Hepatitis Panel — Hepatitis B and C Screening and Diagnosis
The hepatitis panel is a group of blood tests that detect infection with the hepatitis B virus (HBV) and hepatitis C virus (HCV) — two leading causes of chronic liver disease worldwide that together affect more than 300 million people and are responsible for the majority of cirrhosis and hepatocellular carcinoma cases globally. Because both infections progress silently for years before causing symptoms, serological screening is the only reliable way to identify infected individuals early, when treatment is most effective and transmission can be prevented.
Table of Contents
- What the Hepatitis Panel Tests
- Hepatitis B Surface Antigen (HBsAg)
- Anti-HBs: Immunity Marker
- Hepatitis B Core Antibody (Anti-HBc)
- Hepatitis B e Antigen and Viral Load
- Anti-HCV and RNA Confirmation
- HCV Genotype and Treatment Implications
- Interpreting the Hepatitis B Serological Pattern
- When to Order and Who Should Be Screened
- References
- Connections
- Featured Videos
What the Hepatitis Panel Tests
The hepatitis panel screens for viral hepatitis infections that cause liver inflammation and can progress silently to cirrhosis and liver cancer. WHO estimates 254 million people live with chronic HBV and 50 million with chronic HCV globally. Both are leading causes of cirrhosis and hepatocellular carcinoma.
The Hepatitis B panel includes multiple serological markers that together reveal infection status, immune response, and viral activity:
- HBsAg (surface antigen) — active HBV infection
- Anti-HBs (surface antibody) — immunity from vaccination or past infection
- Anti-HBc IgM (core antibody IgM) — acute HBV infection
- Anti-HBc IgG (core antibody IgG) — past or chronic HBV exposure
- HBeAg (e antigen) — active viral replication with high infectivity
- Anti-HBe — marker of reduced replication after HBeAg seroconversion
- HBV DNA (viral load by PCR) — gold standard quantification of replication
The Hepatitis C panel focuses on exposure detection and active infection confirmation:
- Anti-HCV (antibody) — exposure to HCV, whether cleared or active
- HCV RNA by PCR — confirms active infection when anti-HCV is reactive
- HCV genotype (1–6) — guides treatment selection and duration
No fasting is required for hepatitis panel blood tests. Results are not affected by recent meals.
Hepatitis B Surface Antigen (HBsAg)
HBsAg is the first marker to appear after HBV infection, typically within 1–10 weeks of exposure. Its detection indicates active HBV infection — either acute or chronic.
- Presence of HBsAg for more than 6 months defines chronic HBV infection
- Positive in both acute and chronic hepatitis B
- May transiently disappear during the "window period" — the interval between HBsAg clearance and anti-HBs appearance — which is why total anti-HBc is included in comprehensive screening panels
- Qualitative assays report reactive/non-reactive; quantitative assays measure in IU/mL
- Quantitative HBsAg levels guide treatment: HBsAg < 1,000 IU/mL at 24 weeks of peginterferon treatment predicts good response
- FDA threshold for HBsAg positivity: ≥ 0.05 IU/mL
- Reactive results are confirmed by neutralization assay
- HBsAg clearance (seroconversion to anti-HBs positive) is considered functional cure of chronic HBV — occurs spontaneously in fewer than 1% of chronic patients per year
A positive HBsAg alone does not reveal how active the infection is or whether there is liver damage. Additional markers — particularly HBV DNA, HBeAg, and liver enzymes (ALT/AST) — are required for staging and treatment planning.
Anti-HBs: Immunity Marker
Anti-HBs (antibody to hepatitis B surface antigen) is the immunity marker for HBV. It appears after natural infection and clearance, or after vaccination, and signals protection against future HBV infection.
- Protective level: anti-HBs ≥ 10 mIU/mL
- Isolated anti-HBs positive (without anti-HBc) = vaccine-induced immunity
- Anti-HBs positive with anti-HBc positive = past natural infection with recovery
- Healthcare workers, dialysis patients, and immunocompromised individuals should be tested 1–2 months post-vaccination to confirm seroconversion
- Non-responders (anti-HBs < 10 mIU/mL after a full 3-dose series) should receive a second vaccine series; after two complete series without response, the person is considered a true non-responder
- Anti-HBs titers can wane over decades in healthy adults — booster dosing is controversial and generally not recommended in immunocompetent individuals with a documented initial response
- Immunocompromised patients (transplant recipients, HIV-positive individuals, patients on chemotherapy) may benefit from periodic monitoring and booster dosing when anti-HBs falls below 10 mIU/mL
The combination of anti-HBs and anti-HBc interpretation is critical: they distinguish vaccine immunity from past natural infection, which has different clinical implications (natural infection may leave residual occult HBV DNA in liver tissue even after surface antigen clearance).
Hepatitis B Core Antibody (Anti-HBc)
The hepatitis B core antibody exists in two forms — IgM and IgG — and each provides different clinical information. Unlike HBsAg and anti-HBs, anti-HBc (especially the IgG form) is not induced by vaccination; it is only produced in response to actual HBV infection.
Anti-HBc IgM
- Appears during early acute HBV infection
- Distinguishes acute from chronic HBV — IgM is a marker of recent infection
- Detectable during the window period when HBsAg may have already cleared
- IgM titers typically fall within 6 months of infection onset
Anti-HBc IgG (Total Anti-HBc)
- Persists lifelong after any HBV exposure — it does not distinguish active from resolved infection
- Used in blood bank screening to exclude HBV-exposed donors
Isolated Anti-HBc (Positive anti-HBc, Negative HBsAg, Negative anti-HBs)
This pattern has three possible meanings:
- Resolved past infection with undetectable anti-HBs — the most common explanation; anti-HBs has waned below detectable levels over time
- Occult HBV — HBsAg-negative but HBV DNA is present in liver tissue; clinically significant in immunosuppressed patients starting chemotherapy or biologic therapy, where reactivation can be life-threatening
- False positive anti-HBc — particularly in low-prevalence populations
Immunocompromised patients with isolated anti-HBc should have HBV DNA measured before starting immunosuppression. If HBV DNA is detectable, antiviral prophylaxis (entecavir or tenofovir) is recommended to prevent reactivation.
Hepatitis B e Antigen and Viral Load
HBeAg and HBV DNA quantification provide direct information about how actively the virus is replicating — the two key drivers of liver damage and infectivity in chronic HBV.
HBeAg
- HBeAg is a secreted protein that serves as a marker of active viral replication
- Present in early acute infection and in some patients with chronic HBV
- HBeAg-positive chronic HBV = high replication, high infectivity, higher risk of liver damage
- HBeAg seroconversion (HBeAg disappears, anti-HBe appears) = reduced replication, lower infectivity, often associated with improved prognosis
- HBeAg-negative chronic HBV is common and caused by precore or core promoter mutations that prevent HBeAg production while viral replication continues; these patients can have normal ALT despite active disease — ALT alone is not sufficient to assess activity
HBV DNA (Viral Load)
- Gold standard for measuring HBV replication
- Detectable at 10–20 IU/mL by PCR
- Treatment threshold: HBV DNA > 2,000 IU/mL with elevated ALT, or > 20,000 IU/mL regardless of ALT, warrants antiviral therapy
- First-line treatments: entecavir or tenofovir disoproxil fumarate (TDF) / tenofovir alafenamide (TAF) — all achieve durable viral suppression in the majority of patients
- HBV DNA is monitored every 3–6 months during treatment; sustained undetectable HBV DNA is the goal of antiviral therapy
- Unlike HCV, HBV is not curable with current antivirals — treatment suppresses but does not eliminate the virus (covalently closed circular DNA, cccDNA, persists in hepatocyte nuclei)
Anti-HCV and RNA Confirmation
Hepatitis C testing follows a two-step algorithm: antibody screening followed by RNA confirmation. This two-step approach is essential because a positive antibody alone cannot distinguish active infection from past cleared infection.
Anti-HCV (HCV Antibody)
- First-line screening test for HCV exposure
- Detectable 4–10 weeks after infection; some assays detect antibody as early as 3 weeks
- Persists lifelong whether the infection is cleared or ongoing — a positive anti-HCV in a patient who received treatment years ago may simply reflect past exposure
- FDA-cleared anti-HCV assays have sensitivity exceeding 99%
- False positives can occur in autoimmune disease, some malignancies, and other conditions that cause non-specific immunoglobulin elevation
- The USPSTF recommends universal HCV screening for all adults aged 18–79 (2020 recommendation, Grade B)
- Baby boomers (born 1945–1965) have the highest HCV prevalence in the US at 3.25% — birth cohort testing in this group has identified the majority of undiagnosed cases
HCV RNA by PCR
- All reactive anti-HCV results require reflex confirmation with HCV RNA by PCR
- HCV RNA positive = active viral replication = current infection requiring treatment evaluation
- HCV RNA negative with positive anti-HCV = past infection that was cleared (either spontaneously or after treatment)
- HCV RNA can be detected within 1–2 weeks of infection, before antibodies appear — useful in the acute window period and in immunocompromised patients who may not mount an antibody response
HCV Genotype and Treatment Implications
HCV exists in six major genotypes (1–6) with distinct geographic distributions. Genotyping guides treatment selection and duration, though modern pan-genotypic therapies have simplified decision-making substantially.
- Genotype 1 (subtypes 1a and 1b): most common in the US, accounting for approximately 70% of infections; excellent response to modern direct-acting antiviral (DAA) therapy
- Genotypes 2 and 3: together account for most remaining US cases; highly treatable; genotype 3 is associated with faster fibrosis progression and a persistently elevated risk of hepatocellular carcinoma even after viral clearance
- Genotype 4: most common in Africa and the Middle East; less common in the US but fully treatable with pan-genotypic regimens
- Genotypes 5 and 6: uncommon in the US; both respond to pan-genotypic treatment
Modern DAA Treatment
- Glecaprevir/pibrentasvir (Mavyret): 8 weeks for treatment-naive, non-cirrhotic patients across all genotypes; 12 weeks for cirrhosis; achieves sustained virological response at 12 weeks post-treatment (SVR12) in 95–99% of patients
- Sofosbuvir/velpatasvir (Epclusa): 12 weeks pan-genotypic; similarly high SVR12 rates; preferred in decompensated cirrhosis (with low-dose ribavirin)
- SVR12 is considered a cure — HCV RNA remains undetectable indefinitely in more than 99% of patients who achieve it
- Genotyping remains clinically useful to identify prior NS5A-inhibitor resistance-associated substitutions in patients who have failed prior DAA therapy
Unlike HBV, HCV does not integrate into the host genome and can be completely eliminated. With curative therapy available, the primary goal of screening is to identify infection before liver fibrosis and cirrhosis develop.
Interpreting the Hepatitis B Serological Pattern
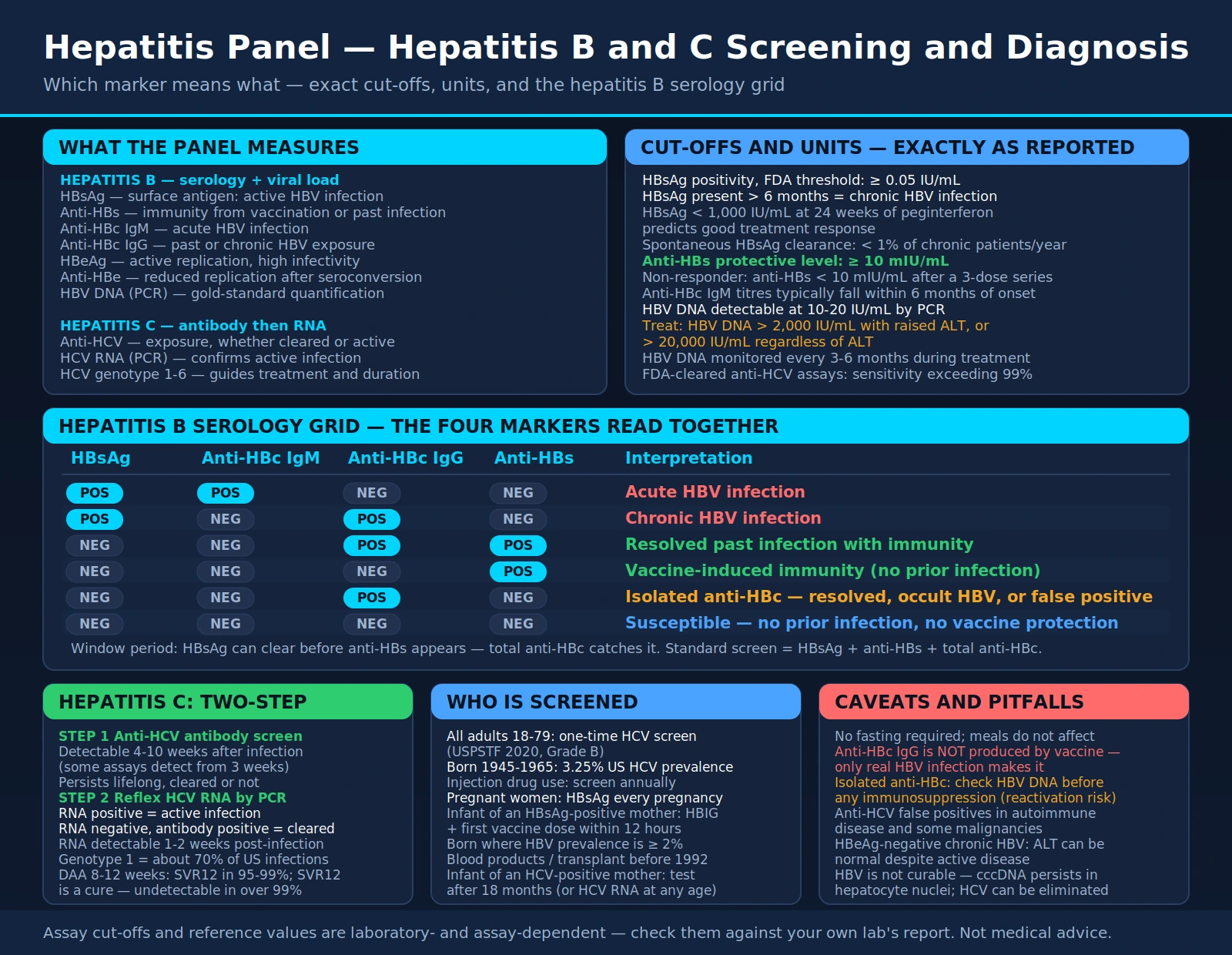
The combination of HBsAg, anti-HBc, and anti-HBs results determines HBV status. The following table summarizes the major clinical patterns:
| HBsAg | Anti-HBc IgM | Anti-HBc IgG | Anti-HBs | Interpretation |
|---|---|---|---|---|
| Positive | Positive | Negative | Negative | Acute HBV infection |
| Positive | Negative | Positive | Negative | Chronic HBV infection |
| Negative | Negative | Positive | Positive | Resolved past infection with immunity |
| Negative | Negative | Negative | Positive | Vaccine-induced immunity (no prior infection) |
| Negative | Negative | Positive | Negative | Isolated anti-HBc — see section 4 for interpretation |
| Negative | Negative | Negative | Negative | Susceptible — no prior infection, no vaccine protection |
The standard 3-marker screening panel for most clinical purposes is HBsAg + anti-HBs + total anti-HBc. This combination covers active infection (HBsAg), immunity status (anti-HBs), and past exposure (anti-HBc). In settings where acute HBV is suspected, anti-HBc IgM should be added specifically.
Pregnant women require HBsAg screening every pregnancy regardless of prior results or vaccination history — neonates born to HBsAg-positive mothers receive hepatitis B immune globulin (HBIG) and the first vaccine dose within 12 hours of birth.
When to Order and Who Should Be Screened
Hepatitis B and C screening targets both universal populations (based on age and risk period) and high-risk groups where prevalence is substantially elevated.
Hepatitis B Screening Indications
- All pregnant women — every pregnancy, at the first prenatal visit
- People born in countries with HBV prevalence ≥ 2% — includes most of Asia, sub-Saharan Africa, Eastern Europe, and the Middle East
- US-born individuals from households with HBV endemic-country origin
- HIV-positive individuals — HBV/HIV co-infection is common and both infections influence each other's treatment
- Injection drug users
- Dialysis patients and those with chronic kidney disease
- Sex partners or household contacts of HBsAg-positive individuals
- Men who have sex with men
- Incarcerated individuals
- Patients initiating immunosuppressive therapy or chemotherapy — occult HBV reactivation can cause fulminant hepatitis
Hepatitis C Screening Indications
- All adults aged 18–79 (USPSTF 2020 recommendation, Grade B) — one-time screening if no ongoing risk
- All adults with ongoing injection drug use — screen annually
- HIV-positive individuals
- Healthcare workers and first responders following needlestick or mucosal exposure
- People born 1945–1965 (baby boomers) — highest US prevalence cohort
- Recipients of blood products or organ transplants before 1992
- People who received tattoos or piercings in non-sterile settings
- People who have been incarcerated
- Patients on hemodialysis
- Children born to HCV-positive mothers — test after 18 months of age (anti-HCV after 18 months, or HCV RNA at any age)
Follow-Up After Positive Results
- All reactive HBsAg or anti-HCV results require confirmatory testing
- Referral to hepatology or infectious disease for comprehensive evaluation, fibrosis staging, and treatment planning
- Liver enzymes (ALT/AST), complete blood count, and hepatic imaging (ultrasound) are typically ordered as part of the initial workup
- In chronic HBV: liver biopsy or non-invasive fibrosis assessment (FibroScan, FIB-4 score) guides treatment initiation decisions
- In active HCV: pan-genotypic DAA therapy achieves cure in 8–12 weeks for most patients — treatment should not be delayed
References
- Terrault NA et al. AASLD guidelines for treatment of chronic hepatitis B. Hepatology. 2018;67(4):1560-1599. PMID 29405329
- Ghany MG et al. Hepatitis C guidance 2019 update: AASLD-IDSA. Hepatology. 2019;71(2):686-721. — Search PubMed
- World Health Organization. Global hepatitis report, 2017. ISBN 9789241565455. WHO.int
- Loomba R, Liang TJ. Hepatitis B Reactivation Associated with Immune Suppressive and Biological Modifier Therapies. Gastroenterology. 2017;152(6):1297-1309. PMID 28219691
- Moyer VA; USPSTF. Screening for hepatitis C virus infection in adults. Ann Intern Med. 2013;159(5):349-57. PMID 23798026
- Kowdley KV et al. Ledipasvir and sofosbuvir for 8 or 12 weeks for chronic HCV without cirrhosis. N Engl J Med. 2014;370(20):1879-88. PMID 24720702
- Zeuzem S et al. Glecaprevir-pibrentasvir for 8 or 12 weeks in HCV genotype 1 or 3 infection. N Engl J Med. 2018;378(4):354-369. — Search PubMed
- Alter MJ et al. The prevalence of hepatitis C virus infection in the United States. N Engl J Med. 1999;341(8):556-62. PMID 10451460
- Tsai NC et al. HBeAg seroconversion and treatment outcomes. J Gastroenterol. 2013;48(4):527-37. — Search PubMed
- Cohen C et al. Why haven't birth cohort testing recommendations for hepatitis C been implemented? Am J Med. 2011;124(8):784-92. — Search PubMed
- Burstow NJ et al. Hepatitis C treatment. BMJ. 2017;356:j834. — Search PubMed
- Liu CJ et al. HBsAg quantification predicts spontaneous HBsAg seroclearance. Hepatology. 2011;53(1):135-44. — Search PubMed
Connections
- All Lab Tests
- Liver Function Tests
- Albumin
- LDH
- ANA Test
- Inflammatory Markers
- Hepatitis B
- Hepatitis C
- Cirrhosis
- Hepatitis — the umbrella liver-inflammation condition this panel screens for, covering all viral types and their transmission routes.