Rheumatoid Factor (RF) Test — Autoimmune Screening
Rheumatoid factor (RF) is an autoantibody — most commonly IgM — directed against the Fc region of IgG immunoglobulins, produced by B cells in the inflamed synovium. It is one of the oldest serological markers in rheumatology, used alongside anti-CCP antibody to support the diagnosis and monitoring of rheumatoid arthritis and other autoimmune and infectious conditions.
Table of Contents
- What Is Rheumatoid Factor
- How the Test Is Performed
- Reference Ranges and Interpretation
- Clinical Uses: Rheumatoid Arthritis
- Non-RA Causes of Positive RF
- Anti-CCP Antibody: The Preferred Companion Test
- RF in Sjögren Syndrome
- Cryoglobulinemia and HCV
- Monitoring and Clinical Interpretation Tips
- References
- Featured Videos
What Is Rheumatoid Factor
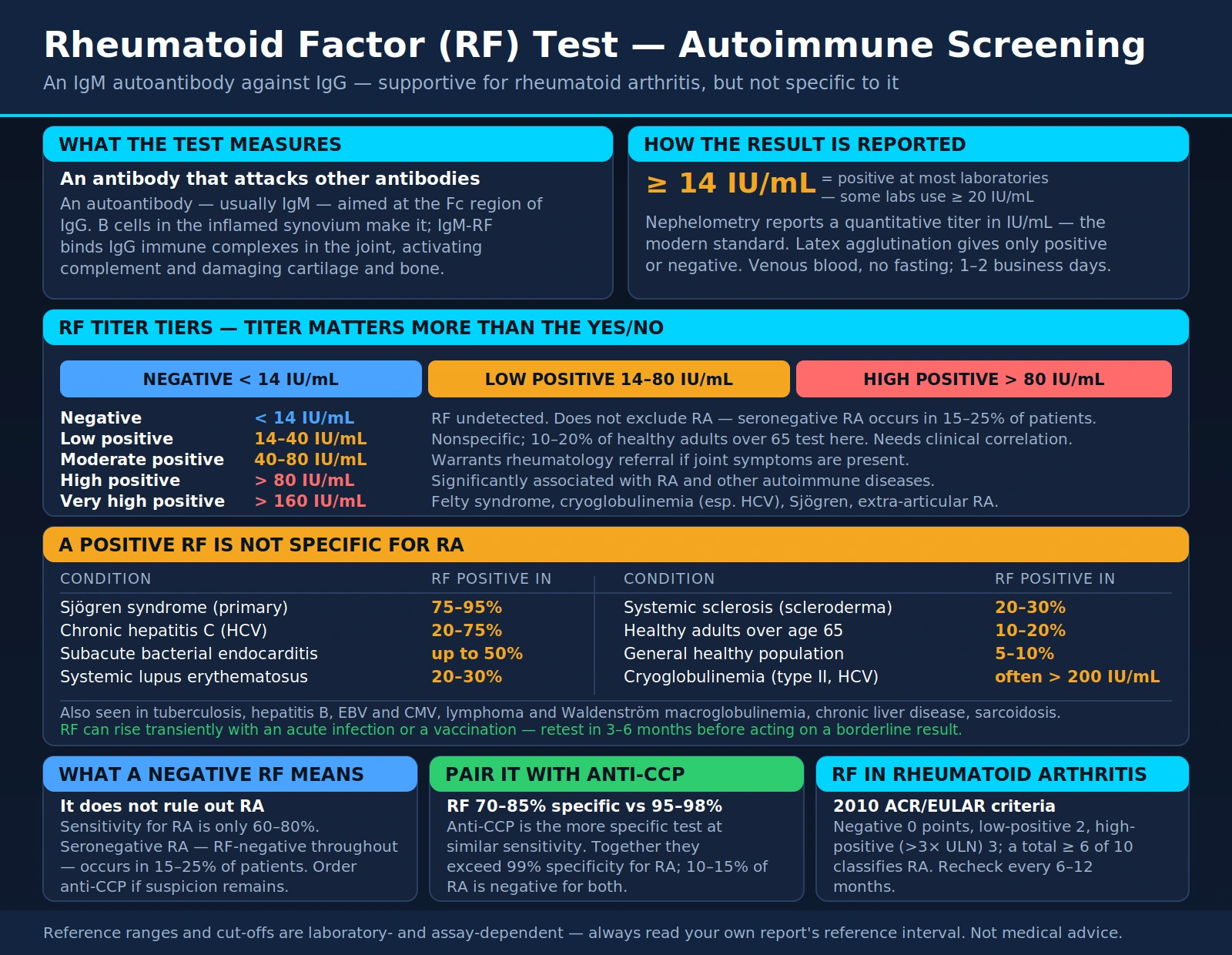
Rheumatoid factor (RF) is an autoantibody — most commonly of the IgM class — that targets the Fc region of IgG immunoglobulin molecules. In other words, it is an antibody that recognizes and binds to other antibodies. RF is produced by B cells in the synovial lining of inflamed joints, though it can also be generated in other lymphoid tissues during chronic immune activation.
The underlying mechanism involves immune complex formation: IgM-RF binds IgG-containing immune complexes in the joint, activating complement and driving the inflammatory cascade that damages cartilage and bone in rheumatoid arthritis. However, RF is not specific to RA — it appears in many conditions involving sustained B-cell activation, including chronic infections, other autoimmune diseases, and even in healthy older adults.
Detection methods vary by laboratory:
- Latex agglutination (qualitative): The older screening method; reports positive or negative; lower sensitivity and reproducibility
- Nephelometry (quantitative): The modern standard; measures light scatter through the sample; reports RF titer in IU/mL with high precision
- ELISA (enzyme-linked immunosorbent assay): Can detect IgM, IgG, and IgA RF isotypes separately; used in research and specialized labs
- Point-of-care rapid tests: Available but have lower sensitivity; acceptable for screening, not for monitoring
The normal threshold is laboratory-dependent: most laboratories define a positive RF as ≥14 IU/mL, though some use ≥20 IU/mL. Titer matters clinically — a low-positive result (14–40 IU/mL) is nonspecific and common in healthy older adults, while a high-positive result (>80 IU/mL) or very high result (>160 IU/mL) carries much greater diagnostic significance for autoimmune disease.
How the Test Is Performed
The RF test is straightforward and places minimal burden on the patient:
- Sample: Standard venous blood draw; no fasting required; results are not meaningfully affected by recent meals
- Turnaround time: 1–2 business days from most clinical laboratories; some point-of-care tests return results in minutes
- Reporting format: Quantitative labs report in IU/mL (nephelometry); qualitative labs report positive or negative; both are acceptable, but quantitative titers are preferred for monitoring
- Concurrent tests: RF is almost always ordered alongside anti-CCP IgG antibody for RA diagnosis; inflammatory markers (ESR, CRP) are typically included in the same panel; ANA may be added to screen for SLE
- Repeat testing: If clinically uncertain, repeat in 3–6 months; RF can transiently rise with acute infections or vaccinations
In the context of suspected RA, the 2010 ACR/EULAR classification criteria specify that RF and anti-CCP should be quantified (not just positive/negative) because the score assigned depends on whether the result is low-positive (2 points) or high-positive — defined as >3 times the upper limit of normal (2 points). Ordering a quantitative RF by nephelometry from the start avoids the need for repeat testing.
Anti-CCP (anti-cyclic citrullinated peptide) IgG is now considered more specific than RF for RA (95–98% specific vs. 70–85% for RF) at comparable sensitivity. Ordering both provides the optimal combination of sensitivity and specificity for RA diagnosis.
Reference Ranges and Interpretation
RF reference ranges vary between laboratories; always interpret against the specific lab's reference interval. The following tiers reflect the most widely used clinical thresholds:
RF Titer (IU/mL) Clinical interpretation tiers
- Negative (<14 IU/mL, most labs): RF undetected; does not exclude RA (seronegative RA occurs in 15–25% of patients); consider anti-CCP if clinical suspicion remains
- Low positive (14–40 IU/mL): Nonspecific; common in healthy elderly (10–20% over age 65); requires clinical correlation; low-positive alone does not support an RA diagnosis
- Moderate positive (40–80 IU/mL): More clinically significant; warrants rheumatology referral if joint symptoms are present; can occur in Sjögren syndrome, chronic infections, and RA
- High positive (>80 IU/mL): Significantly associated with RA and other autoimmune diseases; >3× ULN scores 3 points in the 2010 ACR/EULAR RA criteria
- Very high positive (>160 IU/mL): Strongly associated with Felty syndrome (RA + splenomegaly + neutropenia), high-titer seropositive RA with extra-articular features, cryoglobulinemia (especially with HCV), and Sjögren syndrome
Key diagnostic performance metrics for RF in rheumatoid arthritis:
- Sensitivity for RA: 60–80% — RF misses 20–40% of RA patients (seronegative disease)
- Specificity for RA: 70–85% — positive RF in a patient with joint symptoms raises pre-test probability, but does not confirm RA alone
- Combined RF + anti-CCP specificity: >99% — dual positivity is highly predictive of RA
Clinical Uses: Rheumatoid Arthritis
Rheumatoid arthritis is the most important clinical context in which RF is ordered. The 2010 ACR/EULAR RA classification criteria include RF as one of four scoring domains (along with joint involvement, acute-phase reactants, and symptom duration). RF scoring:
- Negative RF: 0 points
- Low-positive RF (positive but ≤3× ULN): 2 points
- High-positive RF (>3× ULN): 3 points
A total score ≥6 out of 10 is required to classify as RA; RF alone cannot diagnose RA. The full clinical picture — symptom duration, joint count and distribution, inflammatory markers, and imaging — is always required.
Clinical correlations of RF positivity in established RA:
- Disease severity: High-titer RF correlates with more aggressive joint destruction, higher erosion rates on imaging, and greater disability over time
- Extra-articular manifestations: RF-positive RA patients have higher rates of rheumatoid nodules, vasculitis, Felty syndrome, and interstitial lung disease
- Treatment monitoring: Serial RF testing every 6–12 months in established RA; declining RF with DMARD therapy (methotrexate, biologics) indicates serological response; rising RF during remission may predict flare
- Predictive value: Positive RF can precede clinical RA onset by years; individuals found to have RF incidentally should be monitored for early joint symptoms
- Seronegative RA: 15–25% of RA patients are RF-negative throughout their disease course; clinical diagnosis relies on anti-CCP (if positive) and 2010 criteria without serological support
RF should always be interpreted alongside CRP and ESR. In active RA, all three are typically elevated; persistently elevated inflammatory markers despite falling RF warrants investigation for an alternative inflammatory process.
Non-RA Causes of Positive RF
RF is one of the most nonspecific autoimmune tests in common use. A positive RF result — especially a low-positive titer — requires careful clinical correlation before attributing it to RA. Common and important non-RA causes include:
Chronic Infections
- Hepatitis C virus (HCV): 20–75% of chronic HCV patients have a positive RF; often high-titer; HCV is a major cause of unexplained high-titer RF and cryoglobulinemia — always test for HCV in this context
- Bacterial endocarditis: RF positive in up to 50% of subacute infective endocarditis; usually resolves with treatment of the infection
- Tuberculosis (TB): Chronic mycobacterial infection drives B-cell activation and RF production; should be considered in endemic populations with unexplained positive RF
- Hepatitis B, Epstein-Barr virus, cytomegalovirus: Can transiently induce RF during active infection
Other Autoimmune Diseases
- Sjögren syndrome: RF positive in 75–95% of primary Sjögren; often at high titers; may exceed RF titers seen in RA
- Systemic lupus erythematosus (SLE): RF positive in 20–30%; ANA and anti-dsDNA are the primary serological markers
- Systemic sclerosis (scleroderma): RF positive in 20–30%; anti-Scl-70 and anti-centromere antibodies are more specific
- Polymyositis / dermatomyositis: RF positive in a minority; anti-Jo-1 and myositis-specific antibodies are preferred markers
Other Conditions and Physiological Factors
- Healthy elderly: RF false-positive rate rises significantly with age — approximately 10–20% of adults over age 65 have a low-positive RF without any autoimmune disease; age alone is a major driver of low-titer positivity
- Cryoglobulinemia: Often very high RF titers; type II mixed cryoglobulinemia is essentially characterized by a monoclonal IgM-RF (see dedicated section below)
- Lymphoma and leukemia: Monoclonal B-cell proliferations can produce RF; Waldenström macroglobulinemia may show very high-titer IgM RF
- Pulmonary fibrosis, sarcoidosis: Low-positive RF seen in a minority; usually incidental finding
- Chronic liver disease: Polyclonal hypergammaglobulinemia in cirrhosis can produce low-positive RF
- Normal healthy adults: Approximately 5–10% of the general population has a low-positive RF without any identifiable disease
Anti-CCP Antibody: The Preferred Companion Test
Anti-cyclic citrullinated peptide (anti-CCP) IgG antibody has become the most important serological companion to RF in the evaluation of suspected RA. It targets citrullinated proteins — proteins in which arginine residues have been converted to citrulline by peptidylarginine deiminase (PAD) enzymes, a process that occurs in inflamed synovium during RA.
Key characteristics of anti-CCP in RA:
- Specificity for RA: 95–98% — significantly higher than RF (70–85%); a positive anti-CCP result is highly specific for RA
- Sensitivity for RA: 60–70% — similar to RF; neither test alone is sufficient to detect all RA cases
- Preclinical positivity: Anti-CCP can be detectable in blood years before clinical joint symptoms begin; studies show positive anti-CCP up to 10 years before RA onset in some patients
- Dual positivity (RF + anti-CCP): Specificity for RA exceeds 99%; this combination provides the strongest serological support for RA diagnosis
- Seronegative RA: Approximately 10–15% of RA patients are negative for both RF and anti-CCP; these patients require clinical diagnosis based on the full 2010 ACR/EULAR criteria without serological support
Why anti-CCP is more specific than RF: RF targets the Fc region of IgG, which can be activated by many chronic inflammatory processes; anti-CCP targets citrullinated proteins that accumulate specifically in the RA synovial environment via PAD enzyme activity. The citrullination process in the RA joint is driven by local hypoxia and neutrophil extracellular trap (NET) formation — mechanisms more specific to RA pathogenesis than the general B-cell activation that drives RF.
Current recommendation: order both RF (quantitative, nephelometry) and anti-CCP IgG together when evaluating for RA. The combination provides optimal sensitivity and specificity and is cost-effective compared to sequential testing.
RF in Sjögren Syndrome
Sjögren syndrome is the second most common systemic autoimmune disease after RA, affecting approximately 1–4 million Americans. Primary Sjögren syndrome is characterized by lymphocytic infiltration of exocrine glands, producing the hallmark symptoms of dry eyes (keratoconjunctivitis sicca) and dry mouth (xerostomia).
RF in Sjögren syndrome:
- RF is positive in 75–95% of primary Sjögren syndrome — a prevalence higher than in RA itself
- RF titers in Sjögren can be very high, sometimes exceeding those seen in RA
- The serological hallmarks more specific to Sjögren are anti-SSA/Ro (present in 70–90%) and anti-SSB/La (present in 40–60%); RF alone cannot distinguish Sjögren from RA
- Sjögren associated with secondary features of RA can present with both anti-CCP and RF; joint involvement in Sjögren is typically non-erosive, distinguishing it from RA
The most clinically important reason to recognize high-titer RF in Sjögren is lymphoma risk:
- Primary Sjögren syndrome carries a 5- to 44-fold increased risk of non-Hodgkin lymphoma (predominantly mucosa-associated lymphoid tissue [MALT] lymphoma)
- RF-positive Sjögren patients have even higher lymphoma risk than RF-negative Sjögren patients
- Additional high-risk features include persistent parotid gland enlargement, palpable purpura, peripheral neuropathy, low complement (C3/C4), and cryoglobulinemia
- Sjögren patients with high-titer RF and any of these features should undergo lymphoma screening with CT imaging or PET scan
When a patient presents with dry eyes, dry mouth, and high-titer RF, primary Sjögren should be considered alongside RA. The differential is guided by anti-CCP (positive in RA, typically negative in Sjögren), anti-SSA/SSB (specific to Sjögren), and minor salivary gland biopsy (gold standard for Sjögren diagnosis).
Cryoglobulinemia and HCV
Cryoglobulins are immunoglobulins that precipitate in the cold and dissolve upon rewarming. Type II mixed cryoglobulinemia — the most clinically significant form — is characterized by a monoclonal IgM with rheumatoid factor activity that forms immune complexes with polyclonal IgG. This is, in essence, cryoglobulinemia driven by a clonal RF.
The HCV Connection
- Chronic hepatitis C virus (HCV) infection is the cause of mixed cryoglobulinemia in the vast majority of cases (80–90%)
- 30–50% of patients with chronic HCV have laboratory-detectable cryoglobulins, though only a minority develop symptomatic cryoglobulinemic vasculitis
- The HCV virus chronically stimulates B cells in the liver and lymphoid organs, driving the monoclonal IgM-RF production that defines type II cryoglobulinemia
- RF is almost universally positive in HCV-associated cryoglobulinemia, and titers are often very high (>200 IU/mL)
Clinical Presentation of Cryoglobulinemic Vasculitis
- Palpable purpura: The most common cutaneous manifestation; non-blanching lesions on the legs and lower extremities from small-vessel vasculitis
- Arthralgia: Joint pain without erosive arthritis; affects knees, ankles, wrists
- Peripheral neuropathy: Sensory and/or motor neuropathy from vasa nervorum vasculitis; painful distal symmetric pattern
- Membranoproliferative glomerulonephritis (MPGN): Immune complex deposition in glomeruli; presents with proteinuria, hematuria, and declining renal function; can progress to renal failure
Diagnosis and Treatment
- Cryoglobulin testing: Requires special collection at 37°C (body temperature) — the sample must be kept warm from venipuncture to laboratory processing; cold exposure causes premature precipitation, producing falsely negative results
- RF in cryoglobulinemia: Very high titer RF (>160–200 IU/mL) with unexplained vasculitis symptoms should always trigger HCV testing and cryoglobulin measurement
- HCV treatment: Direct-acting antiviral (DAA) therapy achieves >95% sustained virologic response and clears cryoglobulinemia in 80–90% of cases, including resolution of vasculitis, purpura, and neuropathy in most patients
- Immunosuppression: Rituximab (anti-CD20) is used for severe cryoglobulinemic vasculitis with renal involvement or neuropathy, alongside antiviral therapy
Monitoring and Clinical Interpretation Tips
Practical guidance for interpreting RF results in clinical practice:
When the Result Is Low-Positive (14–40 IU/mL)
- In an asymptomatic patient: this is common in older adults (10–20% prevalence over age 65) and is often nonspecific; watch and wait with clinical monitoring; no immediate rheumatology referral required unless symptoms develop
- In a patient with joint symptoms: pursue full serological workup including anti-CCP, ANA, ESR, and CRP; refer to rheumatology if two or more criteria suggest early RA
- After an acute infection: RF can rise transiently with viral or bacterial infections; retest in 3–6 months if the clinical picture is otherwise unclear
When the Result Is High-Positive (>80 IU/mL)
- Always warrants clinical investigation; do not dismiss high-titer RF as nonspecific
- Test HCV if the patient has risk factors (intravenous drug use, blood transfusion before 1992, unexplained liver enzyme elevation, tattoos, sexual exposure)
- Evaluate for Sjögren syndrome (dry eyes, dry mouth, anti-SSA/SSB antibodies, minor salivary gland biopsy)
- Refer to rheumatology if joint symptoms, fatigue, or other systemic features accompany high-titer RF
Monitoring in Established RA
- Serial RF measurement every 6–12 months alongside ESR and CRP; declining RF with DMARD therapy indicates serological response
- Rising RF during clinical remission may predict flare — consider intensifying monitoring frequency
- Very high RF at diagnosis correlates with worse radiographic outcomes — consider this when selecting DMARD intensity
- Never use RF in isolation — always interpret alongside clinical disease activity score (DAS28), joint counts, and imaging
General Pitfalls to Avoid
- Do not diagnose RA based on RF alone — the 2010 ACR/EULAR criteria require a total score ≥6 from multiple domains
- Do not exclude RA based on negative RF alone — seronegative RA is clinically common (15–25% of RA patients)
- Always order anti-CCP alongside RF for RA evaluation — dual negativity supports a non-RA diagnosis; dual positivity is highly specific for RA
- Vaccinations can transiently elevate RF — if drawn within 1–2 weeks of vaccination, retest before making clinical decisions
- When cryoglobulinemia is suspected, the sample must be collected and transported at 37°C — cold transport produces false-negative results
References
- Aletaha D et al. 2010 Rheumatoid arthritis classification criteria. Arthritis Rheum. 2010;62(9):2569–2581. PMID 20872595
- Ingegnoli F et al. Rheumatoid factors: clinical applications. Dis Markers. 2013;35(6):727–734. — Search PubMed
- Aho K et al. Predictive significance of rheumatoid factor. Arthritis Rheum. 2000;43:2427–2429. — Search PubMed
- Scott DL et al. Rheumatoid arthritis. Lancet. 2010;376(9746):1094–1108. PMID 20870100
- van Venrooij WJ, Zendman AJ. Anti-CCP2 antibodies: an overview and perspective of the diagnostic abilities of this serological marker for early rheumatoid arthritis. Clin Rev Allergy Immunol. 2008;34(1):36–39. PMID 18270851
- Ramos-Casals M et al. Primary Sjögren syndrome. N Engl J Med. 2018;378(10):931–939. — Search PubMed
- Cacoub P et al. Mixed cryoglobulinemia and hepatitis C. J Hepatol. 2002;36(6):735–746. — Search PubMed
- Ferri C et al. Hepatitis C virus and mixed cryoglobulinemia. Eur J Clin Invest. 2004;34(suppl 2):26–32. — Search PubMed
- Pruijn GJ et al. Citrullination: a small change for a protein with large consequences for rheumatoid arthritis. Nat Rev Rheumatol. 2009;5:263–264. — Search PubMed
- Jonsson R et al. Sjögren's syndrome. Lancet. 2002;360(9339):1110–1118. — Search PubMed
- McInnes IB, Schett G. The pathogenesis of rheumatoid arthritis. N Engl J Med. 2011;365(23):2205–2219. PMID 22150039
- Nishimura K et al. Meta-analysis: diagnostic accuracy of anti-cyclic citrullinated peptide antibody and rheumatoid factor for rheumatoid arthritis. Ann Intern Med. 2007;146(11):797–808. PMID 17548411
Connections
- All Lab Tests
- ANA Test
- ANCA Test
- ESR Test
- hs-CRP
- Inflammatory Markers
- Rheumatoid Arthritis
- Sjögren Syndrome
- Systemic Lupus Erythematosus
- Cryoglobulinemia — type II mixed cryoglobulinemia is driven by a monoclonal IgM rheumatoid factor, and RF titers are often very high.