Relapsing Polychondritis
- Overview
- Epidemiology
- Pathophysiology
- Auricular Chondritis
- Airway Involvement
- Other Systemic Features
- Associated Conditions and VEXAS
- Diagnosis
- Treatment
- Prognosis and Monitoring
- References
- Connections
Overview
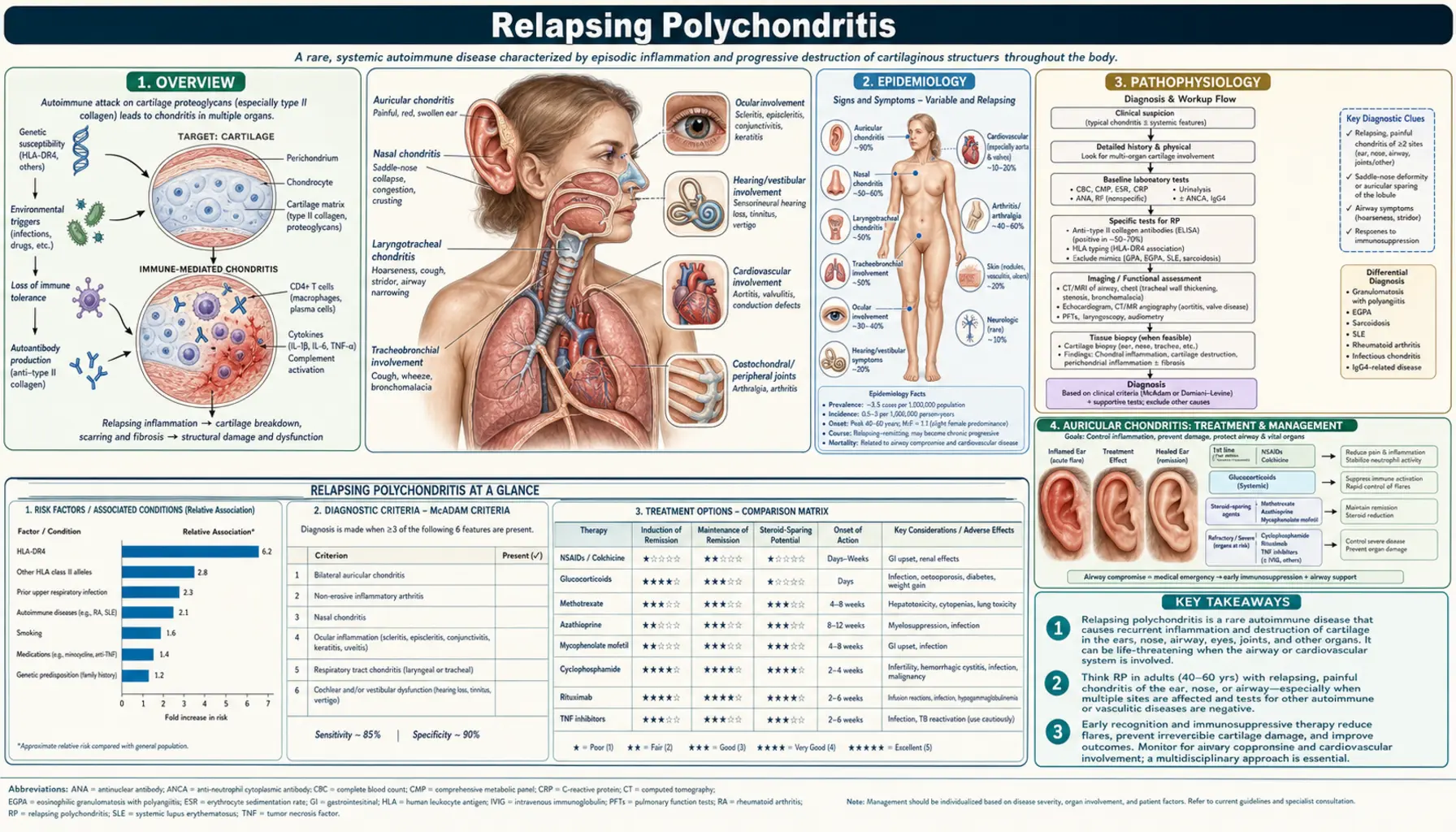
Relapsing polychondritis (RP) is a rare, episodic autoimmune disease characterized by recurrent inflammation of cartilaginous structures and other proteoglycan-rich tissues throughout the body. The targets are anatomically diverse: the ears, nose, larynx, trachea, bronchi, joints, eyes, and cardiovascular structures are all vulnerable. Unlike most autoimmune connective tissue diseases, RP does not fit neatly into the seropositive or seronegative categories — rheumatoid factor and antinuclear antibodies are typically absent, and no single confirmatory laboratory test exists. The diagnosis rests on clinical recognition of the characteristic pattern of recurrent chondritis.
The hallmark feature — and the finding most likely to prompt diagnosis — is painful, erythematous swelling of the outer ear that sharply spares the earlobe. Because the earlobe contains only fat and fibrous tissue (no cartilage), it remains soft and uninflamed even as the surrounding auricular cartilage is intensely inflamed. This earlobe-sparing auricular chondritis is considered pathognomonic in the correct clinical context. Repeated attacks of auricular inflammation eventually destroy the cartilage, causing the ear to collapse into the "cauliflower ear" deformity familiar from contact sports — but arising here from autoimmune destruction rather than trauma.
The most feared complication is progressive destruction of the tracheal and bronchial cartilage skeleton, producing tracheobronchomalacia: the dynamic collapse of the central airways during respiration. This can evolve into life-threatening respiratory failure and is the leading cause of death in RP. The rarity of the condition, its episodic course, and the non-specificity of early symptoms frequently lead to diagnostic delays of months to years — during which irreversible airway damage may accumulate silently.
Epidemiology
Relapsing polychondritis is rare, with an estimated incidence of approximately 3.5 cases per million population per year. It affects all racial groups, both sexes, and a wide age range, but the peak onset is in the fourth and fifth decades of life (ages 40–60 years). Unlike many autoimmune diseases with a strong female predominance, RP shows a roughly equal sex distribution in most large cohort studies, with some series reporting a slight female excess. There is no established geographic or ethnic clustering in the general RP population.
A critical epidemiological observation is the high rate of associated conditions — approximately 30% of RP patients carry a concurrent systemic disease, and this proportion is even higher in specific subgroups. Myelodysplastic syndrome (MDS) occurs in 20–30% of RP cases, a rate far exceeding what would be expected by chance. Other associated conditions include rheumatoid arthritis, systemic lupus erythematosus, Sjögren's syndrome, ankylosing spondylitis, and ANCA-associated vasculitis. The 2020 discovery of VEXAS syndrome — caused by somatic UBA1 mutations in hematopoietic stem cells — has redefined a substantial subset of RP patients who are male, older, treatment-refractory, and carry concurrent MDS or other hematologic diagnoses.
Pathophysiology
The pathogenesis of RP centers on immune-mediated destruction of cartilage matrix proteoglycans, particularly type II collagen, matrilin-1, and cartilage oligomeric matrix protein (COMP). Both cellular and humoral immune mechanisms are implicated. Autoantibodies against type II collagen are detectable in approximately 30% of RP patients and tend to be highest during active flares; they are not reliably present in all patients and their pathogenic role remains incompletely defined. T-cell-mediated cartilage destruction is supported by the observation that CD4+ T helper cells and CD8+ cytotoxic T cells are prominent in chondritis biopsy specimens, and by animal models in which immunization with type II collagen induces RP-like inflammation.
Histologically, active chondritis shows loss of basophilic staining of the cartilage matrix (reflecting proteoglycan depletion), perichondrial mononuclear cell infiltration (lymphocytes and plasma cells), and chondrolysis — the dissolution of the cartilage itself. As attacks recur, fibrous tissue replaces destroyed cartilage; this fibrous replacement lacks the mechanical resilience of cartilage and ultimately leads to structural collapse. The predilection for certain cartilage sites (ears, nose, trachea) over others (hyaline articular cartilage of weight-bearing joints) remains unexplained but may reflect differences in collagen type distribution, vascular supply, or mechanical stress patterns that modulate local immune activation.
The newly defined VEXAS syndrome (Vacuoles, E1 enzyme UBA1, X-linked, Autoinflammatory, Somatic) provides an important mechanistic window. Somatic mutations in UBA1 — the gene encoding the primary E1 ubiquitin-activating enzyme — accumulate in hematopoietic precursor cells, impairing the ubiquitin-proteasome pathway and triggering innate immune activation. These mutant hematopoietic cells differentiate into monocytes and neutrophils with constitutively enhanced inflammatory signaling. The UBA1 mutation is X-linked and, being somatic rather than germline, occurs almost exclusively in post-reproductive males. VEXAS patients present with an RP-like phenotype — auricular chondritis, nasal chondritis, and airway inflammation — but with treatment-refractory systemic inflammation, concurrent MDS or other cytopenias, and a distinctly poor prognosis compared to classic RP.
Auricular Chondritis
Auricular chondritis — inflammation of the cartilaginous framework of the outer ear — is the most common and most diagnostically important manifestation of RP, occurring in approximately 85% of patients over the course of their disease and as the presenting feature in roughly 40%. Its clinical presentation is distinctive: the pinna becomes acutely painful, erythematous, warm, and swollen during a flare. The demarcation at the earlobe is the key diagnostic sign: the lobe, which contains no cartilage, remains soft, non-tender, and uninflamed — a sharp line separates the inflamed upper and outer ear from the normal lobe. This earlobe-sparing pattern distinguishes RP from infectious perichondritis (which does not spare the lobe), from contact dermatitis, and from other causes of ear erythema.
Acute auricular flares typically last days to weeks, then partially or completely resolve between episodes. With each recurrence, incremental cartilage destruction accumulates. Early in the disease the ear returns to near-normal appearance between flares; in advanced or frequently relapsing disease, cartilage loss becomes permanent. The pinna progressively softens and loses its structural rigidity, eventually collapsing into the cauliflower ear deformity — a floppy, structurally unsupported ear that retains none of the original contours. This deformity is cosmetically distressing but also serves as an important disease marker: its presence strongly suggests significant cumulative cartilage damage and implies that other cartilaginous structures (nose, airway) have likely sustained parallel damage even if clinically less apparent.
Cochlear and vestibular involvement affects approximately 30% of RP patients through vasculitis of the internal auditory artery and local inflammation. Sensorineural hearing loss (SNHL) may develop suddenly or gradually and tends to be the most treatment-resistant audiovestibular manifestation. Vestibular dysfunction produces episodic vertigo and ataxia, sometimes resembling Ménière's disease clinically. Conductive hearing loss from external auditory canal collapse (cartilage destruction narrowing the canal) or eustachian tube dysfunction can coexist with SNHL. Any new hearing impairment or vertigo in an RP patient warrants audiometric evaluation and consideration of increased immunosuppression.
Airway Involvement
Laryngotracheal and bronchial involvement — present in approximately 50% of RP patients over the disease course — represents the most dangerous manifestation and the leading cause of RP-related mortality. Laryngeal chondritis produces hoarseness, voice changes, dysphonia, and tenderness over the thyroid cartilage. Subglottic stenosis from scarring after repeated laryngeal flares can cause fixed inspiratory stridor — a high-pitched, harsh, monophonic breath sound on inspiration that marks critical upper airway narrowing.
Tracheal and bronchial cartilage destruction produces tracheobronchomalacia (TBM): the loss of structural rigidity of the central airway walls. In normal physiology, the tracheal cartilage rings provide circumferential support that prevents airway collapse during the pressure fluctuations of normal breathing. When these rings are destroyed by recurrent chondritis, the airway walls become flaccid and dynamic obstruction occurs: the trachea and proximal bronchi collapse during expiration (when intrathoracic pressure exceeds airway lumen pressure) and are compressed from outside during inspiration. Patients experience exertional dyspnea that progresses to dyspnea at rest, ineffective cough (inability to generate sufficient expiratory flow through a collapsing airway to clear secretions), recurrent lower respiratory infections from poor mucous clearance, and eventually respiratory failure.
Pulmonary function testing in TBM classically shows a saw-tooth pattern on the flow-volume loop and a disproportionate reduction in expiratory flow at mid-lung volumes. CT of the chest and airway — particularly dynamic (inspiratory/expiratory) chest CT — is the most informative imaging modality: it demonstrates thickening and enhancement of the tracheal wall during active chondritis, and on expiratory imaging shows the diagnostic "frown sign" or greater than 50% reduction in tracheal cross-sectional area during forced expiration in TBM. Bronchoscopy directly visualizes the mucosal changes and dynamic collapse. Management of severe TBM may require airway stenting with self-expanding metallic or silicone stents, tracheostomy, or continuous positive airway pressure (CPAP) to pneumatically splint the airway open. Systemic immunosuppression can arrest active chondritis but cannot reverse established fibrotic scarring and structural collapse.
Other Systemic Features
Nasal chondritis occurs in approximately 60% of patients. Recurrent inflammation of the nasal septal cartilage produces rhinorrhea, nasal congestion, and bridge tenderness. Progressive destruction of the nasal dorsal cartilage leads to the saddle nose deformity — collapse of the nasal bridge producing a characteristic depressed, widened nose. This same deformity occurs in granulomatosis with polyangiitis (GPA/Wegener's), tertiary syphilis, and congenital syphilis; in RP, the saddle nose is mechanistically identical but serological, ANCA, and infectious context differentiate these conditions. Once the saddle nose has developed, it is permanent — the destroyed cartilage does not regenerate.
Articular involvement occurs in 50–70% of patients and is characteristically non-deforming and seronegative. The arthritis is typically migratory or oligoarticular, involving large joints (knees, ankles, wrists) and small joints without symmetry. Importantly, it does not cause erosive joint destruction — a point that helps distinguish RP arthritis from rheumatoid arthritis in a patient who has both conditions. Costochondral junction tenderness (costochondritis) is a specific pattern pointing toward RP when present alongside other chondritis features; it represents inflammation at the cartilaginous rib-sternal junction.
Ocular involvement occurs in approximately 50–65% of patients over the disease course. Episcleritis — inflammation of the episcleral tissue, producing sectoral or diffuse redness without visual impairment — is the most common ocular manifestation and tends to mirror systemic disease activity. Scleritis is more severe, painful, and potentially vision-threatening; nodular or posterior scleritis can produce significant ocular morbidity. Uveitis (anterior iritis) produces photophobia, pain, and ciliary flush; untreated recurrent uveitis risks posterior synechiae, glaucoma, and cataracts. Proptosis from orbital pseudotumor and keratitis are less common but recognized manifestations.
Cardiovascular involvement affects approximately 25% of patients. Aortitis — inflammation of the aortic wall — produces aortic regurgitation (from aortic root dilatation), aortic aneurysm (thoracic more often than abdominal), and in severe cases aortic dissection. Mitral valve regurgitation from mitral annular inflammation is less common. Conduction system disease (heart block, bundle branch block) from inflammation of the conducting tissue is recognized. Aortic root involvement in RP is mechanistically analogous to the large-vessel vasculitis seen in GCA and Takayasu's, reflecting the shared proteoglycan content of vascular walls and cartilage. Regular echocardiographic surveillance is warranted for all RP patients because cardiovascular complications can be clinically silent until hemodynamically significant.
Associated Conditions and VEXAS Syndrome
Myelodysplastic syndrome (MDS) is present in 20–30% of RP patients — a dramatically elevated rate compared to the general population (age-adjusted incidence of MDS is roughly 4 per 100,000 per year). This association is not coincidental: MDS and RP share dysregulated innate immune signaling as a common upstream driver, and bone marrow examination is appropriate in any RP patient with unexplained cytopenias, macrocytosis, or an atypical disease course. Conversely, rheumatologists evaluating RP should send a complete blood count at diagnosis and follow it longitudinally; new cytopenias may herald MDS or its transformation to acute myeloid leukemia.
VEXAS syndrome, first described in 2020 by Beck and colleagues in the New England Journal of Medicine, has redefined understanding of the RP-MDS overlap. VEXAS arises from somatic mutations in UBA1 — the master E1 ubiquitin-activating enzyme — in hematopoietic stem cells. Because UBA1 is X-linked and the mutations are somatic (arising post-zygotically in the bone marrow), VEXAS occurs almost exclusively in males over age 50. The resulting impairment in ubiquitin-mediated protein quality control activates innate inflammatory pathways constitutively, producing a phenotype overlapping RP, MDS, Sweet's syndrome, and systemic vasculitis. Critical distinguishing features of VEXAS include: older male patients, treatment-refractory inflammation despite high-dose corticosteroids and multiple immunosuppressants, prominent MDS features (anemia, thrombocytopenia), cutaneous neutrophilic dermatosis, and frequent constitutional symptoms. Bone marrow biopsy in VEXAS shows vacuolated erythroid and myeloid precursors — the "V" in VEXAS. Genetic testing for UBA1 mutations (VAF ≥10% in blood or bone marrow) confirms the diagnosis. Treatment of VEXAS remains challenging; ruxolitinib (JAK1/2 inhibitor), azacitidine, and allogeneic hematopoietic stem cell transplantation are being investigated.
Other autoimmune associations in RP include rheumatoid arthritis (coexistent RA occurs in approximately 20% of RP cohorts), systemic lupus erythematosus, Sjögren's syndrome, ANCA-associated vasculitis, and inflammatory bowel disease. When RP overlaps with another systemic autoimmune disease, clinical management becomes significantly more complex because disease activity in one condition may be difficult to distinguish from flares of the other, and treatment regimens must address both.
Diagnosis
There is no pathognomonic laboratory test for RP. The diagnosis is clinical, supported by histopathology when biopsy is feasible and informative. The most widely cited diagnostic framework is the McAdam criteria (1976), which require at least three of the following six features: (1) recurrent bilateral auricular chondritis; (2) non-erosive seronegative inflammatory polyarthritis; (3) nasal chondritis; (4) ocular inflammation (conjunctivitis, keratitis, scleritis/episcleritis, uveitis); (5) respiratory tract chondritis (laryngeal or tracheal cartilage involvement); (6) cochlear or vestibular dysfunction. Damiani and Levine subsequently modified the criteria to allow diagnosis with one of the above plus positive biopsy, or two of the above with a response to dapsone or corticosteroids.
Biopsy of the auricular cartilage or nasal cartilage during an active flare can confirm the diagnosis histologically: loss of basophilic matrix staining, perichondrial inflammatory infiltrate (lymphocytes, plasma cells, neutrophils), and chondrolysis are characteristic. However, biopsy is not required for diagnosis when the clinical presentation is sufficiently characteristic (e.g., bilateral earlobe-sparing auricular chondritis in the appropriate context). CT chest and dynamic CT airway are essential for baseline assessment and follow-up of tracheal and bronchial disease. Pulmonary function testing with flow-volume loops, echocardiography, audiometry, and ophthalmological examination are recommended as part of initial evaluation to establish baseline organ involvement.
Laboratory evaluation reveals elevated inflammatory markers (ESR, CRP) during active flares; these normalize in remission and can track disease activity longitudinally. Complete blood count should be assessed for cytopenias suggesting MDS. Complement levels (C3, C4), immunoglobulins, and urinalysis are useful to exclude overlap syndromes. Anti-type II collagen antibodies are present in approximately 30% of patients but are not commercially available at all centers and are not required for diagnosis. In older males with refractory RP and concurrent cytopenias, UBA1 mutation testing should be performed.
Treatment
Treatment is individualized based on disease severity, organ involvement, and pace of progression. Mild episodic disease (isolated auricular or nasal chondritis without airway, ocular, or cardiovascular involvement) may be manageable with nonsteroidal anti-inflammatory drugs (NSAIDs) or dapsone. Dapsone, at doses of 25–200 mg daily, has demonstrated efficacy in reducing the frequency and severity of chondritis flares in observational studies and case series; its mechanism in RP is incompletely understood but likely involves inhibition of neutrophil function and tissue adhesion.
Corticosteroids are the cornerstone of treatment for moderate-to-severe disease, active airway inflammation, and organ-threatening manifestations. Prednisone doses of 0.5–1 mg/kg/day are typical for acute severe flares, with gradual tapering as the flare resolves. Prolonged steroid dependence — which is common in RP given its episodic, relapsing nature — requires the addition of steroid-sparing immunosuppressants. Methotrexate (15–25 mg weekly), azathioprine (2 mg/kg/day), and mycophenolate mofetil are used as maintenance agents; none has been evaluated in randomized controlled trials given the rarity of the disease, but observational data support modest efficacy for arthritis and systemic inflammation.
Biologic therapies have become increasingly important, particularly for refractory or rapidly progressive disease. TNF inhibitors (infliximab, adalimumab, etanercept) have shown benefit in case series and small retrospective cohorts, particularly for joint and systemic inflammation. IL-6 inhibition (tocilizumab) is used for patients with prominent systemic inflammatory features. Abatacept (CTLA4-Ig, T-cell costimulation blockade) has shown promise in case reports. JAK inhibitors (tofacitinib, baricitinib) are increasingly used, particularly in the context of VEXAS where ruxolitinib is under investigation. Anti-CD20 therapy (rituximab) is employed in overlap syndromes and refractory disease. The absence of randomized trial data means that biologic selection in RP is largely empiric and guided by the dominant manifestation and associated comorbidities.
Airway complications require multidisciplinary management with pulmonology and thoracic surgery. Active airway chondritis with evidence of tracheal wall thickening is treated with intensified systemic immunosuppression to prevent progression to TBM. Established TBM with airway collapse is managed with airway stenting, CPAP, or in severe cases tracheostomy. Patients with progressive hearing loss require audiological support and hearing aids; cochlear implantation has been performed successfully in RP patients with profound SNHL. Aortic root disease and valvular complications require cardiology co-management and, when severe, cardiac surgery.
Prognosis and Monitoring
The course of RP is highly variable. Some patients experience mild episodic disease with long remissions and no life-threatening organ involvement; others have relentlessly progressive disease with early airway and cardiovascular complications. A 1998 analysis found 5-year and 10-year survival rates of approximately 74% and 55% respectively in cohorts assembled before modern biologics; more recent series suggest improved outcomes with earlier diagnosis and aggressive immunosuppression, though precise contemporary mortality data are limited by disease rarity. The leading causes of death are respiratory failure from airway disease, cardiovascular complications (aortic aneurysm, valvular disease), and infections related to chronic immunosuppression. MDS-associated RP carries a worse prognosis, driven by the natural history of the underlying hematologic disease.
Monitoring should be systematic given the wide and unpredictable spectrum of organ involvement. Clinical assessment at each visit should include targeted review of auricular, nasal, airway, ocular, joint, and cardiovascular symptoms. Annual pulmonary function testing and periodic dynamic CT airway imaging track tracheal disease; frequency is guided by baseline findings and symptoms. Serial echocardiography (annually or biannually in patients with any baseline aortic root abnormality) monitors for progressive aortic dilatation. Complete blood count monitoring is essential to detect evolving MDS. Inflammatory markers (CRP, ESR) serve as adjunct disease activity measures. Patient education about the significance of new dyspnea, stridor, or voice change — symptoms requiring immediate medical evaluation — is a critical component of long-term management.
References
- Mathian A, Miyara M, Cohen-Aubart F, et al. Relapsing polychondritis: a 2016 update on clinical features, diagnostic tools, treatment and biological drug use. Best Pract Res Clin Rheumatol. 2016;30(2):316–333 — Search PubMed
- Dion J, Costedoat-Chalumeau N, Sène D, et al. Relapsing polychondritis can be characterized by three distinct clinical phenotypes: analysis of a recent series of 142 patients. Arthritis Rheumatol. 2016;68(12):2992–3001 — Search PubMed
- Beck DB, Ferrada MA, Sikora KA, et al. Somatic mutations in UBA1 and severe adult-onset autoinflammatory disease. N Engl J Med. 2020;383(27):2628–2638. PMID: 33108101
- McAdam LP, O'Hanlan MA, Bluestone R, Pearson CM. Relapsing polychondritis: prospective study of 23 patients and a review of the literature. Medicine (Baltimore). 1976;55(3):193–215 — Search PubMed
- Ferrada MA, Grayson PC, Banerjee S, et al. Patient perception of disease-related symptoms and complications in relapsing polychondritis. Arthritis Care Res (Hoboken). 2018;70(8):1124–1131 — Search PubMed
- Trentham DE, Le CH. Relapsing polychondritis. Ann Intern Med. 1998;129(2):114–122. PMID: 9669970
- Sato M, Sugimoto K, Nakamura M, et al. Tracheobronchial involvement in relapsing polychondritis: clinical and radiological findings. Intern Med. 2018;57(24):3605–3609 — Search PubMed
- Shimizu J, Yamano Y, Kawahata K, et al. Biologic therapies for relapsing polychondritis: an analysis of BIORA (biologics for refractory disease in autoimmune conditions). Rheumatol Int. 2021;41(8):1529–1538 — Search PubMed
- Letko E, Zafirakis P, Baltatzis S, Voudouri A, Livir-Rallatos C, Foster CS. Relapsing polychondritis: a clinical review. Semin Arthritis Rheum. 2002;31(6):384–395 — Search PubMed
- Ferrada MA, Sikora KA, Luo Y, et al. Somatic mutations in UBA1 define a distinct subset of relapsing polychondritis patients with hematologic conditions. Arthritis Rheumatol. 2021;73(10):1836–1844 — Search PubMed
- Arnaud L, Mathian A, Haroche J, Gorochov G, Amoura Z. Pathogenesis of relapsing polychondritis: a 2013 update. Autoimmun Rev. 2014;13(2):90–95 — Search PubMed
- Valenzuela R, Cooperrider PA, Gogate P, Deodhar SD, Bergfeld WF. Relapsing polychondritis: immunomicroscopic findings in cartilage of ear biopsy specimens. Hum Pathol. 1980;11(1):19–22 — Search PubMed
Connections
- Rheumatology
- Vasculitis
- IgG4-Related Disease
- Ankylosing Spondylitis
- Rheumatoid Arthritis
- Psoriatic Arthritis
- Systemic Sclerosis
- Polyarteritis Nodosa
- Giant Cell Arteritis
- Reactive Arthritis
- Adult-Onset Still's Disease
- Lab Tests