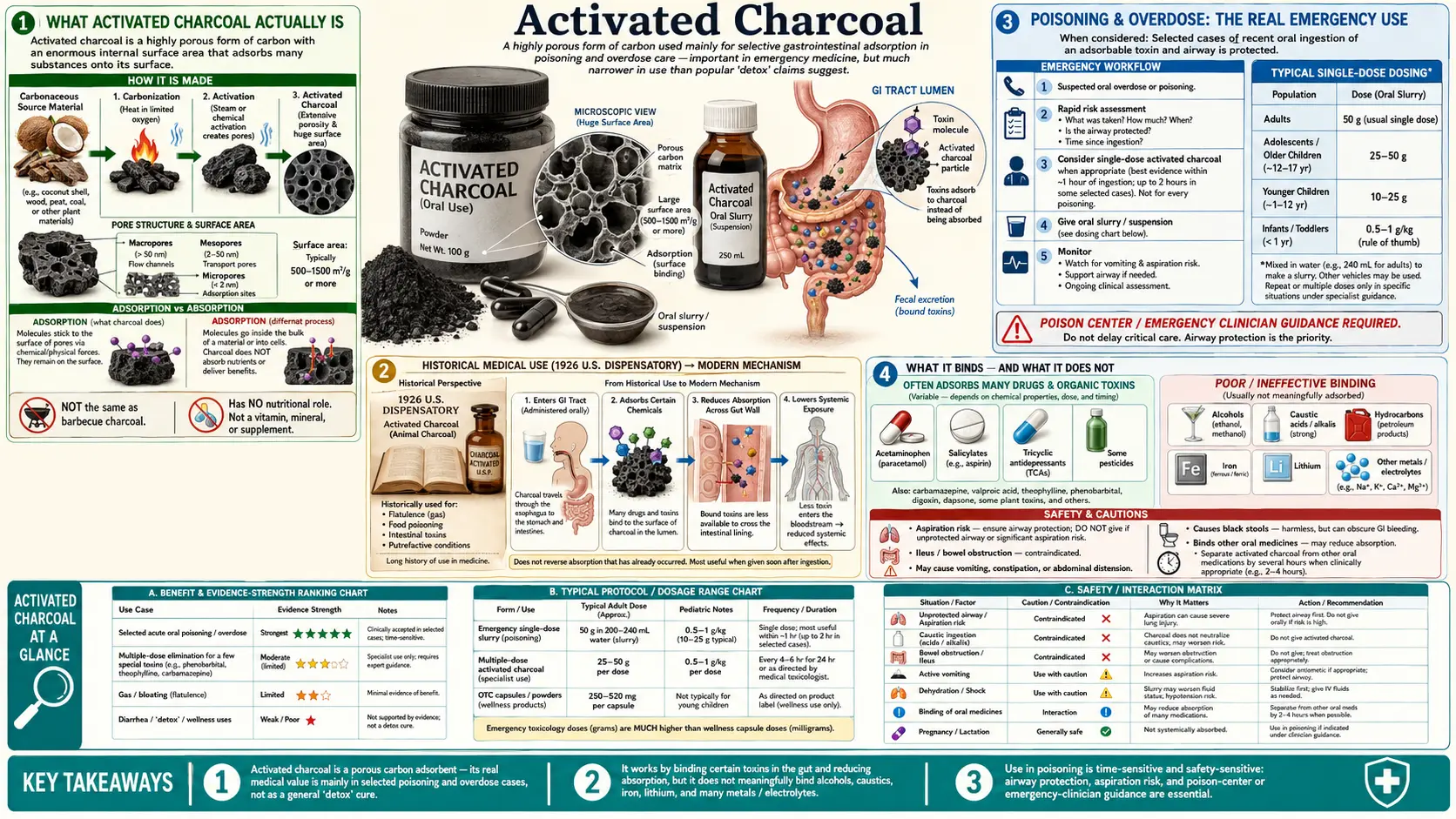
What Activated Charcoal Actually Is
Activated charcoal is ordinary carbon — made by burning a plant material like coconut shells, wood, or peat — that has then been "activated" by heating it with steam or certain gases at very high temperature. That activation step blasts a vast network of microscopic pores into each particle, the way a sea sponge is riddled with holes. The result is a black powder with an almost unbelievable amount of internal surface area: a single gram can have a surface area of roughly 500 to 1,500 square meters — a few teaspoons can carry the surface area of a football field, all folded up inside.
That enormous surface is the whole point. Charcoal works by a process called adsorption — note the "d." It is different from absorption, where one thing soaks into another like water into a sponge. In ad-sorption, molecules stick to the outside surface of the charcoal, like burrs catching on a wool sweater. Because charcoal has so much surface, it can grab and hold a remarkable quantity of other molecules.
The catch — and it is the catch that explains both its powers and its limits — is that charcoal is not picky. It will grab a poison, but it will just as happily grab a vitamin, a mineral, or your blood-pressure pill. It also only works on what it can physically reach: things still sitting in your stomach and intestines. Once a drug or poison has already crossed from the gut into your bloodstream, swallowing charcoal can no longer pull it back out (with a few special exceptions, covered below). Charcoal is also not digested or absorbed itself — it passes straight through and leaves in the stool, taking whatever it grabbed along with it. That is why your stool turns black after taking it: harmless, expected, and the visible proof that it went through unchanged.
Historical Medical Use (1926 U.S. Dispensatory)
Charcoal as a remedy is genuinely ancient — it appears in Egyptian papyri and in the writings of Hippocrates — but the version doctors recognize today came together in the 1800s and was firmly established by the early twentieth century. In the 1926 U.S. Dispensatory (the 21st edition of Wood & LaWall's Dispensatory of the United States of America, the authoritative American drug reference of its day), activated charcoal — listed in the carbon/Carbo tradition — was used for three things: food poisoning, intestinal gas, and "toxins" swallowed by mouth.
Here is the honest historical framing: that 1926 picture was mostly right about the mechanism and partly right about the use. Physicians of the era understood that charcoal soaked up irritating and poisonous substances in the gut, and there were dramatic demonstrations of this even before then — most famously, a French pharmacist named Touéry reportedly swallowed a lethal dose of strychnine mixed with charcoal in front of a medical academy in 1831 and survived. So the core belief that charcoal could neutralize swallowed poisons was real science, not folklore.
Where the 1926 use needs reframing is in two places. First, "toxins" in that era was a loose word that lumped together genuine swallowed poisons (where charcoal truly helps) with a vaguer notion of self-generated "bad humors" in the bowel (where it does not). Second, the routine use for everyday "gas" oversold a benefit that, as we will see, modern controlled trials have found to be inconsistent at best. The legitimate, time-tested core of the 1926 use — charcoal for swallowed poisons — survived and became one of the foundations of modern emergency toxicology. The looser "detox the bowel of toxins" framing did not survive scrutiny, and the modern marketing version of it has no evidence behind it.
Poisoning & Overdose: The Real Emergency Use
This is what activated charcoal is genuinely for, and it is a big deal. When a person swallows a dangerous overdose of certain medications or a poison, much of that substance sits in the stomach and intestine for a while before the body absorbs it into the bloodstream. If activated charcoal reaches it during that window, the charcoal binds the poison so it travels out in the stool instead of being absorbed. Less drug absorbed means a milder, safer poisoning. Poison-control centers and emergency departments use it for exactly this.
The one-hour window
Timing is everything, and this is the single most important fact about charcoal in poisoning. It works best when given early — ideally within about one hour of the poison being swallowed, while most of it is still in the gut. The widely used international guideline, the position paper on single-dose activated charcoal from the American Academy of Clinical Toxicology and the European Association of Poisons Centres (Chyka 2005), concluded that charcoal can reduce drug absorption substantially when given within an hour, but that there is little evidence of meaningful benefit when it is given later than that for most poisons. After the first hour, the benefit drops off because the poison has increasingly moved out of reach into the bloodstream.
This one-hour rule is precisely why home "detox" use makes no sense and emergency use is decided by professionals: the decision depends on what was swallowed, how much, how long ago, and whether the person can safely swallow — judgment calls for Poison Control or an emergency clinician, not a guess in the kitchen.
Single-dose is the standard
For the great majority of poisonings, a single dose of activated charcoal is the standard approach — typically a flavored slurry the patient drinks, or, if needed, given through a tube. A common adult dose is on the order of 25–100 grams, often described as roughly a 10-to-1 ratio of charcoal to the estimated amount of drug swallowed, but in practice this is a clinical decision, not a home recipe.
Multiple-dose charcoal — a narrower, hospital-only tactic
For a small number of specific, life-threatening poisons, doctors sometimes give repeated doses of charcoal over hours. This can do two things: keep binding drug that is still being released from a slow-dissolving pill mass, and, for a few drugs, actually pull drug back out of the bloodstream as it recirculates through the gut (a process informally called "gut dialysis"). This is reserved for particular agents — examples studied include theophylline, carbamazepine, dapsone, phenobarbital, and quinine.
It is worth being honest that even here the evidence is mixed. In a landmark randomized trial in Sri Lanka (de Silva 2003), repeated doses of charcoal reduced deaths in people who had swallowed seeds of the highly toxic yellow oleander plant (a source of heart-stopping cardiac glycosides) — a genuinely positive result. But a much larger randomized trial of multiple-dose charcoal across a broad mix of self-poisonings (Eddleston 2008) found no reduction in deaths overall. The lesson is not that charcoal is useless — it is that its benefit is real but specific, depends heavily on the poison and the timing, and is a decision for toxicology experts.
What It Binds — and What It Does Not
Because charcoal only works by physically sticking to molecules in the gut, there is a hard rule: if a substance does not stick to charcoal, charcoal cannot help. This is one of the most under-appreciated and important safety facts, because relying on charcoal for a poison it cannot bind wastes the precious early minutes during which a real antidote or treatment could have worked.
Charcoal does bind many common drugs and toxins, including many painkillers, antidepressants, heart and seizure medications, and many plant and chemical poisons.
Charcoal does not meaningfully bind several important things — and for these it is useless or worse:
- Alcohols — ethanol (drinking alcohol), methanol, ethylene glycol (antifreeze), and isopropanol. Charcoal does not help an alcohol or antifreeze poisoning; these need entirely different treatment.
- Metals and metal salts — iron, lithium, and similar. Charcoal does not bind them, so it is the wrong tool for an iron or lithium overdose.
- Caustics — strong acids and alkalis (such as drain cleaner or lye). Charcoal does not bind them and can coat the burned tissue, hide the injury, and make it impossible for doctors to see the damage during endoscopy.
- Hydrocarbons — petroleum products such as gasoline, kerosene, and many solvents. Charcoal does not help, and trying to give it raises the danger of these being breathed into the lungs.
The simple takeaway: charcoal is powerful for the things it binds and completely beside the point for the things it does not — which is exactly why the choice belongs to Poison Control or an emergency clinician who knows what was swallowed.
Intestinal Gas & Bloating
The 1926 use for gas points to charcoal's other widely marketed role, sold today as anti-flatulence tablets. The theory is reasonable: charcoal could adsorb some of the gases produced by bacteria in the colon. The reality is that the human evidence is genuinely mixed, and this is a place where honesty matters more than the product label.
On the positive side, a small double-blind study (Jain 1986) reported that activated charcoal reduced the number of gas episodes and bloating after a gas-producing meal. On the negative side, a careful controlled study from a leading intestinal-gas research group (Suarez 1999) found that activated charcoal did not reduce the amount of gas the colon's bacteria released, nor the symptoms. Overall, reviews conclude that charcoal may modestly help some people with gas and bloating, but the benefit is inconsistent and far from guaranteed — quite different from the slam-dunk it is in poisoning.
If you do try a charcoal product for occasional gas, treat it as a short-term, occasional aid, not a daily habit — and keep the medication-spacing warning below firmly in mind, because the same charcoal that might soak up gas can also soak up any pill you take near it.
The "Detox," "Cleanse" & Whitening Myths
Here is where modern marketing parts ways with the science. Activated charcoal now shows up in juices, lemonades, ice cream, face masks, toothpaste, and "daily detox" capsules, all built on the appealing-but-wrong idea that swallowing charcoal regularly will "pull toxins out of your body" or "cleanse" you. It will not, and it is worth understanding exactly why.
- There is no toxin pool for it to mop up. Your liver and kidneys continuously clear genuine metabolic waste and process foreign substances — that is what "detox" actually means, and it happens in your organs and bloodstream, around the clock, for free. Activated charcoal works only on what is physically present inside the gut. It cannot reach your blood, your liver, your fat, or your cells, so it cannot remove any "stored toxin" the wellness ads imagine. There is no good evidence it improves any health marker in a healthy person.
- It does the opposite of helpful with food. Taken with or near meals, charcoal can bind nutrients — vitamins and minerals — and carry them out unabsorbed. A "detox" drink consumed regularly is, at best, a non-event and, at worst, slowly working against your nutrition.
- It can sabotage your medications — including birth control. This is the most serious part of the myth. The same non-selective binding that makes charcoal useful in an overdose means a "daily detox" capsule can reduce how much of your real medication you absorb. This includes oral contraceptives — a charcoal habit taken near the pill could lower its effectiveness and, in theory, lead to unintended pregnancy — as well as thyroid medication, antidepressants, heart medications, and many others. Any medication that matters should be kept well away from charcoal.
- "Detox" hangover cures don't work. A popular claim is that charcoal-laced drinks prevent or cure hangovers by soaking up the alcohol. As covered above, charcoal does not bind alcohol, so this is simply false.
- Charcoal toothpaste is abrasive, not whitening. Dental research has not shown activated-charcoal toothpaste to safely whiten teeth. Many such products are abrasive enough to wear down enamel over time, lack fluoride (removing real cavity protection), and can lodge dark particles in the gum line and around fillings. Dental groups have warned against routine use.
None of this contradicts charcoal's real value. It is precisely because charcoal is a powerful, non-selective binder that it is excellent in a one-time emergency and a bad idea as a daily lifestyle product.
How It's Used Today
Legitimately, activated charcoal lives in a few well-defined places:
- Emergency poisoning treatment — the central, evidence-based use, given under the direction of Poison Control or in an emergency department, usually as a single oral or tube-administered dose for suitable poisonings caught early.
- A small set of severe poisonings where multiple-dose charcoal is considered by toxicologists, as described above.
- Occasional anti-gas product — sold over the counter for flatulence, with the modest, inconsistent benefit noted above.
- Some hospital and clinical roles — for example, certain charcoal-based products are used to bind specific drugs or bile acids in particular medical situations, and charcoal is used industrially in water and air filtration. These are distinct from swallowing "detox" capsules.
On dosing: for poisoning, the dose is a clinical decision (commonly tens of grams for an adult) and is not something to attempt at home. For an over-the-counter gas product, follow the package directions and the medication-spacing rule below. There is no legitimate "daily wellness" dose, because there is no legitimate daily wellness use.
Safety, Cautions & Myths
Activated charcoal is not the harmless novelty its trendy uses suggest. The cautions the lemonade ads leave out:
- It binds your medications — space them apart. Because charcoal grabs drugs non-selectively, any medication taken near it may be partly soaked up and lost. This includes oral contraceptives (a real risk of reduced effectiveness), thyroid medication, antidepressants, heart and blood-pressure drugs, and many more. Keep regular medications well away from any charcoal product — typically several hours apart — and never take charcoal casually if you depend on a daily medication.
- It binds nutrients too. Taken with food or used chronically, charcoal can reduce absorption of vitamins and minerals. This is one more reason it is not a daily supplement.
- Aspiration is the big danger. If charcoal is swallowed (or vomited) by someone who is drowsy, confused, having seizures, or otherwise cannot protect their airway, it can go down into the lungs. Charcoal in the lungs causes a severe, sometimes fatal pneumonia-like injury. This is why charcoal should never be forced on a sleepy or unresponsive person at home, and why clinicians protect the airway first.
- It is useless or harmful for certain poisons. As detailed above, charcoal does not help with alcohols (including drinking alcohol and antifreeze), metals such as iron and lithium, caustics (acids/alkalis), or hydrocarbons (gasoline, solvents) — and giving it for caustics or hydrocarbons can make things worse. Relying on it for these wastes critical time.
- Constipation and black stools. Black stools are harmless and expected. But charcoal — especially repeated doses — can cause constipation and, rarely, a blockage (bowel obstruction), so it is avoided when the gut is not moving normally.
- Not for routine or "detox" use. There is no health benefit to taking activated charcoal regularly, and real downside (lost nutrients, lost medication effect). It is an emergency tool, not a daily supplement.
- In a real poisoning, get expert help first. Do not give charcoal at home on your own judgment. Call Poison Control at 1-800-222-1222 or 911; they will tell you whether charcoal is appropriate and, far more often, will direct other care. Bring the container or a photo of what was swallowed if you can.
Key Research Papers
- Chyka PA, Seger D, Krenzelok EP, Vale JA (American Academy of Clinical Toxicology / European Association of Poisons Centres and Clinical Toxicologists). Position Paper: Single-Dose Activated Charcoal. Clinical Toxicology, 43(2):61–87 (2005). — The major international guideline: single-dose charcoal can substantially cut drug absorption when given within about an hour of ingestion, with little proven benefit later, and should not be used routinely.
- Juurlink DN. Activated charcoal for acute overdose: a reappraisal. British Journal of Clinical Pharmacology, 81(3):482–487 (2016). — A clear, balanced clinical review of when charcoal helps in overdose and when it does not, emphasizing early administration and a protected airway.
- Zellner T, Prasa D, Färber E, Hoffmann-Walbeck P, et al. The Use of Activated Charcoal to Treat Intoxications. Deutsches Ärzteblatt International, 116(18):311–317 (2019). — A modern overview of charcoal in poisoning, including which substances it does and does not bind and the importance of airway safety.
- Eddleston M, Juszczak E, Buckley NA, et al. Multiple-dose activated charcoal in acute self-poisoning: a randomised controlled trial. The Lancet, 371(9612):579–587 (2008). — A large randomized trial that found multiple-dose charcoal did not reduce deaths across a broad mix of self-poisonings — important evidence that its benefit is specific, not universal.
- de Silva HA, Fonseka MMD, Pathmeswaran A, et al. Multiple-dose activated charcoal for treatment of yellow oleander poisoning: a single-blind, randomised, placebo-controlled trial. The Lancet, 361(9373):1935–1938 (2003). — A randomized trial in which repeated-dose charcoal reduced deaths from highly toxic yellow oleander seed poisoning — a genuine positive result for a specific, life-threatening poison.
- Jain NK, Patel VP, Pitchumoni CS. Activated Charcoal, Simethicone, and Intestinal Gas: A Double-Blind Study. Annals of Internal Medicine, 105(1):61–62 (1986). — A small double-blind study reporting that activated charcoal reduced gas symptoms and bloating after a gas-producing meal.
- Suarez FL, Furne J, Springfield J, Levitt MD. Failure of Activated Charcoal to Reduce the Release of Gases Produced by the Colonic Flora. American Journal of Gastroenterology, 94(1):208–212 (1999). — A controlled study from a leading gas-research group finding that activated charcoal did not reduce gas production or symptoms — the counterweight that makes the gas evidence genuinely mixed.
Live PubMed Searches
- Activated charcoal in poisoning & overdose (randomized trials)
- Activated charcoal & medication / oral-contraceptive interactions
- Activated charcoal for intestinal gas & flatulence
- Activated charcoal & "detox" / detoxification claims
Connections
- Detox Protocols
- Liver Detox
- Liver Cleansing
- Parasites
- Natural Constipation Relief
- Gut Healing
- Toxins
- Heavy Metals
- All Remedies