SHBG (Sex Hormone Binding Globulin) Test
Sex hormone binding globulin (SHBG) is a protein your liver makes that grabs onto your sex hormones — testosterone, DHT, and estrogen — and carries them through your bloodstream. While a hormone is held by SHBG, it is essentially in storage: it cannot act on your tissues. Only the small unbound, or "free," fraction is available to do its job. That makes SHBG a kind of thermostat for how much of your hormones are actually working, which is why a doctor almost never orders it on its own. It is usually run alongside a total testosterone (or estrogen) test to figure out what the total number really means.
SHBG has a second, less obvious use that has drawn a lot of research attention: a low SHBG level is one of the earliest and most reliable blood markers of insulin resistance and metabolic syndrome, and it turns out to predict the future risk of type 2 diabetes. This page explains what SHBG does, why the test is ordered, what pushes it up or down, how to read your result, and how to prepare.
Table of Contents
- What SHBG Is
- Free vs. Total Hormone: Why SHBG Matters
- Why Doctors Order an SHBG Test
- What Raises and Lowers SHBG
- Low SHBG, Insulin Resistance & Diabetes Risk
- Understanding Your Results & Reference Ranges
- How the Test Is Done & How to Prepare
- Key Takeaways
- Research Papers
- Connections
- Featured Videos
What SHBG Is
Sex hormone binding globulin is a transport protein produced mainly by the liver and released into the bloodstream. Its job is to bind sex steroid hormones and ferry them around the body. It does not bind all hormones equally — the strength of its grip matters:
- Dihydrotestosterone (DHT) — bound most tightly of all.
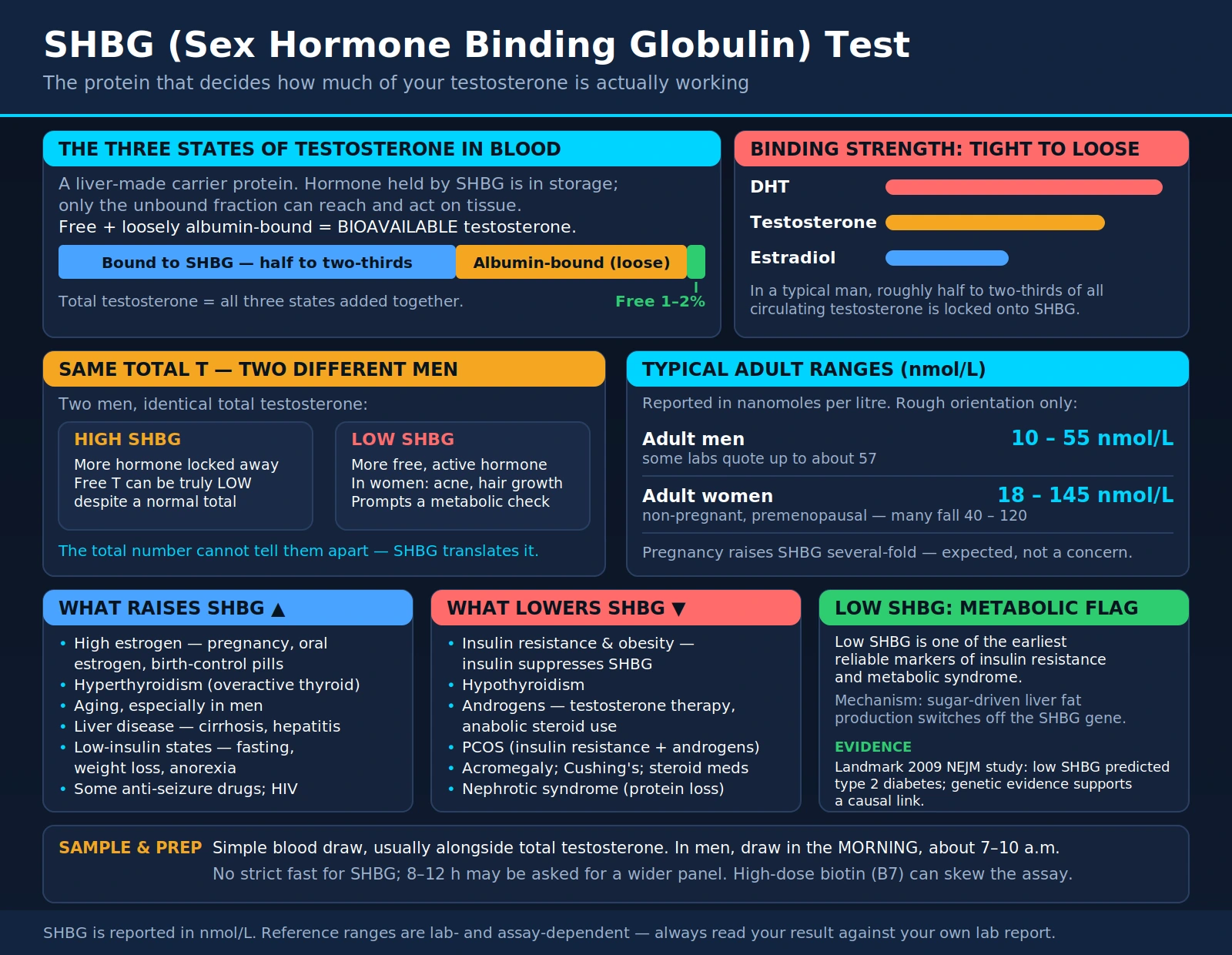
- Testosterone — bound tightly. In a typical man, roughly half to two-thirds of all circulating testosterone is locked onto SHBG.
- Estradiol (the main estrogen) — bound, but more loosely than testosterone.
A helpful way to picture it: think of your hormones as passengers and SHBG as a fleet of taxis with the doors locked. A passenger riding in a locked taxi cannot get out to do any work. Only the passengers walking on the sidewalk — the "free" hormone — can actually reach the tissues and have an effect. SHBG decides how many passengers are stuck in taxis versus free to walk around.
Because SHBG is made by the liver, anything that changes how hard the liver works to produce it — hormones, insulin, thyroid status, liver health, age — will change your SHBG level, and therefore change the balance between bound and free hormone. That sensitivity is exactly what makes SHBG both useful and, at times, confusing to interpret.
Free vs. Total Hormone: Why SHBG Matters
To understand why SHBG is almost always ordered together with a testosterone test, it helps to know that the testosterone in your blood exists in three states at once:
- Tightly bound to SHBG — the largest slice. This testosterone is held firmly and is not available to your tissues.
- Loosely bound to albumin — another protein in blood. This bond is weak, so the hormone can slip off fairly easily and be used.
- Free — completely unbound, usually only about 1–2% of the total. This fraction is immediately available.
The free portion plus the loosely albumin-bound portion together are called bioavailable testosterone — the hormone that can actually reach and act on cells. The total testosterone that most basic panels report simply adds up all three states together.
Here is why that distinction is the whole point of the SHBG test. Imagine two men with the exact same total testosterone. If one has very high SHBG, most of his testosterone is locked away and he may feel and function as though he is low on testosterone. If the other has very low SHBG, more of his testosterone is free and active, and he may be perfectly fine. The single total number cannot tell them apart — you need SHBG to translate a total testosterone into a meaningful picture of active hormone.
In practice, a lab or clinician combines total testosterone, SHBG, and albumin into a calculated free testosterone using a well-validated equation. This calculation is inexpensive, widely used, and generally tracks the more elaborate laboratory reference methods well enough for everyday care. It is the reason your provider may draw all three at once.
Why Doctors Order an SHBG Test
SHBG is a supporting test. It is ordered when a total hormone level alone leaves questions unanswered. Common reasons include:
- To interpret a total testosterone result. This is the number-one reason. When total testosterone sits near the low or high edge of normal, SHBG (and the calculated free testosterone it enables) clarifies whether the active hormone is truly low, normal, or high.
- Low-testosterone symptoms with a "normal" total T. A man with fatigue, low libido, erectile difficulty, or loss of muscle may have a total testosterone that looks acceptable on paper. If his SHBG is high, his free testosterone can still be low — explaining the symptoms the total number missed.
- Signs of excess androgens in women. In women with hirsutism (unwanted coarse hair growth), stubborn acne, scalp hair thinning, or irregular periods, a low SHBG raises the fraction of free, active testosterone even when total testosterone is only mildly elevated. SHBG is a routine part of the workup for polycystic ovary syndrome (PCOS).
- Evaluating fertility and sexual dysfunction in both sexes, where the balance of bioavailable hormones is more informative than totals.
- As a window into metabolic health. Because low SHBG tracks so closely with insulin resistance, some clinicians read it as an early flag for metabolic risk (see the section below).
SHBG is not a screening test for the general public and is not something most healthy people ever need. It earns its keep when a hormone picture does not add up.
What Raises and Lowers SHBG
Because the liver tunes SHBG production in response to the body's hormonal and metabolic state, a long list of conditions moves it. Knowing the direction helps you make sense of an unexpected result — a "high" or "low" SHBG is often a clue about something else entirely.
Things that RAISE SHBG
- High estrogen. Pregnancy raises SHBG several-fold; so do oral estrogen therapy and estrogen-containing birth control pills. (Estrogen taken through the skin as a patch or gel has much less effect, because it bypasses the liver.)
- Hyperthyroidism (an overactive thyroid) — thyroid hormone stimulates SHBG production.
- Aging, especially in men, where SHBG tends to drift upward over the decades.
- Liver disease such as cirrhosis and hepatitis, which alter the liver's hormone handling.
- Low insulin states — fasting, meaningful weight loss, calorie restriction, and eating disorders such as anorexia. When insulin is low, the liver makes more SHBG.
- Certain medications, including some anti-seizure drugs, and conditions such as HIV infection.
Things that LOWER SHBG
- Insulin resistance and obesity. This is the big one. High insulin levels suppress the liver's production of SHBG, so excess body fat and metabolic syndrome are strongly linked to low SHBG.
- Hypothyroidism (an underactive thyroid) — the mirror image of the hyperthyroid effect.
- Androgens — testosterone therapy and anabolic steroid use push SHBG down.
- Polycystic ovary syndrome (PCOS), which combines insulin resistance with higher androgens — a double push toward low SHBG.
- Excess growth hormone (acromegaly) and Cushing's syndrome / high-dose glucocorticoid (steroid) medication.
- Nephrotic syndrome and some other conditions that cause the body to lose protein.
Notice the pattern: estrogen and thyroid hormone tend to raise SHBG, while insulin and androgens tend to lower it. That is why interpreting your number always means asking, "What else is going on with this person?"
Low SHBG, Insulin Resistance & Diabetes Risk
One of the most important and well-supported findings about SHBG is that a low level is a genuine marker of insulin resistance and metabolic syndrome — and it does more than just travel alongside those conditions. It appears to help predict who will develop type 2 diabetes years down the road.
The mechanism is elegant and now fairly well understood. Laboratory work has shown that the liver dials SHBG production up or down in response to how much fat it is building. When you take in a lot of sugar — particularly fructose and glucose — the liver ramps up fat synthesis (a process called lipogenesis), and this directly switches off the SHBG gene. High insulin, the hallmark of insulin resistance, drives that same fat-building state. So low SHBG is not a random coincidence with metabolic disease; it is a readout of what is happening inside liver cells.
The clinical evidence is striking. A landmark 2009 study followed thousands of women and men and found that people with low SHBG were markedly more likely to develop type 2 diabetes. Crucially, it used genetic evidence — naturally occurring gene variants that set a person's SHBG higher or lower from birth — and found the same pattern, which is a powerful sign that the relationship is causal rather than a mere association. A separate large genetic study the following year reached the same conclusion: variants that raise SHBG reduce diabetes risk. Later reviews have confirmed that low SHBG is one of the strongest single-protein predictors of future diabetes we have.
What does this mean for you? If your SHBG comes back low and you were not expecting it, it is worth having a conversation about your metabolic health — blood sugar, insulin, waist size, blood pressure, and lipids. A low SHBG can be an early, quiet signal, sometimes showing up before fasting glucose drifts out of range. The encouraging flip side is that the very things that improve insulin sensitivity — losing excess weight, cutting refined sugar, and exercising — also tend to raise SHBG back up.
Understanding Your Results & Reference Ranges
SHBG is reported in nanomoles per liter (nmol/L). There is no single universal "normal" range — it depends heavily on your sex, your age, and the specific assay your laboratory uses. Always read your result against the reference range printed on your own lab report, not a number from the internet. As a rough orientation only, typical adult ranges look something like this:
- Adult men: roughly 10 to 55 nmol/L (some labs quote up to about 57).
- Adult women (non-pregnant, before menopause): roughly 18 to 145 nmol/L, with many premenopausal women falling in the 40 to 120 range.
- Pregnancy raises SHBG dramatically — several times above normal — which is expected and not a concern.
Two points matter more than the exact numbers. First, SHBG is almost never interpreted alone. It is read together with your total testosterone (and often estradiol, albumin, and a calculated free testosterone) to build the real picture. A given SHBG is only "good" or "bad" in the context of those other values and your symptoms.
Second, think about the direction:
- A high SHBG means more of your hormones are bound and inactive. With a borderline total testosterone, high SHBG can leave free testosterone genuinely low — a common explanation for low-T symptoms despite a "normal" total. High SHBG points toward causes like hyperthyroidism, liver disease, estrogen exposure, or simply aging.
- A low SHBG means more free, active hormone is circulating. In women this can amplify symptoms of excess androgens (acne, hair growth). In anyone, an unexpectedly low SHBG is a prompt to look at insulin resistance, obesity, hypothyroidism, or androgen use.
Reference ranges also shift with age and across the lifespan, and men's and women's ranges differ substantially, so a result that is normal for one person may be unusual for another. Your clinician interprets the number in light of who you are and why the test was ordered.
How the Test Is Done & How to Prepare
The SHBG test is a simple blood draw from a vein in your arm, usually taking only a minute or two. It is frequently drawn at the same time as a total testosterone and other hormones so everything reflects the same moment. A few practical points help make the result reliable:
- Timing. When SHBG is paired with a testosterone level in men, the blood is ideally drawn in the morning, roughly between 7 and 10 a.m., because testosterone follows a daily rhythm and peaks early. SHBG itself is more stable across the day, but morning sampling keeps the accompanying hormones meaningful.
- Fasting. SHBG does not strictly require fasting, but because it is often bundled into a broader hormone or metabolic panel that does, you may be asked to fast for 8–12 hours. Follow the instructions your provider gives for the whole panel.
- Biotin supplements. High-dose biotin (vitamin B7, found in many "hair, skin, and nails" products) can interfere with some laboratory immunoassays and skew hormone results. It is commonly recommended to stop biotin for a day or two before the draw — ask your lab. Mention any supplement to whoever draws your blood.
- Medications and hormones matter. Estrogen (including birth control pills and hormone therapy), thyroid medication, testosterone or anabolic steroids, and corticosteroids all move SHBG. Tell your provider everything you take so the result can be read correctly — do not stop any prescription on your own.
- Recent illness, weight change, or crash dieting can temporarily shift SHBG. If any of these apply, let your clinician know.
There is no special recovery needed afterward; you can return to normal activities right away. Results are typically available within a few days.
Key Takeaways
- SHBG is a liver-made carrier protein that binds testosterone, DHT, and estrogen, controlling how much hormone is "free" and able to act.
- It is ordered to interpret total testosterone, not usually on its own — it powers the calculated free testosterone that explains many hormone puzzles.
- High SHBG (hyperthyroidism, liver disease, estrogen, aging) locks hormones away and can leave free testosterone low despite a normal total.
- Low SHBG (insulin resistance, obesity, hypothyroidism, androgens, PCOS) leaves more free, active hormone circulating.
- A low SHBG is a recognized early marker of insulin resistance and metabolic syndrome, and genetic evidence suggests it helps predict type 2 diabetes — making it a useful metabolic warning sign, not just a hormone number.
- Always read your result against your own lab's reference range, alongside your other hormone values and your symptoms.
Research Papers
- Ding EL, Song Y, Manson JE, Hunter DJ, Lee CC, Rifai N, et al. Sex hormone–binding globulin and risk of type 2 diabetes in women and men. New England Journal of Medicine. 2009;361(12):1152–1163. doi:10.1056/NEJMoa0804381 — The landmark study; low SHBG strongly predicted diabetes, and genetic (Mendelian randomization) evidence supported a causal link.
- Perry JR, Weedon MN, Langenberg C, Jackson AU, Lyssenko V, Sparsø T, et al. Genetic evidence that raised sex hormone binding globulin (SHBG) levels reduce the risk of type 2 diabetes. Human Molecular Genetics. 2010;19(3):535–544. doi:10.1093/hmg/ddp522 — A large genetic study confirming that variants raising SHBG lower diabetes risk.
- Selva DM, Hogeveen KN, Innis SM, Hammond GL. Monosaccharide-induced lipogenesis regulates the human hepatic sex hormone–binding globulin gene. Journal of Clinical Investigation. 2007;117(12):3979–3987. doi:10.1172/JCI32249 — The mechanistic paper showing how sugar-driven liver fat production switches off the SHBG gene, explaining the insulin-resistance link.
- Le TN, Nestler JE, Strauss JF, Wickham EP. Sex hormone-binding globulin and type 2 diabetes mellitus. Trends in Endocrinology & Metabolism. 2012;23(1):32–40. doi:10.1016/j.tem.2011.09.005 — A clear review connecting SHBG, insulin resistance, and diabetes.
- Wallace IR, McKinley MC, Bell PM, Hunter SJ. Sex hormone binding globulin and insulin resistance. Clinical Endocrinology. 2013;78(3):321–329. doi:10.1111/cen.12086 — Reviews the evidence that SHBG is a marker — and possibly a mediator — of insulin resistance.
- Simó R, Sáez-López C, Barbosa-Desongles A, Hernández C, Selva DM. Novel insights in SHBG regulation and clinical implications. Trends in Endocrinology & Metabolism. 2015;26(7):376–383. doi:10.1016/j.tem.2015.05.001 — Updates on how SHBG is regulated and why it matters clinically.
- Vermeulen A, Verdonck L, Kaufman JM. A critical evaluation of simple methods for the estimation of free testosterone in serum. The Journal of Clinical Endocrinology & Metabolism. 1999;84(10):3666–3672. doi:10.1210/jcem.84.10.6079 — The widely used equation for calculating free testosterone from total testosterone, SHBG, and albumin.
- Goldman AL, Bhasin S, Wu FCW, Krishna M, Matsumoto AM, Jasuja R. A reappraisal of testosterone's binding in circulation: physiological and clinical implications. Endocrine Reviews. 2017;38(4):302–324. doi:10.1210/er.2017-00025 — A detailed look at how testosterone binds SHBG and albumin and what "free" and "bioavailable" really mean.
- Hammond GL. Plasma steroid-binding proteins: primary gatekeepers of steroid hormone action. Journal of Endocrinology. 2016;230(1):R13–R25. doi:10.1530/JOE-16-0070 — An overview of SHBG's role as a gatekeeper controlling hormone availability.
- Bhasin S, Brito JP, Cunningham GR, Hayes FJ, Hodis HN, Matsumoto AM, et al. Testosterone therapy in men with hypogonadism: an Endocrine Society clinical practice guideline. The Journal of Clinical Endocrinology & Metabolism. 2018;103(5):1715–1744. doi:10.1210/jc.2018-00229 — The clinical guideline describing when free testosterone (via SHBG) should be measured to diagnose low testosterone.