Mullein for Ear Health and Ear Infections
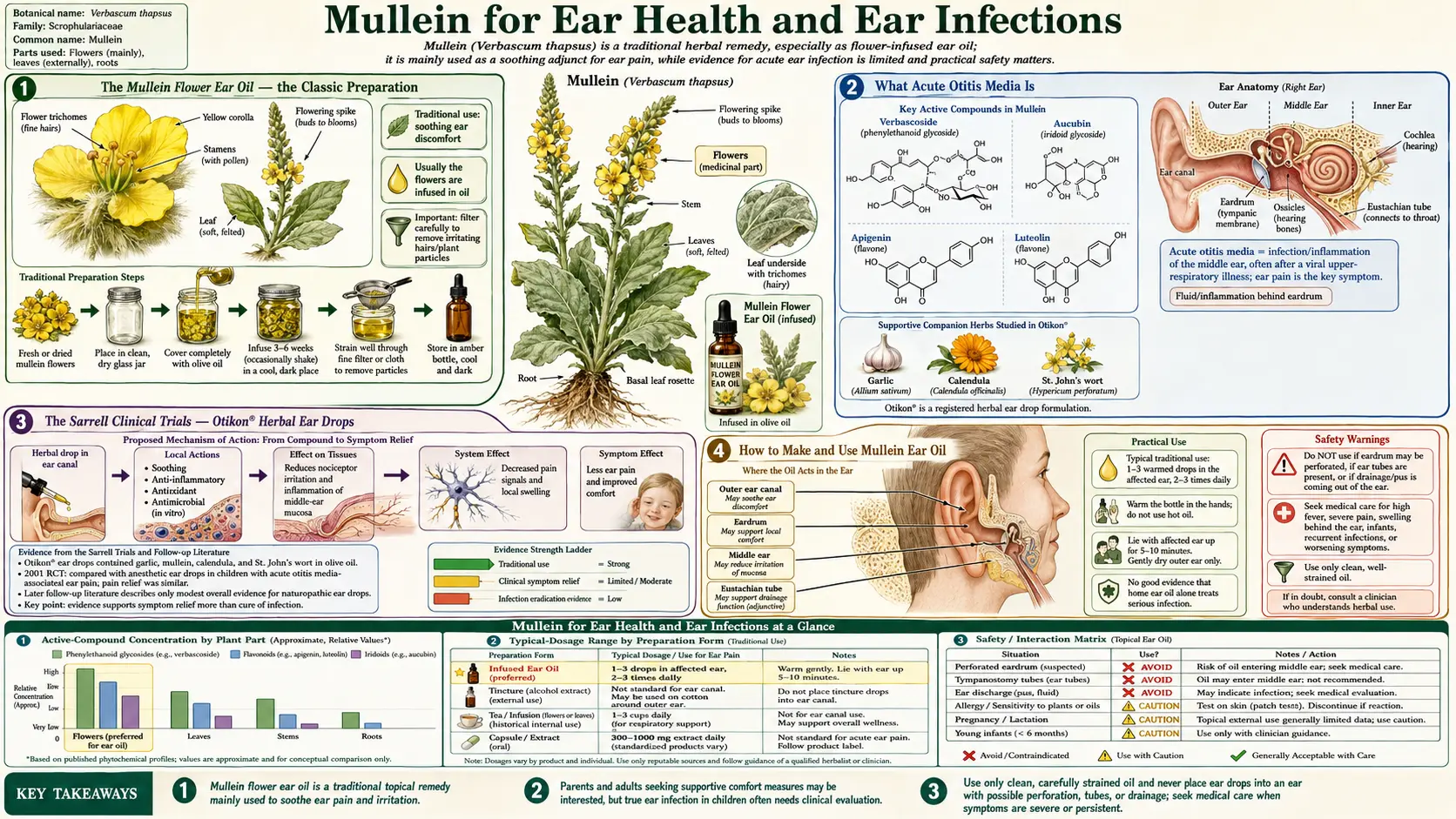
Table of Contents
- Mullein Flower Ear Oil — the Classic Preparation
- What Acute Otitis Media Is
- The Sarrell Clinical Trials — Otikon Herbal Ear Drops
- How to Make and Use Mullein Ear Oil
- Why It May Soothe the Ear
- Critical Safety — When You Must Not Use Ear Oil
- Combining Mullein with Garlic
- Pediatric Considerations and the Limits of the Evidence
- Evidence Summary
- Cautions
- Research Papers and References
- Connections
- Featured Videos
Mullein Flower Ear Oil — the Classic Preparation
Mullein (Verbascum thapsus) is best known in folk medicine for two organ systems: the lungs and the ears. Of these, the use that has filtered most directly into the modern herbal cabinet is mullein flower ear oil — the bright yellow flowers of the plant slowly infused into a warm carrier oil, then strained and dripped into an aching ear. Walk into almost any natural-foods store and you will find a small amber dropper bottle labeled "Mullein Garlic Ear Oil" or "Children's Earache Oil," and mullein is nearly always the headline botanical.
The preparation is genuinely old. Eclectic physicians of the nineteenth century, and the broader European and Appalachian folk traditions before them, used oil infusions of mullein flowers as a topical remedy for the pain of earache. The flowers were valued specifically — not the leaf, which is the part used for cough — because they carry a soothing, demulcent, slightly mucilaginous quality and a set of constituents (flavonoids, iridoid glycosides such as aucubin, and saponins) that the tradition associated with calming inflamed tissue.
It is worth being precise about what mullein ear oil is and is not. It is a symptomatic comfort measure for the pain of an intact-eardrum earache, used while the body's own immune response resolves the underlying problem. It is not an antibiotic, it does not drain a middle-ear effusion that sits behind the eardrum, and — as the safety section below stresses — it must never be poured into an ear when the eardrum may be perforated. Understanding that distinction is the single most important thing on this page.
What Acute Otitis Media Is
Most childhood earaches are acute otitis media (AOM) — an infection of the middle ear, the small air-filled space that sits behind the eardrum (tympanic membrane) and connects to the back of the nose through the Eustachian tube. AOM typically follows a cold: the virus inflames the lining of the Eustachian tube, the tube stops draining and ventilating properly, fluid accumulates in the middle ear, and bacteria or viruses multiply in that trapped fluid. The result is pressure, a red bulging eardrum, and the sharp, often nighttime pain that sends families to urgent care.
AOM is extraordinarily common in young children, largely because their Eustachian tubes are short, narrow, and nearly horizontal, so they drain poorly. The great majority of episodes resolve on their own. Because of this, modern pediatric guidelines (the American Academy of Pediatrics 2013 AOM guideline) endorse "watchful waiting" with adequate pain control for many children over six months of age with non-severe symptoms, reserving immediate antibiotics for younger infants, severe presentations, or both ears. That guideline shift is the reason a safe, effective pain remedy — herbal or pharmaceutical — is clinically valuable: pain relief is often the actual goal, not sterilizing the ear.
It is essential to distinguish AOM (infection and fluid behind an intact eardrum) from two other things people loosely call "an ear infection." Otitis externa (swimmer's ear) is an infection of the outer ear canal itself. A perforated or draining ear means the eardrum has ruptured and pus is escaping — or there is a tube in place. The crucial point for this page: mullein ear oil drops are placed into the ear canal. With an intact eardrum the oil warms and soothes the canal and outer membrane but cannot reach the middle ear. With a perforated eardrum, anything dripped into the canal can pass straight through into the middle ear — which is exactly why drainage or a known perforation is an absolute stop.
The Sarrell Clinical Trials — Otikon Herbal Ear Drops
The strongest clinical evidence for herbal ear drops comes from two randomized trials led by Ephraim Sarrell and colleagues in Israel, both published in mainstream pediatric journals. They tested a standardized herbal ear-drop product called Otikon, an olive-oil extract combining Allium sativum (garlic), Verbascum thapsus (mullein), Calendula flores (calendula), and Hypericum perforatum (St John's wort). Mullein is one of the four botanicals in the formula, so the trials are best read as evidence for a mullein-containing blend rather than for mullein in isolation.
The first study (Sarrell, Mandelberg & Cohen, Archives of Pediatrics & Adolescent Medicine, 2001) enrolled children aged 6–18 years with ear pain associated with AOM and compared the Otikon naturopathic drops against an anesthetic ear-drop preparation (ametocaine/amethocaine plus phenazone in glycerin). Over the course of treatment, ear pain decreased significantly in both groups, and the herbal extract was statistically comparable to the anesthetic drops for relieving pain — an important result, because it suggested a plant-oil drop could match a conventional topical analgesic for the symptom that matters most to a child at 2 a.m.
The second, larger study (Sarrell, Cohen & Kahan, Pediatrics, 2003) randomized 171 children into a 2×2 design that crossed the ear drops (herbal extract vs anesthetic) with the management approach (drops alone vs drops plus oral antibiotics). The herbal drops again produced clinically meaningful pain reduction, and — notably — adding antibiotics did not improve pain control beyond the topical drops. This dovetails with the watchful-waiting philosophy: for the pain of uncomplicated AOM, a well-formulated topical drop performed as well as the alternatives the trial tested.
These are the citations to anchor any claim about mullein ear drops. Their limits are equally important and are discussed in the pediatric-evidence section below: the active comparator was a topical anesthetic rather than placebo, the product was a four-herb blend, and the children all had intact eardrums by design.
How to Make and Use Mullein Ear Oil
A traditional mullein ear oil is a simple flower-in-oil infusion. The flowers are the part used — the small, bright-yellow blossoms picked from the tall flowering spike, ideally dried or wilted first so that residual water does not spoil the oil. The classic methods are:
- Slow (solar) infusion — pack a clean dry jar loosely with dried mullein flowers, cover completely with a stable carrier oil (olive oil is traditional), cap, and leave in a warm spot out of direct harsh sun for 2–4 weeks, shaking daily. Strain thoroughly through cheesecloth so no plant fragments remain.
- Gentle heat infusion — warm the flowers and oil together in a double boiler or low oven (kept well below a simmer, roughly 100–110°F / 38–43°C) for several hours, then strain. Faster, but excess heat degrades the delicate constituents, so keep it low.
To use a finished, strained oil for an intact-eardrum earache: warm the dropper bottle to body temperature first — the easiest way is to stand it in a cup of warm (not hot) water for a few minutes, then test a drop on the inside of your wrist. Cold oil in the ear can trigger dizziness because it stimulates the balance organs. Have the person lie with the sore ear facing up, gently drip in a few drops, then have them rest in that position for several minutes (a loose cotton ball at the canal opening keeps the oil from running out). A typical folk regimen is a few drops two to four times a day for a day or two while symptoms settle.
Practical cautions for the preparation itself: use only well-dried flowers and a clean, dry jar, because water left in the oil invites mold and rancidity; discard any oil that smells off; and buy from a reputable maker if you are not confident infusing your own. Commercial products are convenient and consistently strained, which matters for the ear. None of this changes the absolute rule in the next section — warm, well-made oil is still only appropriate when the eardrum is intact and not draining.
Why It May Soothe the Ear
Several plausible, overlapping mechanisms explain why a warm mullein-oil drop can ease ear pain, and it is honest to say that the relative contribution of each is not fully pinned down by research.
First, and probably most underrated, is warmth itself. Applying gentle heat to the ear is a time-tested comfort measure, and a body-temperature oil delivers a small, sustained warm compress directly to the inflamed canal and outer eardrum. In the Sarrell trials the anesthetic comparator drops were also oil/glycerin-based and warmed, so part of the benefit in both arms likely came from the vehicle and the warmth, not solely from any pharmacology. The oil also forms an occlusive, lubricating film that may blunt the irritation of an inflamed canal.
Second, mullein flowers carry anti-inflammatory and demulcent constituents. Verbascum thapsus contains flavonoids (such as verbascoside/acteoside and luteolin derivatives), iridoid glycosides including aucubin, mucilage, and saponins. Pharmacological reviews of the genus (for example Turker & Gurel's monograph and a more recent Verbascum thapsus review) describe anti-inflammatory and antioxidant activity for these compounds in laboratory models, consistent with the plant's traditional role in calming irritated mucous membranes.
Third, several of the botanicals traditionally paired with mullein in ear oils — most notably garlic — have measurable antimicrobial activity in vitro. This is the most over-claimed mechanism, because a few drops in an intact ear canal cannot reach bacteria sitting behind the eardrum; any antimicrobial effect is confined to the canal surface. The realistic picture is that warmth plus anti-inflammatory plant oils provide comfort while the immune system clears the actual middle-ear infection, rather than the oil "curing" the infection directly.
Critical Safety — When You Must Not Use Ear Oil
This is the most important section on the page. Read it before you use any ear oil, herbal or otherwise.
- Never put oil drops in an ear with a perforated or ruptured eardrum. If the eardrum has a hole, anything dripped into the canal can pass directly into the middle ear, where it does not belong and can cause harm. A known perforation is an absolute contraindication.
- Never use ear drops if there is drainage coming from the ear. Fluid, pus, or blood draining out of the canal is a red flag that the eardrum has already ruptured (or that there is another serious problem). Stop and see a clinician — do not put anything in the ear.
- Do not use ear oil if a tympanostomy (ear) tube is in place, for the same reason — the tube is an open channel into the middle ear.
- See a clinician promptly for severe or rapidly worsening ear pain, a high fever, swelling or redness of the bone behind the ear, facial weakness, a stiff neck, sudden hearing loss or marked dizziness, or any earache in an infant under about six months.
- Do not let symptoms run beyond 48–72 hours. If the pain has not clearly improved within two to three days, or it improves and then sharply worsens, get the ear examined. An untreated bacterial AOM occasionally progresses to complications, and only a clinician with an otoscope can confirm the eardrum is intact and the diagnosis is right.
The reason a clinician's examination matters so much is that you cannot see your own eardrum. The Sarrell trials specifically enrolled children whose eardrums had been examined and found intact; that examination is the safety gate the home user is missing. When in doubt, the safe default is to control pain with measures that do not require an intact eardrum (oral acetaminophen or ibuprofen at appropriate doses, a warm external compress) and to have the ear looked at.
Combining Mullein with Garlic
The most common commercial earache oil pairs mullein flowers with garlic (Allium sativum), and the Otikon formula in the Sarrell trials included both. The rationale is complementary: mullein contributes the soothing, anti-inflammatory, demulcent character, while garlic contributes the antimicrobial reputation. Garlic's signature compound, allicin, is generated when raw garlic is crushed (the enzyme alliinase converts alliin to allicin) and has well-documented antibacterial and antifungal activity in laboratory testing.
Two honest caveats temper the garlic story. First, allicin is unstable and is not efficiently extracted into, or preserved in, a warm oil — so the allicin content of a homemade garlic oil is variable and often low. Second, as stressed above, any antimicrobial action is limited to the ear-canal surface and cannot reach a middle-ear infection through an intact eardrum. The practical takeaway is that the garlic–mullein pairing is a reasonable, traditional comfort blend with a supportive (if blended) clinical trial behind it — not a documented stand-alone cure for AOM.
A separate, serious safety note applies to garlic oil specifically: garlic infused in oil is a botulism risk if stored improperly. Clostridium botulinum spores from soil on the garlic can germinate and produce toxin in the low-oxygen, low-acid environment of oil held at room temperature. This is well documented for culinary garlic-in-oil and is the reason such oils must be refrigerated and used quickly or made fresh. For more on garlic's chemistry and uses, see the Garlic page.
Pediatric Considerations and the Limits of the Evidence
Children are the population most affected by earache and the population in which mullein ear oil is most often used, so the evidence's limits deserve a careful, honest read.
The Sarrell trials are genuinely encouraging, but they were designed in a way that constrains the conclusions. The comparator was an active topical anesthetic, not a placebo, so the trials show the herbal drops were not inferior to a conventional analgesic — they do not isolate how much of the relief came from the herbs versus from the warmed oil vehicle and the natural, rapid resolution of most AOM pain. The intervention was a four-herb blend in olive oil, so the design cannot tell you how much mullein specifically contributed. And the enrolled children were 6–18 years old (first trial) with confirmed intact eardrums, which does not directly establish safety or efficacy in infants and toddlers, the group most prone to AOM and least able to report a worsening course.
Pediatric practicalities follow from this. Any earache in an infant under roughly six months warrants prompt medical evaluation rather than home oil. For older children with a non-severe earache and an eardrum a clinician has confirmed is intact, warmed herbal ear oil is a reasonable comfort measure alongside — not instead of — appropriate oral analgesia and the watchful-waiting plan the clinician advises. Parents should be coached on the same red flags listed in the safety section, and reminded that persistent or worsening symptoms past 48–72 hours need a re-examination. Mullein ear oil is an adjunct for comfort, not a substitute for diagnosis.
Evidence Summary
Pulling the threads together:
- What is well supported: A mullein-containing herbal ear drop (Otikon: garlic, mullein, calendula, St John's wort in olive oil) relieved the pain of acute otitis media about as well as a conventional anesthetic ear drop in two randomized pediatric trials, and adding oral antibiotics did not improve pain control beyond the drops.
- What is plausible but not proven for mullein alone: The anti-inflammatory and demulcent constituents of Verbascum thapsus flowers likely contribute to the soothing effect, but the trials used a blend, so mullein's isolated contribution is not quantified.
- What is over-claimed: The idea that drops "cure" a middle-ear infection. With an intact eardrum, drops cannot reach the middle ear; the realistic role is symptomatic comfort (warmth, lubrication, anti-inflammatory action) while the infection resolves on its own.
- The non-negotiable boundary: No oil in a perforated, draining, or tube-fitted ear; medical evaluation for severe, infant, or persistent cases.
In short, mullein ear oil — ideally as part of a traditional warmed garlic–mullein blend — is a reasonable, low-risk comfort measure for the pain of an uncomplicated, intact-eardrum earache, used within the safety boundaries above and alongside proper diagnosis. It is one of the better-studied topical herbal remedies precisely because two real randomized trials put a mullein-containing product head-to-head with a pharmaceutical comparator.
Cautions
- Intact eardrum only. Use ear oil only when a clinician has confirmed the eardrum is not perforated. Stop immediately for any drainage from the ear.
- Get the diagnosis right. Severe pain, high fever, swelling behind the ear, facial weakness, stiff neck, sudden hearing loss, marked dizziness, or any earache in a young infant requires prompt medical care, not home oil.
- Honor the time limit. If symptoms do not clearly improve within 48–72 hours, or worsen after improving, have the ear re-examined.
- Botulism risk with garlic oil. Refrigerate garlic-infused oils, use them quickly, and never store homemade garlic oil at room temperature.
- Preparation hygiene. Use thoroughly dried flowers and clean, dry jars; strain completely; discard oil that smells rancid or shows any sign of mold.
- Allergy and irritation. Mullein's fine plant hairs can irritate; the strained oil avoids this, but discontinue if the ear canal becomes itchy, swollen, or more painful after use.
- St John's wort component. Topical St John's wort (in blends like Otikon) can increase skin photosensitivity; this is a minor concern for an in-ear drop but worth noting for anyone using the same product on skin.
- Not a substitute for antibiotics when truly indicated. Infants, severe or bilateral AOM, and immunocompromised patients may need antibiotics; ear oil does not replace them.
Research Papers and References
The references below anchor the clinical claims on this page. The two Sarrell trials and the Verbascum reviews are linked to their PubMed/DOI records; broader topics open as curated PubMed searches at the National Library of Medicine.
- Sarrell EM, Mandelberg A, Cohen HA (2001). Efficacy of naturopathic extracts in the management of ear pain associated with acute otitis media. Archives of Pediatrics & Adolescent Medicine; 155(7):796–799. — PubMed 11434846
- Sarrell EM, Cohen HA, Kahan E (2003). Naturopathic treatment for ear pain in children. Pediatrics; 111(5):e574–e579. — Search PubMed
- Turker AU, Gurel E (2005). Common mullein (Verbascum thapsus L.): recent advances in research. Phytotherapy Research; 19(9):733–739. — doi:10.1002/ptr.1653
- Review of Verbascum thapsus (common mullein) phytochemistry and pharmacology. Phytotherapy Research. — doi:10.1002/ptr.7393
- Lieberthal AS et al. (2013). The diagnosis and management of acute otitis media (AAP clinical practice guideline). Pediatrics. PubMed search
- Watchful waiting and pain management in acute otitis media. PubMed search
- Topical herbal and analgesic ear drops for otitis media pain. PubMed search
- Verbascum thapsus anti-inflammatory and antioxidant constituents (verbascoside, aucubin, luteolin). PubMed search
- Allium sativum (garlic) allicin antimicrobial activity. PubMed search
- Garlic-in-oil and the risk of Clostridium botulinum toxin formation. PubMed search
- Tympanic membrane perforation and contraindications to ototopical preparations. PubMed search
External Resources
- NCCIH — Herbs at a Glance
- MedlinePlus — Herbs and Supplements
- PubMed — All research on Verbascum thapsus
Connections
- All Herbs
- Mullein Hub
- Mullein: Antibacterial & Antimicrobial Action
- Mullein: Skin, Wounds & Inflammation
- Mullein: Forms, Dosage & Safety
- Mullein: History & Traditional Use
- Garlic
- Echinacea