Lithium Carbonate
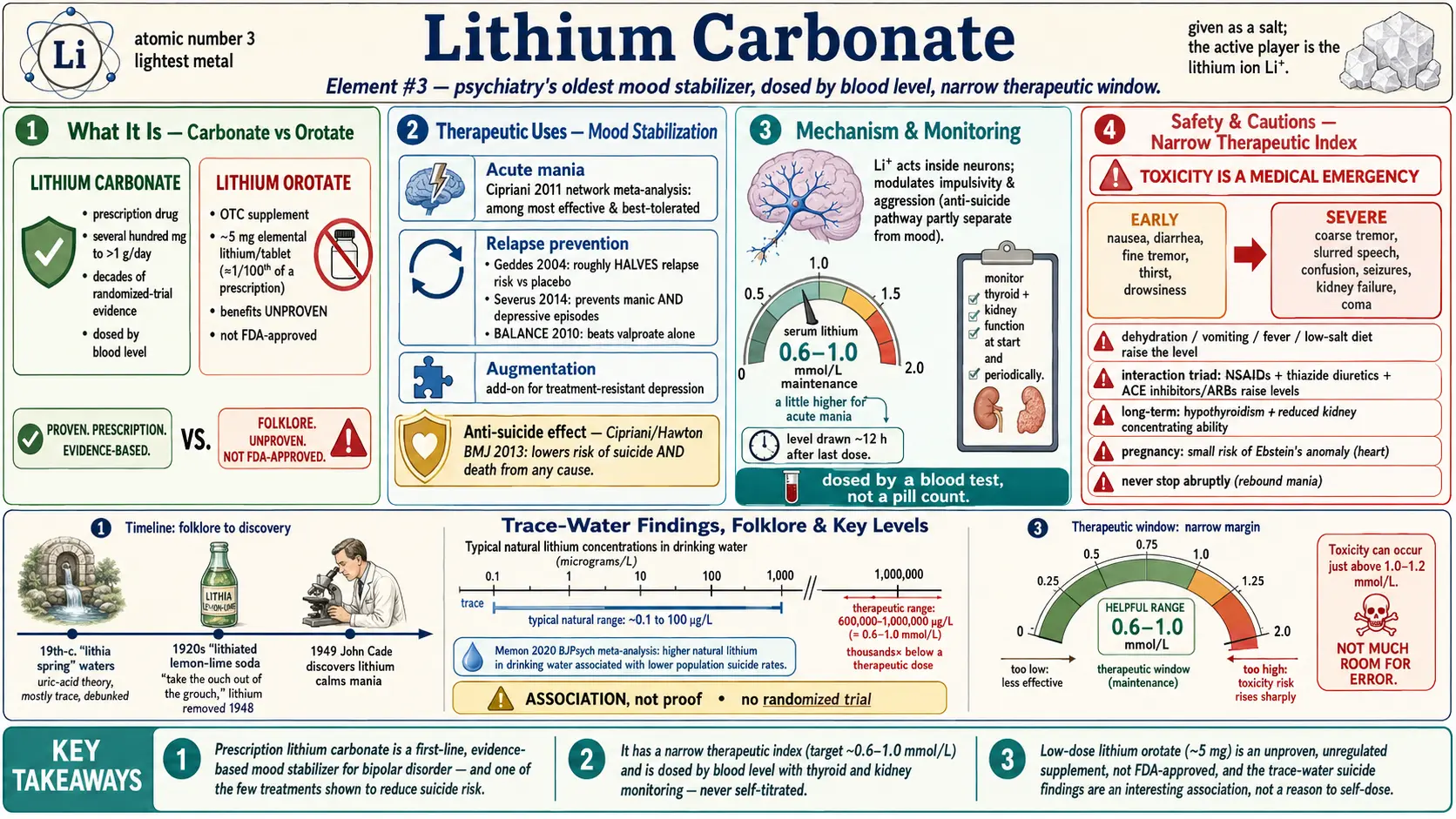
Lithium is one of the oldest treatments still in everyday use in psychiatry, and one of the most quietly remarkable. The same lithium that fizzes in the periodic table as the third-lightest element of all was once dissolved in spa waters that people traveled across the country to bathe in, and was even added to a lemon-lime soda marketed to "take the ouch out of the grouch." Today, in the carefully dosed form of lithium carbonate, it is a first-line, well-proven mood stabilizer for bipolar disorder — and one of the very few psychiatric medicines shown to lower the risk of suicide. It is also a medicine that demands respect: it has a narrow margin between a helpful dose and a toxic one, so it is taken under a doctor's care with regular blood tests. This page separates the genuine science from the spa-water folklore, and is honest about a popular newcomer — low-dose lithium orotate supplements — whose claimed benefits are, so far, unproven.
Table of Contents
- Historical Medical Use: Springs, Soda & the 1949 Discovery
- What It Actually Is (the Element, Carbonate vs Orotate)
- Bipolar Disorder & Mood Stabilization
- The Anti-Suicide Effect
- Trace Lithium in Drinking Water
- Low-Dose Lithium Orotate (Unproven)
- How It's Used Today
- Safety, Cautions & Myths
- Key Research Papers
- Connections
- Featured Videos
Historical Medical Use: Springs, Soda & the 1949 Discovery
Lithium's medical story begins long before anyone understood what it actually did. In the second half of the 19th century, doctors became convinced that many ailments — gout, "gravel" (kidney stones), rheumatism, even some forms of low mood — were caused by a build-up of uric acid in the body. Lithium salts dissolve uric-acid crystals nicely in a test tube, so physicians reasoned (incorrectly, as it turned out) that drinking lithium would dissolve those crystals inside people too. This launched a fashion for "lithia waters." Natural springs advertised their lithium content, bottled "lithia water" was sold by the case, and well-to-do patients traveled to spa towns to drink and bathe in waters promoted as rich in lithium. In truth, most of these springs contained only trace amounts — far too little to do what was claimed — and the uric-acid theory of mood and disease did not hold up. By the time of the United States Dispensatory of 1926, lithium salts were on the shelf chiefly as remedies for gout and uric-acid conditions, a use that has since been abandoned.
The folklore reached its most famous form in the soft-drink aisle. In the late 1920s a "lithiated" lemon-lime soda was launched containing lithium citrate, advertised with slogans promising it would "take the ouch out of the grouch" and cure a hangover. Lithium was removed from such drinks in 1948 after the U.S. government tightened the rules on adding lithium to beverages and food. There is a widely repeated anecdote that this lithiated soda was an ancestor of the modern 7Up. Treat this as etymology and folklore, not established fact — historians dispute whether the original formula truly contained lithium and how directly it connects to the drink sold today, and the company itself has not confirmed the lithium story. It is a charming piece of cultural history; it is not evidence of anything medical.
The real breakthrough came in 1949, and it had nothing to do with springs or soda. An Australian psychiatrist, John Cade, working in a small repatriation-hospital lab, was testing whether something in the urine of people with mania might be toxic. He used lithium urate to dissolve uric acid for his experiments, injected lithium into guinea pigs, and noticed it made them strikingly calm. He then tried lithium carbonate in a handful of patients with severe, chronic mania — and several improved dramatically, with one long-hospitalized man well enough to go home. Cade published his observations that year, and lithium became the first medicine ever shown to control mania. It was slow to be accepted (lithium had a frightening reputation from a 1940s episode in which it was used carelessly as a salt substitute and caused fatal poisonings), but careful research over the following decades established it as a genuine, evidence-based treatment. So the honest summary is this: the spa and soda history is real cultural history built on a mistaken theory, while the actual psychiatric value of lithium was discovered independently, in 1949, and proven by modern clinical trials.
What It Actually Is (the Element, Carbonate vs Orotate)
Lithium is a chemical element — a soft, silvery metal, atomic number 3, the lightest metal there is. You will never swallow the pure metal (it reacts violently with water); instead, lithium is given as a salt, a stable compound in which lithium is paired with something else. What actually does the work in the brain is the lithium ion (written Li+), a tiny positively charged particle. The "carbonate" or "orotate" part is just the carrier that delivers that ion; once dissolved in the body, the lithium ion is the active player regardless of which salt it came in.
Lithium carbonate is the standard prescription form (it also comes as lithium citrate in a liquid). It is a regulated medicine, taken in fairly substantial daily amounts — typically several hundred milligrams to over a gram of the carbonate salt per day — and it is dosed by measuring the lithium level in your blood, not by guessing. This is the form with decades of randomized-trial evidence behind it.
Lithium orotate is a different salt (lithium paired with orotic acid) sold as an over-the-counter dietary supplement, usually providing only about 5 mg of elemental lithium per tablet — very roughly on the order of one-hundredth of the elemental lithium in a typical carbonate prescription. Marketers claim orotate slips into cells more efficiently, so a tiny dose supposedly does the work of a large one. As the orotate section below explains, that claim rests largely on a single old animal study and is not supported by good human evidence. The key point to hold onto: carbonate is a proven prescription drug used at carefully monitored doses; orotate is an unregulated supplement at a tiny dose whose benefits have not been demonstrated in people.
Bipolar Disorder & Mood Stabilization
Bipolar disorder is an illness of mood swings — episodes of mania or hypomania (abnormally high, energized, or irritable states, sometimes with reckless behavior or psychosis) alternating with episodes of depression. A mood stabilizer is a medicine that both calms acute episodes and, taken long-term, makes future episodes less frequent and less severe. Lithium is the original and still one of the best mood stabilizers, and unlike most of the 1926-era remedies on this site, it earns that title through modern gold-standard research.
For acute mania, a large network meta-analysis by Cipriani and colleagues (2011) compared the antimanic drugs head to head and found lithium among the more effective and best-tolerated options for bringing a manic episode under control — performing comparably to several antipsychotics and better than some alternatives. For preventing relapse — arguably what matters most over a lifetime — the evidence is even stronger. A systematic review of randomized trials by Geddes and colleagues (2004) found that long-term lithium roughly halved the risk of relapse compared with placebo, with its clearest effect on preventing manic relapses. A later, broader meta-analysis by Severus and colleagues (2014) confirmed that lithium prevents both manic and, to a meaningful degree, depressive episodes, and concluded it should remain a first-line maintenance treatment.
Lithium also holds up against newer drugs. The BALANCE trial (2010), a randomized study in people with bipolar I disorder, found that lithium (alone or combined with valproate) was more effective for long-term relapse prevention than valproate by itself. This is a striking result: a medicine first tried in 1949 still outperforms or matches drugs developed half a century later. That is why, despite the monitoring it requires, lithium remains a cornerstone of bipolar treatment in modern guidelines worldwide. It does not work for everyone — some people respond beautifully ("lithium responders"), others less so — but for those it suits, it can be genuinely life-changing, smoothing the violent swings into something livable.
The Anti-Suicide Effect
One of the most important and least appreciated facts about lithium is that it appears to reduce the risk of suicide — something very few psychiatric treatments have ever convincingly shown. This matters enormously because bipolar disorder and recurrent depression carry a tragically high suicide risk, and reducing deaths, not just symptoms, is the ultimate goal.
The landmark evidence is a meta-analysis by Cipriani, Hawton, and colleagues, published in the BMJ in 2013, which pooled randomized controlled trials in people with mood disorders. It found that, compared with placebo, lithium was associated with a significantly lower risk of suicide and of death from any cause. The protective effect was seen across both bipolar disorder and unipolar (ordinary) depression. Importantly, this signal comes from randomized trials, the strongest kind of evidence, not just from observation.
How lithium does this is not fully understood, and honesty requires saying so. The anti-suicide effect seems to be partly separate from simply preventing mood episodes — it may relate to lithium's effects on impulsivity and aggression. The size of the benefit and exactly who gains the most are still debated, and a single landmark trial designed specifically to test lithium for suicide prevention in high-risk veterans did not find a clear reduction, a reminder that the picture is not settled. But the overall weight of evidence has been strong enough that this remains one of the central reasons clinicians value lithium, and a reason it is sometimes kept on board even when other medicines might control the mood swings.
Trace Lithium in Drinking Water
Here is where the old "lithia spring" idea takes a genuinely intriguing modern turn — and where careful, honest framing matters most. Lithium occurs naturally in rocks and soil, so tap water in different regions contains very different trace amounts of lithium: amounts far, far smaller than any medicine, measured in micrograms per liter. Researchers have asked a fascinating question: do communities whose drinking water happens to contain more natural lithium have lower suicide rates?
A number of ecological studies — studies that compare whole populations, region by region — have reported exactly that pattern. The idea was popularized by a 1990 study of Texas counties by Schrauzer and Shrestha, and similar correlations have since been reported in Japan, Austria, England, Greece, and elsewhere. A 2015 systematic review (Vita and colleagues) and a more rigorous 2020 systematic review and meta-analysis in the British Journal of Psychiatry (Memon and colleagues) both concluded that, on balance, higher natural lithium levels in drinking water are associated with lower suicide rates across populations.
It is genuinely tempting to leap from this to "we should add lithium to the water supply," and you will see exactly that suggested online. Resist the leap. This is hypothesis-generating evidence, not proof. Ecological studies have a built-in trap (the "ecological fallacy"): a correlation seen across whole regions does not prove the effect holds for individuals, and these studies cannot rule out other regional differences — wealth, rural-versus-urban living, climate, healthcare access, even other minerals in the water — that travel alongside lithium levels. No randomized trial has ever tested whether trace lithium in water actually prevents suicides in individuals, and the doses involved are thousands of times smaller than a therapeutic dose. So the honest verdict is: this is a real, repeatable, and scientifically interesting association that justifies further research — and nothing more. It is not a reason to take lithium supplements, and it is not established public-health policy.
Low-Dose Lithium Orotate (Unproven)
Riding on the genuine fame of prescription lithium and the intriguing trace-water findings, low-dose lithium orotate has become a popular over-the-counter supplement, widely promoted for mood, "calm," sleep, irritability, and even as a supposed brain-protective "longevity" nutrient. It is sold without a prescription, typically at around 5 mg of elemental lithium per tablet. The marketing is confident. The evidence is not.
The central claim is that orotic acid acts as a special "carrier" that ushers lithium into cells far more efficiently than carbonate, so a tiny dose does the work of a big one. This idea traces largely to a single 1970s animal study (in rats) and the promotion of one mid-century researcher; it has never been confirmed by solid human pharmacokinetic studies. A 2021 review in Brain and Behavior by Pacholko and Bekar examined the "superior option" claim carefully and concluded that the supposed advantages of orotate are not established — there are no adequate controlled human trials showing low-dose orotate treats any psychiatric condition, and the cellular-uptake story is unproven in people. In short, the headline justification for the product does not currently stand up.
So where does that leave the honest reader? Lithium orotate is not FDA-approved for any condition, and its benefits are unproven. It is not a tested treatment for bipolar disorder, depression, or anxiety, and it must never be used as a substitute for prescribed lithium carbonate or any other psychiatric medicine. The doses are too low to expect the proven mood-stabilizing or anti-suicide effects of prescription lithium, yet — because it is an unregulated supplement — actual lithium content can vary between products and brands, and stacking multiple tablets or combining them with other lithium sources is not harmless. If you are drawn to it because of low mood or mood swings, the responsible step is to talk to a clinician about treatments that are actually proven to work, rather than to self-experiment with an unproven supplement.
How It's Used Today
In modern medicine, the proven, mainstream use of lithium is prescription lithium carbonate (or citrate) for bipolar disorder — both to treat acute manic episodes and, especially, as a long-term maintenance treatment to prevent future episodes. It is sometimes added to an antidepressant to boost the response in difficult-to-treat (treatment-resistant) unipolar depression, a strategy called augmentation. It is also valued, as described above, for its association with reduced suicide risk. These are real, guideline-supported uses, prescribed and supervised by a doctor.
What makes lithium unusual among medicines is that it is dosed by a blood test rather than by a fixed pill count. Because the gap between a helpful level and a toxic level is small, clinicians measure the serum lithium concentration and adjust the dose to land in a target therapeutic window (commonly around 0.6–1.0 millimoles per liter for maintenance, sometimes a little higher for acute mania). Levels are usually checked drawn about 12 hours after the last dose. Alongside the lithium level, doctors monitor thyroid function and kidney function at the start and periodically thereafter, because long-term lithium can affect both (see Safety). This monitoring is not a sign that lithium is dangerous to use — it is precisely what makes it safe to use, and millions of people take it successfully for years or decades within this framework.
The honest counterpoint is the supplement aisle. Low-dose lithium orotate is "used today" in the sense that it is widely sold and taken — but, as the section above makes clear, that popular use is not backed by evidence, is not FDA-approved, and is not a recognized medical treatment. Popularity is not proof.
Safety, Cautions & Myths
Lithium is a genuinely valuable medicine, but it is one that must be respected. The single most important fact about it is its narrow therapeutic index: the dose (and blood level) that helps is uncomfortably close to the dose that harms. A level that is therapeutic for one person can tip into toxicity with only a modest rise. This is why prescription lithium is always taken with regular blood monitoring and never casually self-titrated. Please read this section carefully.
- Lithium toxicity is real and can be dangerous. A systematic review of lithium's toxicity profile by McKnight and colleagues (2012) documents its adverse effects clearly. Early signs of rising lithium levels include nausea, diarrhea, a fine hand tremor that worsens, increased thirst and urination, drowsiness, and muscle weakness. More severe toxicity causes a coarse tremor, slurred speech, confusion, unsteadiness, vomiting, and — at high levels — seizures, kidney failure, and coma. Severe lithium toxicity is a medical emergency. If you take lithium and develop these symptoms, seek urgent care and have your level checked.
- Dehydration and anything that raises the level is the classic danger. Because lithium is handled by the kidneys and tracks with the body's salt and water balance, anything that concentrates it can push you toward toxicity: vomiting or diarrhea, fever and heavy sweating, sudden low-salt diets, or simply not drinking enough during hot weather or illness. Sick-day rules and steady fluid and salt intake matter.
- Drug interactions are a major cause of toxicity. Several very common medicines raise lithium levels by changing how the kidneys handle it. The big three to know are NSAID painkillers (such as ibuprofen and naproxen — over-the-counter pain relievers people take without thinking), diuretics ("water pills," especially thiazides), and ACE inhibitors and ARBs (common blood-pressure drugs). Combining these with lithium without dose adjustment and monitoring can be hazardous. Always tell every prescriber and pharmacist that you take lithium, and check before starting any new medicine, including over-the-counter ones.
- Long-term effects on the thyroid and kidneys. Over months and years, lithium can reduce thyroid function (causing hypothyroidism, which is usually manageable with thyroid hormone and is not a reason to stop lithium in most cases) and can affect the kidneys — most commonly causing the kidneys to concentrate urine less well (leading to thirst and frequent urination), and, in a minority of long-term users, a gradual decline in kidney function. This is exactly why thyroid and kidney tests are part of routine monitoring; problems caught early can be managed.
- Pregnancy. Lithium taken in early pregnancy is associated with a small increased risk of a heart malformation in the baby known as Ebstein's anomaly. The absolute risk is low, and for some women with severe bipolar disorder the risk of stopping lithium (a dangerous relapse) can outweigh it — but this is a decision that must be made carefully with an obstetrician and psychiatrist, never alone. Anyone who is pregnant, planning pregnancy, or breastfeeding should discuss lithium with their doctor.
- Never stop lithium abruptly on your own. Suddenly stopping lithium can trigger a rebound manic episode and may blunt how well it works if restarted. Changes should be made gradually and under medical guidance.
Myths to put to rest. First, lithium is not a "natural, gentle mineral supplement you can dose yourself" — the proven prescription drug is a precisely monitored medicine, and treating it like a casual supplement is how people get hurt. Second, the popular low-dose orotate form is not a proven, safer "lithium lite" that delivers the medicine's benefits without the risks; its benefits are unproven and its lithium content is unregulated. Third, the trace-lithium-in-water findings, however intriguing, do not mean you should buy lithium supplements "to get what's missing from your water." And finally, lithium is not the obsolete relic some assume — it remains a first-line, life-saving treatment that newer drugs have not surpassed. The single safe path with lithium is a prescription, a clinician, and regular blood tests.
Key Research Papers
- Cade JFJ. (1949). Lithium Salts in the Treatment of Psychotic Excitement. Medical Journal of Australia, 2(10):349–352. — The historic paper that launched modern lithium therapy, reporting that lithium carbonate calmed patients with chronic mania. (PubMed search link — original 1949 article; no reliable modern DOI.)
- Cipriani A, Barbui C, Salanti G, et al. (2011). Comparative Efficacy and Acceptability of Antimanic Drugs in Acute Mania: A Multiple-Treatments Meta-Analysis. The Lancet, 378(9799):1306–1315. — A network meta-analysis ranking treatments for acute mania, finding lithium among the more effective and better-tolerated options. (PMID: 21851976)
- Geddes JR, Burgess S, Hawton K, Jamison K, Goodwin GM. (2004). Long-Term Lithium Therapy for Bipolar Disorder: Systematic Review and Meta-Analysis of Randomized Controlled Trials. American Journal of Psychiatry, 161(2):217–222. — Pooled randomized trials showing long-term lithium roughly halves relapse risk versus placebo, with its strongest effect against manic relapse. (PMID: 14754766)
- Severus E, Taylor MJ, Sauer C, et al. (2014). Lithium for Prevention of Mood Episodes in Bipolar Disorders: Systematic Review and Meta-Analysis. International Journal of Bipolar Disorders, 2:15. — Confirms lithium prevents both manic and depressive episodes and supports it as a first-line maintenance treatment. (PMID: 25530932)
- BALANCE investigators and collaborators; Geddes JR, Goodwin GM, Rendell J, et al. (2010). Lithium Plus Valproate Combination Therapy versus Monotherapy for Relapse Prevention in Bipolar I Disorder (BALANCE): A Randomised Open-Label Trial. The Lancet, 375(9712):385–395. — A randomized trial finding lithium (alone or with valproate) more effective for relapse prevention than valproate alone. (PMID: 20092882)
- Cipriani A, Hawton K, Stockton S, Geddes JR. (2013). Lithium in the Prevention of Suicide in Mood Disorders: Updated Systematic Review and Meta-Analysis. BMJ, 346:f3646. — Landmark meta-analysis of randomized trials showing lithium reduces the risk of suicide and of death from any cause in mood disorders. (PMID: 23814104)
- Memon A, Rogers I, Fitzsimmons SMDD, et al. (2020). Association between Naturally Occurring Lithium in Drinking Water and Suicide Rates: Systematic Review and Meta-Analysis of Ecological Studies. British Journal of Psychiatry, 217(6):667–678. — A rigorous meta-analysis finding higher natural lithium in drinking water associated with lower population suicide rates — an association, not proof. (PMID: 32716281)
- Vita A, De Peri L, Sacchetti E. (2015). Lithium in Drinking Water and Suicide Prevention: A Review of the Evidence. International Clinical Psychopharmacology, 30(1):1–5. — A systematic review summarizing the ecological evidence linking trace lithium in water to lower suicide rates. (PMID: 25072645)
- Schrauzer GN, Shrestha KP. (1990). Lithium in Drinking Water and the Incidences of Crimes, Suicides, and Arrests Related to Drug Addictions. Biological Trace Element Research, 25(2):105–113. — The influential early Texas-counties study that popularized the trace-lithium hypothesis. (PubMed search link — DOI unreliable.)
- McKnight RF, Adida M, Budge K, et al. (2012). Lithium Toxicity Profile: A Systematic Review and Meta-Analysis. The Lancet, 379(9817):721–728. — A comprehensive review of lithium's adverse effects, including its impact on the thyroid, kidneys, and parathyroid — the evidence base behind routine monitoring. (PMID: 22265699)
- Pacholko AG, Bekar LK. (2021). Lithium Orotate: A Superior Option for Lithium Therapy? Brain and Behavior, 11(8):e2262. — A critical review concluding that the claimed advantages of low-dose lithium orotate over carbonate are not established by adequate human evidence. (PMID: 34196483)
Live PubMed Searches
- Lithium carbonate & bipolar maintenance
- Lithium & suicide prevention
- Trace lithium in drinking water
- Lithium orotate
- Lithium toxicity & monitoring
- Lithium in pregnancy
Connections
- Bipolar Disorder
- Depression
- Anxiety
- Natural Anxiety Relief
- Magnesium
- Hypothyroidism
- Kidney Disease
- All Minerals