Beta-hCG (Pregnancy Hormone)
Beta-hCG is the blood test for human chorionic gonadotropin — the hormone the developing placenta makes in pregnancy, so widely known that it is simply called "the pregnancy hormone." It is the same hormone a home urine test looks for, but the blood version measures the exact amount rather than giving a plain yes or no. Because of that precision, beta-hCG does far more than confirm a pregnancy: it helps date an early pregnancy, watch a pregnancy that a doctor is worried about, and flag serious problems such as an ectopic (tubal) pregnancy or a miscarriage in progress. Outside of pregnancy it has a second life as a tumor marker for a small group of cancers. This page explains, in plain language, what the hormone is, how the test is used, what the numbers mean, and where the test can mislead. Pregnancy is deeply personal and often anxious territory, so the goal here is to inform and steady you — not to replace the doctor or midwife who knows your specific situation.
Table of Contents
- What hCG Is
- Qualitative vs. Quantitative
- Why the Test Is Ordered in Pregnancy
- Dating and the 48-Hour Doubling
- Ectopic Pregnancy and Miscarriage
- The Discriminatory Zone
- Beta-hCG as a Tumor Marker
- How It Is Measured and When
- Interpreting the Numbers
- False Positives and False Negatives
- When to Talk to a Doctor
- Research Papers
- Connections
- Featured Videos
What hCG Is
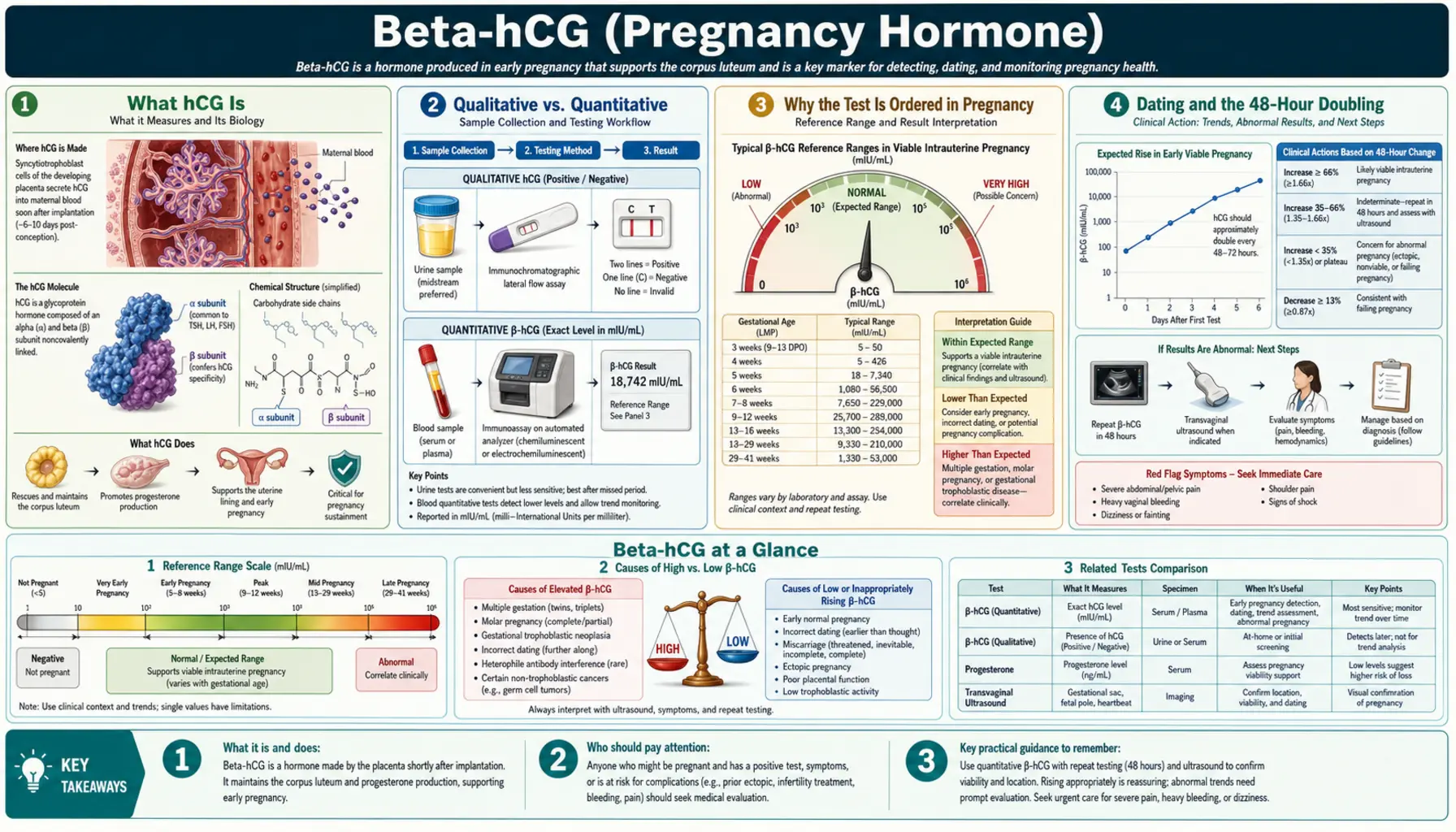
Human chorionic gonadotropin (hCG) is a hormone produced by the placenta — specifically by the layer of cells called the syncytiotrophoblast that forms as a fertilized egg implants into the wall of the uterus. Its most important early job is to send a signal to the ovary that keeps a small structure called the corpus luteum alive. The corpus luteum, in turn, keeps making progesterone, and progesterone is what holds the uterine lining in place so the pregnancy can continue. In plain terms: hCG is the message that tells the body "a pregnancy has started, keep it going."
The hormone is built from two joined pieces, called subunits. The alpha subunit is nearly identical to a part of several other hormones your pituitary gland makes (LH, FSH, and TSH). The beta subunit is unique to hCG. That uniqueness is exactly why the test is called beta-hCG: laboratories aim their measurement at the beta subunit so they are reading hCG specifically, and not accidentally counting look-alike hormones. When someone says a "beta" was drawn, they mean this quantitative blood test.
hCG appears in the bloodstream very early — usually around eight to eleven days after conception, once implantation has occurred. It rises quickly through the first weeks, peaks around the tenth to twelfth week of pregnancy, and then falls to a lower, steadier level for the rest of the pregnancy. Understanding that rise-and-fall pattern is the key to almost everything the test is used for.
Qualitative vs. Quantitative
There are two very different ways to test for hCG, and the difference matters.
A qualitative test answers a single question: is hCG present or not? The drugstore home pregnancy test is the familiar example. You place urine on a stick, and a line (or a "pregnant" / "not pregnant" readout) tells you yes or no. Clinics use qualitative urine tests too, as a fast first check. These tests are simple, cheap, private, and remarkably good — but they only give a yes-or-no.
A quantitative test — the beta-hCG blood test — measures the actual concentration of the hormone and reports a number in units called milli-international units per milliliter (mIU/mL). Instead of "pregnant," you get something like "hCG = 340." That number is what makes the blood test so much more powerful. It can be repeated in two or three days and compared, so a doctor can see whether the level is rising normally, rising too slowly, plateauing, or falling.
Blood testing is also more sensitive and can turn positive earlier. Most quantitative blood assays can detect hCG at very low levels — often around 1 to 5 mIU/mL — whereas many home urine tests need roughly 20 to 25 mIU/mL to show a reliable positive. In practice that means a blood test may confirm a pregnancy a few days sooner than a urine test, and can do so with a precise starting value. The trade-off is that the blood test requires a blood draw and a laboratory, so home urine testing remains the everyday tool and the blood beta is reserved for when the number, or the trend, actually changes what happens next.
Why the Test Is Ordered in Pregnancy
In an uncomplicated, healthy pregnancy, you may never need a quantitative beta-hCG at all — a positive urine test and a well-timed ultrasound tell the story. Doctors reach for the blood test when the number itself will guide a decision. Common reasons include:
- Confirming a pregnancy when a urine test is unclear, or very early, or when a precise baseline is wanted before other care.
- Estimating how far along a pregnancy is before an ultrasound can show much, since hCG tracks loosely with the weeks since conception.
- Following a pregnancy of uncertain location or health — for example when there is bleeding, cramping, or pain, or when an early ultrasound cannot yet find the pregnancy inside the uterus.
- Monitoring after a fertility treatment such as IVF, where the timing and rise of hCG are watched closely.
- Checking that levels fall to zero after a miscarriage, a treated ectopic pregnancy, or a molar pregnancy, to confirm the process is complete.
The theme running through all of these is that a beta-hCG is most useful when it is either giving a precise starting point or being repeated to reveal a trend. A single number, taken alone, almost never tells the whole story.
Dating and the 48-Hour Doubling
Early in a normal, healthy pregnancy located in the uterus, hCG rises fast — the classic teaching is that it roughly doubles about every 48 to 72 hours. That doubling is why two blood draws spaced two or three days apart can be so informative. If the level is climbing as expected, it is reassuring; if it is barely rising or falling, it points toward a problem that needs a closer look.
It helps to know that "doubling" is a rule of thumb, not a law. Careful research has shown that the minimum rise still compatible with a potentially healthy pregnancy is slower than a true doubling. In one influential study of women with pain or bleeding but an ultimately viable pregnancy, the slowest normal two-day rise was on the order of 50 percent, and later work put the floor even a little lower. The practical takeaway is gentle but important: a rise that is somewhat less than a perfect doubling can still be fine, which is exactly why doctors avoid drawing hard conclusions from one pair of numbers and instead look at the whole picture — symptoms, ultrasound, and the trend over time.
It also helps to know the ceiling on this trick. The doubling pattern is only reliable at relatively low levels, roughly below 6,000 mIU/mL. Once hCG climbs higher, the rise naturally slows even in a perfectly healthy pregnancy, so a slower rise late in the first trimester is expected and not a warning sign. By that point, ultrasound has taken over as the better tool.
Ectopic Pregnancy and Miscarriage
This is one of the most genuinely important uses of beta-hCG, and it deserves a plain, calm explanation.
An ectopic pregnancy is one that implants outside the uterus — most often in a fallopian tube. It cannot develop into a baby, and because a tube can rupture and cause dangerous internal bleeding, an ectopic pregnancy is a situation that needs prompt medical attention. hCG helps in a specific way: in an ectopic pregnancy the hormone is usually present but tends to rise abnormally slowly, without the healthy near-doubling, and an ultrasound cannot find the pregnancy inside the uterus. Importantly, hCG alone does not diagnose an ectopic pregnancy. It is one piece of a puzzle that also includes symptoms and ultrasound; the pattern of a positive test, a slow or plateauing rise, and an empty uterus on ultrasound is what raises concern.
A miscarriage (early pregnancy loss) shows a different hormone pattern: hCG that is falling, or that rose abnormally slowly and then stalled. As with an ectopic, a single value cannot confirm a loss — but a clearly declining trend, together with the clinical picture, can. When a loss is confirmed or an ectopic is treated, doctors often keep drawing beta-hCG until it returns all the way to zero, which is how they know the process is truly finished.
If you are reading this while waiting on your own results, please be gentle with yourself. These tests exist precisely to catch problems early and keep you safe, and a worrying single number is not a verdict — it is a reason for the next look, not the last word.
The Discriminatory Zone
The discriminatory zone is the hCG level above which a normal pregnancy inside the uterus should be visible on a transvaginal ultrasound. The idea is simple and useful: if hCG is above that threshold and the ultrasound still shows an empty uterus, it raises the possibility that the pregnancy is somewhere it should not be (an ectopic) or is not developing normally.
For years the discriminatory zone was quoted as roughly 1,500 to 2,000 mIU/mL. More recent evidence has pushed clinicians toward a deliberately higher and more cautious threshold — often around 3,500 mIU/mL — for a compassionate reason. Occasionally a perfectly healthy, wanted pregnancy simply is not visible yet even at 2,000 mIU/mL, especially with twins or slightly off dates. Using a higher threshold before calling a pregnancy abnormal makes it far less likely that a viable pregnancy is mistakenly ended. In other words, the number was raised specifically to protect pregnancies that are actually fine. The discriminatory zone is best understood as a caution flag that prompts more watching and repeat testing — not a switch that decides anything by itself.
Beta-hCG as a Tumor Marker
hCG is famous as the pregnancy hormone, but a handful of tumors can also produce it, which makes beta-hCG a valuable tumor marker in a few specific cancers. When hCG turns up in someone who is not pregnant — or in a man — it can be an important clue.
The main uses are:
- Germ-cell tumors of the testicle and ovary. Some of these tumors secrete hCG, and beta-hCG is measured alongside two other markers (AFP and LDH) to help diagnose them, judge how advanced they are, and monitor whether treatment is working. A rising marker after treatment can signal that cancer has returned, sometimes before it can be seen on a scan.
- Gestational trophoblastic disease, which includes molar pregnancy (an abnormal growth of placenta-like tissue) and its rare cancerous forms such as choriocarcinoma. These conditions can drive hCG to strikingly high levels, and the hormone is central both to diagnosing them and to following treatment. Because the tissue comes from placental cells, it produces hCG in abundance, and watching the level fall to zero is how doctors confirm a cure.
Rarely, other cancers can produce small amounts of hCG. In cancer care, as in pregnancy, the trend over time usually matters more than any single value: a marker that keeps falling after treatment is reassuring, while one that rises prompts a closer look.
How It Is Measured and When
A quantitative beta-hCG is a routine blood test. A small sample is drawn from a vein in the arm and sent to a laboratory, where an automated immunoassay measures the hormone and reports a number in mIU/mL. There is nothing special to do beforehand — no fasting, no special preparation. Results are often available the same day.
Timing is where a little knowledge helps:
- Too early can mean too low. Before implantation, hCG is not yet in the blood, so a test drawn very soon after conception can be negative even when pregnancy is on its way. If a very early result is negative but a period has not arrived, repeating in a few days is reasonable.
- Trends need spacing. When the point is to watch a rise or fall, draws are usually spaced about 48 hours apart — enough time for a meaningful change, ideally at the same lab, since different laboratories can report slightly different numbers.
- Same method, same lab. Comparing two values run by the same method avoids being misled by differences between assays. If your care shifts between clinics, mention it, because the reference values may differ.
Home urine tests follow their own timing rules: first-morning urine is the most concentrated and gives the earliest reliable positive, and testing after the day a period is due improves accuracy.
Interpreting the Numbers
Perhaps the most common source of anxiety with beta-hCG is a single number and the urge to compare it to someone else's. Here is the honest, reassuring truth: the normal range is enormous, and a single value tells you much less than the trend.
hCG levels vary so widely by week of pregnancy — and from person to person at the same week — that published ranges span from double digits to the hundreds of thousands. As a rough illustration of the scale (not a diagnostic table): a few weeks after a missed period, values commonly range anywhere from a few dozen to several thousand mIU/mL, and around the peak near weeks ten to twelve they can reach the tens of thousands to over a hundred thousand. Two healthy pregnancies at exactly the same stage can have hCG numbers several times apart and both be perfectly normal.
Because of that spread, doctors rarely read much into one value. What they watch instead is:
- The trend — is it rising appropriately, plateauing, or falling?
- The clinical picture — bleeding, pain, prior history, and dates.
- The ultrasound — especially once levels reach the range where a pregnancy should be visible.
So if your first beta comes back and you cannot tell from the number alone whether things are fine, that is normal — it usually cannot. The number is a starting point, and the story is written over the following days.
False Positives and False Negatives
hCG testing is very reliable, but no test is perfect. Knowing the handful of ways it can mislead helps you interpret an unexpected result calmly.
False negatives
- Testing too early. The most common cause — hCG simply has not risen high enough to detect yet. Retesting in a few days usually resolves it.
- Dilute urine. Drinking a lot of fluid before a home test waters down the sample and can push a faint positive below the line; first-morning urine avoids this.
- The "hook effect." At extraordinarily high hCG levels — as can occur with a molar pregnancy or, occasionally, a very high normal pregnancy — the test chemistry can become overwhelmed and paradoxically read low or even negative. Laboratories fix this by diluting the sample and re-running it. It is rare, but it is why a "negative" result that does not fit the clinical picture is always questioned.
False positives
- Heterophile antibodies. A small number of people have antibodies in their blood that interfere with the assay and produce a falsely positive serum hCG — sometimes called "phantom hCG." A classic clue is that the blood test is positive while a urine test is negative, because these interfering antibodies do not pass into urine. Recognizing this pattern prevents unnecessary treatment.
- Recent hCG injections. Some fertility treatments use an hCG "trigger shot"; testing too soon afterward can detect that injected hormone rather than a pregnancy.
- Evaporation lines and misreads. On home tests, a faint mark that appears after the reading window is usually an evaporation line, not a true positive — read within the time the instructions specify.
When a result does not match how someone feels or what an ultrasound shows, a good clinician treats the mismatch itself as the finding worth investigating — repeating the test, switching methods, or checking urine against blood.
When to Talk to a Doctor
Beta-hCG is a tool your care team uses; it is not something to interpret alone from an online chart. Reach out to a doctor or midwife when:
- You have a positive pregnancy test along with abdominal or pelvic pain, shoulder-tip pain, dizziness or fainting, or vaginal bleeding — these can be signs of an ectopic pregnancy and warrant prompt evaluation.
- Your beta-hCG is not rising as expected, is plateauing, or is falling, and you have not been told what it means.
- A home test and a clinical test disagree, or results simply do not match how you feel.
- You are going through fertility treatment, a known high-risk pregnancy, or follow-up after a miscarriage, ectopic, or molar pregnancy — where structured beta-hCG monitoring is part of your care.
- hCG is detected and you are not or cannot be pregnant, which should always be explained rather than dismissed.
Above all, remember that a number on a page is only part of the story. The people caring for you will read it together with your symptoms, your history, and your ultrasound — and they are the right ones to tell you what your particular result means.
Research Papers
- Barnhart KT, Sammel MD, Rinaudo PF, et al. Symptomatic patients with an early viable intrauterine pregnancy: hCG curves redefined. Obstetrics & Gynecology. 2004;104(1):50-55. doi:10.1097/01.AOG.0000128174.48843.12 — the landmark study showing the minimum normal two-day hCG rise is slower than a true doubling.
- Connolly A, Ryan DH, Stuebe AM, et al. Reevaluation of discriminatory and threshold levels for serum β-hCG in early pregnancy. Obstetrics & Gynecology. 2013;121(1):65-70. doi:10.1097/AOG.0b013e318278f421 — evidence supporting a higher, more cautious discriminatory zone to protect viable pregnancies.
- Barnhart KT. Ectopic pregnancy. New England Journal of Medicine. 2009;361(4):379-387. doi:10.1056/NEJMcp0810384 — a widely cited clinical review of how hCG and ultrasound are used to evaluate a possible ectopic.
- American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 193: Tubal ectopic pregnancy. Obstetrics & Gynecology. 2018;131(3):e91-e103. doi:10.1097/AOG.0000000000002560 — the authoritative U.S. guideline on diagnosing and managing tubal ectopic pregnancy.
- Doubilet PM, Benson CB, Bourne T, et al. Diagnostic criteria for nonviable pregnancy early in the first trimester. New England Journal of Medicine. 2013;369(15):1443-1451. doi:10.1056/NEJMra1302417 — consensus criteria that deliberately avoid calling an early pregnancy nonviable too soon.
- Cole LA. New discoveries on the biology and detection of human chorionic gonadotropin. Reproductive Biology and Endocrinology. 2009;7:8. doi:10.1186/1477-7827-7-8 — a thorough review of hCG's forms, biology, and how assays detect it.
- Griffey RT, Trent CJ, Bavolek RA, et al. "Hook-like effect" causes false-negative point-of-care urine pregnancy testing in emergency patients. The Journal of Emergency Medicine. 2013;44(1):155-160. doi:10.1016/j.jemermed.2011.05.032 — documents how very high hCG can produce a falsely negative test.
- Gronowski AM, Cervinski M, Stenman UH, et al. False-negative results in point-of-care qualitative human chorionic gonadotropin (hCG) devices due to excess hCGβ core fragment. Clinical Chemistry. 2009;55(7):1389-1394. doi:10.1373/clinchem.2008.121210 — explains a specific chemistry cause of false-negative urine tests.
- Braunstein GD. False-positive serum human chorionic gonadotropin results: causes, characteristics, and recognition. American Journal of Obstetrics and Gynecology. 2002;187(1):217-224. doi:10.1067/mob.2002.124284 — the classic paper on heterophile-antibody "phantom hCG" false positives.
- Sturgeon CM, Duffy MJ, Stenman UH, et al. National Academy of Clinical Biochemistry laboratory medicine practice guidelines for use of tumor markers in testicular, prostate, colorectal, breast, and ovarian cancers. Clinical Chemistry. 2008;54(12):e11-e79. doi:10.1373/clinchem.2008.105601 — guideline covering hCG's role as a tumor marker in germ-cell cancers.
- Gilligan TD, Seidenfeld J, Basch EM, et al. American Society of Clinical Oncology clinical practice guideline on uses of serum tumor markers in adult males with germ cell tumors. Journal of Clinical Oncology. 2010;28(20):3388-3404. doi:10.1200/JCO.2009.26.4481 — how beta-hCG, AFP, and LDH are used to stage and monitor testicular germ-cell tumors.
- Seckl MJ, Sebire NJ, Berkowitz RS. Gestational trophoblastic disease. The Lancet. 2010;376(9742):717-729. doi:10.1016/S0140-6736(10)60280-2 — comprehensive review of molar pregnancy and choriocarcinoma, where hCG guides diagnosis and follow-up.
Connections
- Hormone Panel
- Testosterone Test
- AMH (Anti-Müllerian Hormone)
- DHEA-S
- SHBG
- AFP Test (Alpha-Fetoprotein)
- CA-125 Test
- Reproductive Medicine
- Oncology
- All Lab Tests