Heavy Metals Panel
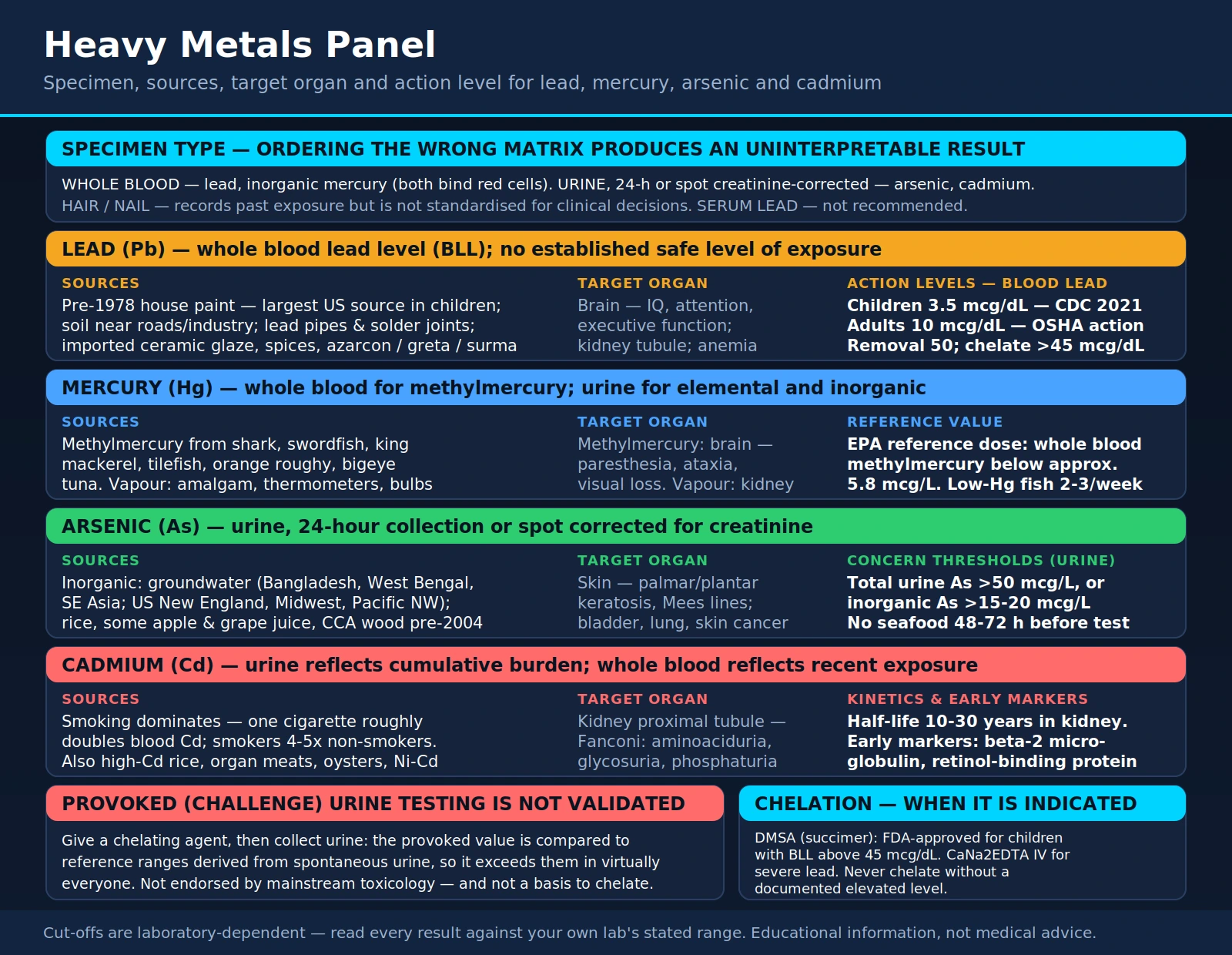
Table of Contents
- Specimen Type: Why It Matters
- Lead: Blood Lead Level (BLL)
- Mercury: Methylmercury vs. Inorganic
- Arsenic: Organic vs. Inorganic
- Cadmium: The Smoking Metal
- Other Metals in Common Panels
- Chelation Therapy: Evidence and Thresholds
- Who Should Be Tested
- Research Papers
- Connections
- Featured Videos
Specimen Type: Why It Matters
Heavy metals testing is not a single test — it is a collection of measurements that each require a specific specimen type to be clinically meaningful. Ordering the wrong matrix produces results that are uninterpretable or actively misleading.
Whole blood is the preferred specimen for lead and inorganic mercury. These metals bind tightly to red blood cells and hemoglobin, so whole blood reflects ongoing or recent exposure with far greater accuracy than serum or plasma. Serum lead levels, in particular, are not recommended for clinical assessment because they capture only the free fraction, which is a small and inconsistently measured portion of total body lead.
Urine (typically 24-hour collection, or a spot urine corrected for creatinine) is preferred for arsenic and cadmium. Both of these metals are excreted predominantly through the kidneys and concentrate in urine, making urine the most representative sample of body burden and recent exposure.
Hair and nail analysis can detect past exposure over weeks to months because metals are incorporated into growing keratin. However, these matrices are not standardized for clinical decisions due to variable external contamination, differences in washing protocols between laboratories, and a lack of consensus reference ranges. Hair and nail testing is appropriate for forensic or research purposes, not routine clinical management.
Challenge or provocation testing — administering a chelating agent and then collecting urine to measure excreted metals — is used by some integrative medicine practitioners but is not endorsed by mainstream toxicology or occupational medicine guidelines. The provoked values are not comparable to standard reference ranges, which are derived from spontaneous (unprovoked) specimens, making challenge results difficult to interpret clinically.
Lead: Blood Lead Level (BLL)
Lead is measured as blood lead level (BLL) using whole blood. There is no established safe level of lead exposure, and the action thresholds have been revised downward repeatedly as evidence of harm at lower concentrations has accumulated.
- Children — CDC 2021 blood lead reference value: 3.5 mcg/dL. This was lowered from 5 mcg/dL based on new epidemiological data demonstrating cognitive and behavioral effects at even lower concentrations. Children identified at or above this level should receive case management, environmental investigation, and follow-up testing.
- Adults — OSHA occupational action level: 10 mcg/dL (with mandatory medical surveillance), and removal from lead exposure at 50 mcg/dL. OSHA is currently updating these standards.
- Pregnant women and women of childbearing age should be managed at the same thresholds as children due to placental transfer and fetal neurotoxicity.
Common sources of lead exposure include paint in pre-1978 homes (the single largest source for US children), contaminated soil near roads or former industrial sites, older plumbing with lead pipes or lead-solder joints, imported ceramics and pottery with lead-containing glazes, some imported spices (turmeric, paprika, chili powder have been found adulterated with lead chromate for color enhancement), imported vinyl mini-blinds, and traditional home remedies from some cultures (azarcon, greta, surma).
Symptoms of lead poisoning depend on exposure level and duration. In children, even subclinical blood lead levels impair IQ, executive function, attention, and behavior — effects that may be permanent. In adults: fatigue, hypertension, renal tubular damage, peripheral neuropathy (wrist or foot drop), abdominal colic, and anemia (lead inhibits heme synthesis at two steps: ALA dehydratase and ferrochelatase, producing a microcytic hypochromic anemia with elevated free erythrocyte protoporphyrin).
Iron deficiency dramatically amplifies lead absorption — the intestinal iron transporter DMT1 also transports lead, and upregulation from iron deficiency pulls in more lead. Treating concurrent iron deficiency is an essential part of lead management. Calcium and zinc also compete with lead for absorption.
Chelation therapy is indicated for symptomatic lead poisoning or BLL above 45 mcg/dL in children (FDA-approved: DMSA/succimer oral). Severe encephalopathy requires IV EDTA (CaEDTA) with or without BAL. The primary intervention for all lead levels remains environmental remediation — identifying and eliminating the source of exposure.
Mercury: Methylmercury vs. Inorganic/Elemental
Mercury exists in three forms, each with distinct sources, toxicology, and clinical management:
Methylmercury (Organic Mercury)
Methylmercury is the form that accumulates in fish and other marine organisms. It is formed when inorganic mercury in ocean sediment is methylated by bacteria and then biomagnifies up the food chain, reaching the highest concentrations in large, long-lived predatory fish: shark, swordfish, king mackerel, tilefish (Gulf of Mexico), orange roughy, and bigeye tuna. Canned light tuna (primarily skipjack) has substantially lower levels than canned albacore tuna.
Methylmercury is almost completely absorbed from the gastrointestinal tract, distributes throughout the body, crosses the blood-brain barrier and placenta, and is primarily neurotoxic. The classic large-scale outbreak was Minamata disease in Japan (1950s–1960s), caused by industrial methylmercury discharge into Minamata Bay. Symptoms of methylmercury poisoning: sensory disturbances (paresthesias), ataxia, visual field constriction, hearing loss, tremor, and in severe cases death.
Whole blood is the preferred specimen for methylmercury because it distributes into red blood cells. The EPA reference dose corresponds to a whole blood methylmercury level below approximately 5.8 mcg/L. The FDA and EPA advise pregnant women, nursing mothers, and young children to limit high-mercury fish while continuing to eat 2–3 servings per week of lower-mercury fish (salmon, sardines, shrimp, catfish, canned light tuna).
Elemental Mercury
Elemental (metallic) mercury vapor is released from dental amalgam fillings, broken thermometers, broken fluorescent bulbs, and industrial settings. Mercury vapor is well absorbed through the lungs and is primarily nephrotoxic and, at high doses, neurotoxic. Urine mercury is the appropriate specimen for elemental mercury exposure. The debate over dental amalgam and health effects is not settled; mainstream dental and health organizations consider amalgam fillings safe for most people, though some individuals may have idiosyncratic sensitivity.
Inorganic Mercury Salts
Inorganic mercury compounds are used in some industrial processes and have historically appeared in certain skin-lightening creams (still found in products from some countries). They are primarily nephrotoxic. Urine mercury is the appropriate specimen.
Treatment of mercury toxicity: DMSA (succimer) is used for methylmercury. BAL (dimercaprol) is historically used but has significant toxicity of its own. Supportive care and removal from exposure are primary. Avoidance of high-mercury fish is the main preventive strategy for the general population.
Arsenic: Organic vs. Inorganic
Arsenic testing almost always requires urine (24-hour collection or spot urine corrected for creatinine). The most critical distinction in arsenic testing is between organic and inorganic arsenic — a distinction that is frequently overlooked and leads to false positive interpretations.
Organic arsenic — primarily arsenobetaine — is abundant in seafood (fish, shrimp, shellfish) and is essentially nontoxic. It is absorbed and excreted unchanged in urine without any conversion to toxic forms. A patient who consumed shrimp, crab, or fish the day before a urine arsenic test will commonly show dramatically elevated total urine arsenic, sometimes ten times the reference range, entirely from benign arsenobetaine. Patients must avoid all seafood for at least 48–72 hours before urine arsenic collection. Without this instruction, false positive results are extremely common and lead to unnecessary anxiety and further testing.
Inorganic arsenic is a Group 1 carcinogen (International Agency for Research on Cancer). Sources: contaminated groundwater (particularly in Bangladesh, West Bengal, parts of Southeast Asia, and US regions including New England, the Midwest, and Pacific Northwest), rice and rice-based products (rice absorbs arsenic from paddy water), some apple and grape juice, and wood pressure-treated with chromated copper arsenate (CCA, used prior to 2004 for residential lumber).
Chronic low-dose inorganic arsenic exposure produces a characteristic syndrome: palmar and plantar keratosis (thickened skin on palms and soles), Mees lines (white transverse bands across fingernails), rain-drop hyperpigmentation alternating with depigmentation of the skin, peripheral neuropathy, and significantly increased risk of bladder, lung, and skin cancers. Blackfoot disease (peripheral vascular disease causing gangrene of the extremities) occurred in Taiwan from severe groundwater arsenic contamination.
Some commercial laboratories can fractionate urine arsenic to separately report inorganic arsenic, methylarsenic species, and arsenobetaine. Total urine arsenic above 50 mcg/L, or inorganic arsenic above 15–20 mcg/L, is generally considered concerning. Treatment: DMSA (succimer) for significant inorganic arsenic toxicity; removal from exposure source; private well testing is inexpensive and recommended in high-risk regions.
Cadmium: The Smoking Metal
Cadmium is unique among common environmental heavy metals in having a very long biological half-life of 10–30 years in the kidney, which means urine cadmium reflects cumulative body burden rather than just recent exposure. Whole blood cadmium is used for acute or recent exposure assessment.
Cigarette smoking is the dominant source of cadmium exposure in non-occupationally exposed adults. Tobacco plants accumulate cadmium from soil, and smoking one cigarette approximately doubles blood cadmium. Smokers have blood cadmium 4–5 times higher than non-smokers. This is a primary and underappreciated mechanism linking smoking to kidney disease.
Other sources include: cadmium-contaminated soil and food crops (especially rice grown in high-cadmium soil — Itai-itai disease in Japan resulted from rice contaminated by industrial cadmium discharge), some phosphate fertilizers that contain cadmium as a contaminant, organ meats and shellfish (kidneys and oysters concentrate cadmium), and occupational exposure in nickel-cadmium battery manufacturing, zinc smelting, and welding operations.
Cadmium's primary target organ is the kidney. It accumulates in the proximal tubular cells and causes tubular dysfunction: aminoaciduria (amino acids in urine), glycosuria (glucose in urine without hyperglycemia), phosphaturia (phosphate wasting contributing to bone loss), and low-molecular-weight proteinuria. This is called Fanconi syndrome and eventually progresses to chronic kidney disease. Itai-itai disease ("ouch-ouch disease") described painful osteomalacia combined with renal tubular damage, causing severe bone pain and pathological fractures.
Early markers of cadmium nephrotoxicity in urine include: beta-2 microglobulin and retinol-binding protein — small proteins normally filtered and reabsorbed by proximal tubules. When tubular function is impaired, these proteins appear in urine before conventional creatinine rises. Cadmium is also a Group 1 carcinogen, primarily associated with lung cancer from inhalation and, at high exposures, kidney cancer.
There is no effective chelation for cadmium — DMSA does not meaningfully mobilize cadmium from the kidney. The primary management is cessation of exposure (especially smoking), monitoring renal function, and supportive care. Calcium and zinc adequate dietary intake may modestly reduce cadmium absorption from the gastrointestinal tract.
Other Metals in Common Panels
Comprehensive heavy metals panels may include a range of additional metals beyond the "big four" (lead, mercury, arsenic, cadmium). Most of these are relevant only in specific occupational or environmental contexts:
- Thallium: Historically used in rodenticides (now banned in most countries). Causes a characteristic syndrome: painful peripheral neuropathy followed by dramatic alopecia (complete hair loss) 2–3 weeks after exposure. High clinical specificity — unexplained alopecia + neuropathy should prompt thallium testing. Urine thallium is the standard specimen.
- Antimony: Used historically as an emetic and in modern flame retardants and semiconductor manufacturing. Toxicity resembles arsenic (gastroenteritis, peripheral neuropathy). Blood or urine specimens.
- Manganese: An essential mineral at low doses but neurotoxic from inhalation at occupational levels. Manganism is a parkinsonian syndrome from manganese inhalation in welding, smelting, and mining. Blood manganese for recent exposure; MRI of basal ganglia shows characteristic T1 hyperintensity in the globus pallidus.
- Chromium: Trivalent chromium Cr(III) is an essential trace element. Hexavalent chromium Cr(VI) is a potent carcinogen (lung cancer, nasal cancer from inhalation; basis of the Erin Brockovich case involving contaminated groundwater). Urine chromium for occupational monitoring.
- Nickel: Most commonly causes contact dermatitis (jewelry allergy). Occupational inhalation in nickel refining causes lung and nasal cancers. Urine nickel for occupational monitoring.
- Aluminum: Clinically significant primarily in dialysis patients, who cannot excrete aluminum and develop dialysis encephalopathy and osteomalacia from aluminum in dialysate water. For healthy individuals with normal kidney function, dietary aluminum from cookware and food additives is generally excreted efficiently. Serum aluminum is monitored in dialysis patients.
- Beryllium: Occupational lung disease from inhalation in aerospace, nuclear, and electronics industries. Causes chronic beryllium disease (CBD), a granulomatous lung disease similar to sarcoidosis diagnosed by beryllium lymphocyte proliferation test (BeLPT), not blood beryllium levels.
- Barium: Soluble barium salts are cardiotoxic and cause hypokalemia. Most relevant in industrial/accidental exposure. Urine barium is the standard specimen.
Chelation Therapy: Evidence and Thresholds
Chelation therapy uses molecules called chelating agents that bind metal ions and increase their urinary or fecal excretion. There are clear evidence-based indications for chelation, and there is a distinct category of chelation marketing that lacks supporting evidence and carries real risks.
Evidence-Based Indications
- DMSA (succimer, Chemet): FDA-approved oral chelator for children with BLL above 45 mcg/dL. Also used off-label for mercury and arsenic toxicity. Relatively well-tolerated; key side effects are gastrointestinal upset and transient aminotransferase elevation. Must be used with adequate hydration.
- CaNa2EDTA (calcium disodium edetate): IV chelator for severe lead poisoning, particularly lead encephalopathy. Used in combination with BAL (dimercaprol) in the most severe cases. Not appropriate for oral or home administration.
- BAL (dimercaprol, British anti-Lewisite): Originally developed for arsenic-based chemical warfare agents. Given IM, painful, and has significant toxicity including hypertension and hemolysis. Reserved for severe cases where other agents are unavailable or contraindicated.
- DMPS (dimercaptopropanesulfonate): Used in Europe for mercury and arsenic; not FDA-approved in the United States for these indications but available through compounding pharmacies. Some evidence of efficacy for inorganic mercury.
- D-penicillamine: Oral chelator used in Wilson's disease for copper chelation; also used for lead and mercury but largely superseded by DMSA for those indications due to D-penicillamine's more significant side effect profile.
The TACT Trial and EDTA in Cardiovascular Disease
The Trial to Assess Chelation Therapy (TACT) was an NIH-funded randomized controlled trial of IV EDTA infusions in post-myocardial infarction patients. The primary analysis found a statistically significant reduction in the composite cardiovascular endpoint (hazard ratio 0.82), with a larger effect in the diabetic subgroup. This generated significant controversy — the effect was modest, the trial had methodological criticisms, and TACT-2 (focused on diabetic post-MI patients) is ongoing. EDTA chelation for cardiovascular disease remains investigational and is not standard of care.
Important Cautions
- Never chelate without documented elevated metal levels. Chelation depletes essential minerals (calcium, zinc, copper, magnesium) along with toxic metals. Chelation in the absence of metal toxicity causes harm without benefit.
- Challenge/provocation testing is not a basis for prescribing chelation. Provoked urine values exceed reference ranges (which are based on spontaneous urine) in virtually everyone. Using provoked values to justify chelation in patients without symptoms or documented exposure is not evidence-based practice.
- Nephrotoxicity risk. Some chelating agents are nephrotoxic; renal function must be monitored before and during chelation.
- Re-exposure prevention is primary. Chelation without identifying and eliminating the source of exposure has limited long-term benefit — the patient will simply re-accumulate the metal.
Who Should Be Tested and Environmental Surveillance
Heavy metals testing is most valuable when ordered in the context of a plausible exposure history or compatible clinical presentation. Routine screening in asymptomatic adults without exposure risk is low-yield.
Indications for Heavy Metals Testing
- Children living in pre-1978 housing or near industrial sites: Universal childhood lead screening is recommended at ages 1 and 2 in most states; high-risk children may need earlier and more frequent screening.
- Occupational exposure: Workers in mining, smelting, battery manufacturing, electronics recycling, painting, welding, dentistry, and semiconductor fabrication should receive periodic occupational surveillance testing per OSHA standards.
- Private well water users: Particularly in high-risk regions for arsenic (New England, Midwest), lead (older homes), and other local contaminants. The EPA does not regulate private wells; owners are responsible for testing. Testing costs $20–$100 and is strongly recommended.
- Immigrants from high-exposure regions: Certain traditional cosmetics, remedies, and foods from Asia, South Asia, and Latin America have been found to contain heavy metals. Ayurvedic preparations, some kohl/surma eyeliners, azarcon, and greta have caused lead toxicity.
- Unexplained neurological symptoms: Peripheral neuropathy, parkinsonism, cognitive decline, or behavioral change in the context of possible exposure history.
- Unexplained nephropathy or cytopenias: Cadmium and lead both cause renal tubular disease; lead inhibits heme synthesis causing anemia.
- Frequent high-mercury fish consumers with neurological symptoms: Numbness, ataxia, or visual changes in a patient who eats large predatory fish multiple times per week.
- Patients with alopecia of unknown cause: Consider thallium poisoning, especially if peripheral neuropathy is also present.
Environmental Testing
Environmental surveillance — testing drinking water, paint chips, soil, and air — is often the first step and is separate from clinical blood or urine testing. A child's BLL alone does not tell you where the lead came from; environmental investigation must accompany clinical management. Home lead paint test kits are available but less accurate than laboratory analysis of paint chips and dust wipes by certified laboratories.
Research Papers and References
The following are curated PubMed literature searches covering the evidence base for heavy metals testing, clinical interpretation, and management. Each link opens a filtered PubMed query.
- Blood lead level children CDC reference value — PubMed search
- Methylmercury fish consumption neurotoxicity — PubMed search
- Inorganic arsenic carcinogen groundwater — PubMed search
- Cadmium nephrotoxicity smoking — PubMed search
- Heavy metals chelation DMSA succimer — PubMed search
- Lead poisoning chelation treatment children — PubMed search
- Mercury dental amalgam health effects — PubMed search
- Arsenic rice exposure biomarkers — PubMed search
- Cadmium kidney tubular damage — PubMed search
- Heavy metals occupational exposure monitoring — PubMed search
- Lead IQ cognitive development children — PubMed search
- EDTA chelation cardiovascular TACT trial — PubMed search
External Authoritative Resources
- MedlinePlus — Laboratory Tests Reference
- Lab Tests Online — Patient-Oriented Lab Test Reference (AACC)
- StatPearls / NCBI Bookshelf — Clinical Laboratory Reference
Connections
- All Lab Tests
- Toxic Minerals
- Lead
- Mercury
- Arsenic
- Cadmium
- Toxins
- Iron Panel
- Complete Blood Count
- Zinc Test
- Copper Test
- Kidney Disease