Preterm Labor
Table of Contents
- Overview and Definition
- Risk Factors
- Diagnosis: The Tricky Part
- Tocolysis: Stopping Contractions
- Antenatal Corticosteroids
- Magnesium for Fetal Brain Protection
- Progesterone for Prevention
- Cervical Cerclage
- What Parents Should Know: NICU
- Signs That Need Immediate Evaluation
- Key Research Papers
- Connections
- Featured Videos
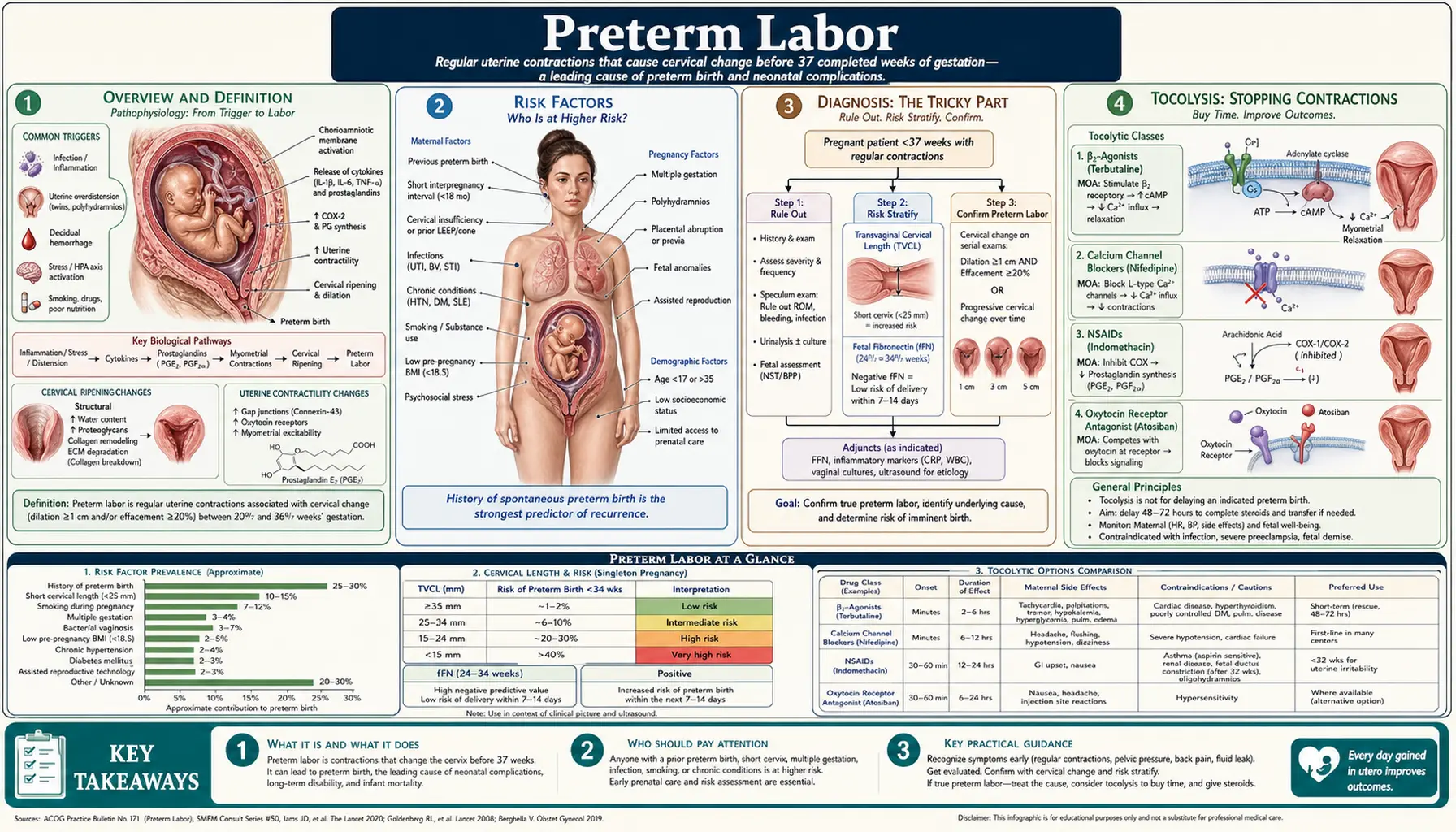
Overview and Definition
Preterm labor is defined as regular uterine contractions — at least 4 in 20 minutes or at least 8 in one hour — accompanied by cervical change (dilation, effacement, or both) before 37 completed weeks of pregnancy. It is the most common cause of neonatal illness and death in the United States, and the US has one of the highest preterm birth rates among wealthy nations.
About 10–12% of all US births are preterm — roughly 380,000 babies every year. After congenital anomalies, preterm birth is the leading cause of infant death. Survivors face real long-term risks: cerebral palsy, chronic lung disease, developmental delay, vision loss, and hearing loss. The earlier a baby is born, the higher those risks.
The Preterm Spectrum
- Late preterm (34–36 6/7 weeks): About 70% of all preterm births. These babies often appear healthy and "big enough" but carry subtle vulnerabilities — feeding difficulties, temperature instability, low blood sugar, jaundice, and breathing issues that may not show up until the first day or two at home. They need close follow-up after discharge.
- Early preterm (<34 weeks): More serious risks across the board. NICU admission is the norm rather than the exception.
- Extremely preterm (<28 weeks): Requires intensive NICU care. Viability begins around 22–23 weeks with aggressive intervention, but survival with disability is common at those gestational ages.
An Important Distinction: PPROM
Preterm labor (contractions causing cervical change) is different from PPROM — Premature Rupture of Membranes before 37 weeks, meaning the bag of water breaks before labor starts. These are related but separate entities with different management pathways. If your water breaks before 37 weeks, go to labor and delivery immediately — do not wait for contractions.
Cause Is Often Unknown
In many cases, no single clear cause is found. This can be frustrating and even guilt-inducing for mothers — but preterm labor frequently happens without any identifiable reason. It is not your fault.
Racial Disparities
Black women in the US experience preterm birth at roughly twice the rate of white and Hispanic women. Research increasingly points to structural racism, chronic stress (the "allostatic load" hypothesis), and systemic barriers to care — not biological differences — as the driving factors behind this disparity.
Risk Factors
Some risk factors are strong predictors; others add moderate risk. Knowing your risk can help you and your provider watch more closely — but having risk factors does not mean you will deliver preterm, and many preterm births happen in women with no known risk factors at all.
Strongest Predictors
- Prior preterm birth: The single strongest risk factor. If you delivered preterm before, your risk of preterm birth in a future pregnancy is 2.5 to 5 times higher than average. The shorter the previous pregnancy, the higher the recurrence risk.
- Short cervical length: Measured by transvaginal ultrasound between 16 and 24 weeks. A cervix shorter than 25 mm is a significant risk factor. A cervix shorter than 10 mm carries approximately a 70% chance of delivery before 35 weeks. This measurement is one of the most useful tools your provider has — ask about it if you have prior preterm birth or other risk factors.
- Positive fetal fibronectin (fFN): A protein in cervicovaginal secretions that is normally not detectable between 22 and 34 weeks. A positive test (above 200 ng/mL) raises concern. More usefully, a negative result is highly reassuring — if fFN is negative, there is less than a 1% chance of delivering within the next 14 days. This makes fFN a very useful test to rule out preterm labor and avoid unnecessary hospitalization or treatment.
Moderate Risk Factors
- Multiple gestation: Twins deliver at about 36 weeks on average; triplets around 33 weeks. Carrying more than one baby significantly raises preterm risk.
- Uterine anomalies: Bicornuate uterus, septate uterus, or other structural differences in the uterus can increase risk.
- Prior cervical procedures: LEEP or cone biopsy for abnormal Pap results can shorten the cervix or weaken it, sometimes leading to cervical incompetence (the cervix opens silently, without contractions).
- Infections: Bacterial vaginosis (BV), urinary tract infections, sexually transmitted infections, and chorioamnionitis (infection of the membranes) are all associated with preterm labor. Treatment of these infections is important throughout pregnancy.
- Short time between pregnancies: An interpregnancy interval of less than 6 months raises preterm risk.
- Substance use: Smoking, alcohol, and illicit substances all increase the risk.
- Domestic violence: Physical and emotional abuse are independently associated with preterm birth.
Social Determinants of Health
Poverty, food insecurity, neighborhood violence, inadequate prenatal care access, and chronic stress are all independently associated with higher preterm birth rates. These are not minor contributors — they are among the most powerful drivers of preterm birth disparities in the US. If you are facing any of these challenges, talk to your prenatal provider or social worker about resources available to you.
Diagnosis: The Tricky Part
Diagnosing preterm labor is genuinely difficult — and getting it wrong in either direction has consequences. Here is the central problem: about 80% of women admitted for suspected preterm labor do not actually deliver preterm. This means most contractions before 37 weeks are not true preterm labor — but you cannot know which ones are without an evaluation.
Symptoms of Preterm Labor
- Regular contractions — every 5 to 10 minutes or closer — that last 30 to 60 seconds
- Pelvic pressure or a feeling of heaviness "down there"
- Low back pain that is dull, constant, or rhythmic
- Abdominal cramping that feels like strong period cramps but doesn't go away
- A change in your vaginal discharge (more, thicker, tinged with pink or blood)
- A feeling that the baby is pushing down harder than usual
How Providers Confirm Preterm Labor
- Contractions on the monitor: Regular pattern documented on the fetal monitor (tocometer)
- Cervical change on exam: Dilation or effacement found on digital vaginal exam, or change from a previous exam
- Transvaginal ultrasound: Short cervical length (<25 mm) supports the diagnosis
- Fetal fibronectin (fFN): A negative result is very reassuring; a positive result raises concern but is not definitive on its own
False Labor (Braxton Hicks Contractions)
Braxton Hicks contractions are irregular practice contractions that most pregnant women feel, especially after 28 weeks. They tend to be irregular, do not intensify over time, often stop with a change in position, rest, or drinking water, and — most importantly — do not cause the cervix to dilate or efface. They can feel exactly like real contractions to you. This is why it can be so hard to tell the difference at home.
When to Go In — Trust Your Instincts
If you have contractions that are 10 minutes apart or less, lasting 30 to 60 seconds, for more than one hour — go in. Even if you are not sure. Even if they feel mild. Even if you've been sent home before. Providers would always rather check you and reassure you than miss true preterm labor. Preterm labor caught early may be stopped or slowed — time matters enormously.
Rule of thumb: If you are asking yourself whether you should call or go in, the answer is yes — call or go in.
Tocolysis: Stopping Contractions
Tocolysis means using medications to slow or stop uterine contractions. It is important to understand the goal clearly: tocolysis is not meant to prevent preterm birth permanently. The realistic goal is to delay delivery for 48 hours — long enough to give antenatal steroids (which need 24–48 hours to fully work) and, if needed, to transfer you to a hospital with a higher-level NICU. Even a 48-hour delay can make a meaningful difference in your baby's outcomes.
Nifedipine (Calcium Channel Blocker) — First-Line
Nifedipine is taken by mouth and is widely used as the first-line tocolytic in the US. A typical regimen is a loading dose of 10–30 mg followed by 10–20 mg every 4 to 6 hours. Common maternal side effects include flushing, headache, and heart palpitations — usually temporary and manageable. Important safety note: do not combine nifedipine with magnesium sulfate, as the two together can cause dangerous drops in blood pressure.
Indomethacin (COX Inhibitor)
Indomethacin is a non-steroidal anti-inflammatory given as a rectal suppository (loading dose 50–100 mg) then orally (25–50 mg every 6 hours). It is effective but has an important limitation: it is only used at or before 32 weeks of gestation, because after that point it can cause premature closure of the ductus arteriosus — a blood vessel in the baby's heart that needs to stay open before birth. It is also limited to short courses (48–72 hours maximum) and is avoided in women with kidney disease.
Magnesium Sulfate
Magnesium is given intravenously. When used before 32 weeks, its primary role is protecting the baby's brain — not stopping contractions (see the Magnesium section below). It does have some tocolytic effect, but this is modest and secondary. It is not used as a standalone tocolytic.
Terbutaline (Betamimetic)
Terbutaline given as a subcutaneous injection (0.25 mg) can briefly slow contractions. Its cardiac side effects — rapid heart rate, palpitations, chest tightness — limit its use to short-term, closely monitored settings. Oral terbutaline for ongoing prevention of preterm birth is not recommended — it is not proven to work for this purpose and has been associated with serious maternal cardiac events.
What Does NOT Work
- Bedrest: No evidence that routine bedrest prevents preterm birth or improves outcomes. It can actually cause harm (blood clots, muscle loss, psychological impact) in prolonged use.
- IV hydration: No evidence that routine hydration for preterm contractions prevents preterm birth. It may be given for comfort or to rule out dehydration as a trigger, but it is not a treatment for preterm labor itself.
- Oral tocolytics for maintenance: Continuing tocolytic pills at home after the acute episode has passed does not prevent recurrence and is not recommended.
Antenatal Corticosteroids: The Single Most Important Treatment
If you are between 24 and 34 weeks pregnant and facing the possibility of preterm birth, the most important thing your medical team can do — beyond anything else — is give you antenatal corticosteroids. These are steroid shots that help your baby's lungs, brain, and intestines mature faster than they normally would.
What Is Given
- Betamethasone: 12 mg injected into muscle, two doses given 24 hours apart. This is the most widely used regimen.
- Dexamethasone: 6 mg injected into muscle, four doses given 12 hours apart. Equivalent effectiveness to betamethasone.
The shots take 24 to 48 hours to reach full effect in the baby. Even if delivery happens sooner, partial benefit still occurs.
What They Prevent
- Respiratory distress syndrome reduced by approximately 40%
- Neonatal mortality reduced by approximately 30%
- Intraventricular hemorrhage (brain bleeding) reduced by approximately 46%
- Necrotizing enterocolitis (serious intestinal condition) reduced by approximately 50%
Rescue Course
If you received steroids more than 14 days ago and are now facing preterm birth again before 34 weeks, your provider may give one additional "rescue course" of steroids. The evidence supports this in certain situations.
Late Preterm Steroids (34–36 6/7 Weeks)
A landmark 2016 trial called the ALPS trial (led by Dr. Gyamfi-Bannerman, published in the New England Journal of Medicine) showed that betamethasone reduces respiratory complications even in late preterm infants — babies at 34 to 37 weeks who look relatively healthy. Based on this evidence, the FDA expanded the approved indication for antenatal steroids to include late preterm pregnancy in 2019. If you are being admitted for possible preterm birth between 34 and 37 weeks, ask whether steroids are indicated for your situation.
Things to Know as a Patient
- The shots may sting briefly — this is normal
- Blood sugar may rise temporarily, especially if you have gestational diabetes — your team will monitor you
- Your white blood cell count will go up — this is an expected steroid effect and does not mean you have an infection
Magnesium Sulfate for Fetal Brain Protection
When preterm birth before 32 weeks appears imminent, magnesium sulfate is given intravenously — not primarily to stop contractions, but to protect your baby's developing brain.
Why Magnesium Protects the Brain
The developing brain of an extremely premature baby is vulnerable to a type of injury called excitotoxicity — essentially, overstimulation of brain cells by glutamate that causes them to die. Magnesium blocks a key receptor (the NMDA glutamate receptor) that mediates this damage, particularly in the white matter of the brain (the "wiring" that connects different brain regions). White matter injury is one of the main causes of cerebral palsy in premature babies.
The Evidence
- The BEAM trial (2008, Rouse et al., New England Journal of Medicine): A randomized controlled trial of 2,241 women. Magnesium sulfate reduced cerebral palsy by 45% in survivors born before 28 weeks.
- The ACTOMgSO4 trial (Crowther et al., 2003, JAMA): Similar findings with consistent reduction in cerebral palsy.
- A Cochrane meta-analysis of four trials found consistent evidence of benefit across all included studies.
How It Is Given
A loading dose of 4 to 6 grams is given intravenously over 15 to 30 minutes (this can cause a sensation of warmth or flushing — tell your nurse if you feel this). Then a maintenance infusion of 1 to 2 grams per hour continues for at least 12 hours, or until delivery.
Monitoring for Safety
Your nurses will check these closely while you are on magnesium:
- Patellar reflex (knee jerk): This is checked every hour. When magnesium levels get too high, the reflex disappears — this is an early warning sign before more serious toxicity
- Breathing rate: Must stay above 12 breaths per minute
- Urine output: Magnesium is cleared by the kidneys
The antidote for magnesium toxicity is calcium gluconate, which is kept at the bedside whenever magnesium is running. Magnesium crosses the placenta, so your newborn may have some effects (low muscle tone, brief breathing issues) that the NICU team will be watching for and can manage.
Progesterone for Prevention
Progesterone is a hormone that plays a key role in maintaining pregnancy — it keeps the uterus relaxed, maintains cervical length, and suppresses inflammation and contractions. Two types of progesterone supplementation have been studied for preventing preterm birth.
Vaginal Progesterone — For Short Cervix
Vaginal progesterone (200 mg per night inserted vaginally from about 20 weeks through 36 weeks) has solid evidence supporting its use in women with a short cervix (less than 25 mm) found on ultrasound, even without a prior preterm birth. Multiple randomized trials support this, including the Fonseca NEJM 2007 trial and the Hassan AJOG 2011 trial. FIGO (the international obstetrics society) recommends it for this indication. If your provider finds a short cervix on ultrasound, ask whether vaginal progesterone is appropriate for you.
17-Alpha-Hydroxyprogesterone Caproate (17-OHPC) — A Complicated Story
17-OHPC (brand name Makena) is a weekly injection given from 16–20 weeks through 36 weeks. It was approved by the FDA in 2011 based on a 2003 trial by Meis et al. in the New England Journal of Medicine showing reduced preterm birth in women with prior preterm birth. However, a much larger subsequent trial (the PROLONG trial) failed to replicate this benefit in a broader population. Based on this, the FDA revoked approval for Makena in 2023.
This does not mean 17-OHPC definitely does not work for any individual — the science is genuinely uncertain and the patient population in the two trials differed. If you have a prior preterm birth, discuss the options and the current evidence honestly with your provider. Decision-making is individualized.
Why Vaginal and Injected Progesterone Have Different Results
This is still not fully understood. The two forms of progesterone are absorbed differently, may reach the uterus and cervix through different pathways, and may act through different mechanisms. Researchers are actively studying this question.
Cervical Cerclage
Cervical cerclage is a surgical procedure in which a stitch (suture) is placed around the cervix to hold it closed and prevent it from opening prematurely. It is typically placed under spinal or general anesthesia as an outpatient procedure.
Types of Cerclage
- McDonald cerclage: A circumferential suture placed around the cervix near the opening (external os). The most common type; can be placed in the office or operating room. Removed at 36–37 weeks or at the onset of labor.
- Shirodkar cerclage: Placed higher, closer to the internal opening of the cervix. Requires more dissection. Used when the McDonald approach is not technically feasible.
- Transabdominal cerclage: Placed through the abdomen, not vaginally, at or near the uterine isthmus (the very top of the cervix). Used when transvaginal cerclage has failed, or when the cervix is too short or damaged for a vaginal approach. Often placed laparoscopically before conception or early in pregnancy. Delivery must be by cesarean section.
When Cerclage Is Recommended
- History-indicated (prophylactic): If you have had one or more second-trimester pregnancy losses or preterm births where the cervix opened painlessly without contractions, your provider may recommend cerclage placed at 12–14 weeks of gestation — before any cervical shortening is visible on ultrasound. This is the strongest indication.
- Ultrasound-indicated: If you have a prior preterm birth AND a short cervix (less than 25 mm) found on ultrasound between 16 and 24 weeks, cerclage combined with vaginal progesterone may be recommended. Evidence supports benefit in this specific group.
- Physical exam-indicated (emergency cerclage): If your cervix is found to be dilated with membranes visible or prolapsed into the vagina — sometimes called a "bulging bag" cerclage. This is controversial and high-risk, but in carefully selected cases it can prolong pregnancy by 4 to 5 weeks.
When Cerclage Does NOT Help
Cerclage does not benefit women who have a short cervix without a prior preterm birth. Multiple meta-analyses have shown no benefit — and it may even cause harm — in this group. Vaginal progesterone alone is preferred for short cervix without prior preterm birth.
Risks of Cerclage
- Infection (chorioamnionitis)
- Premature rupture of membranes triggered by the procedure itself
- Preterm labor from the procedure
- Uterine rupture at delivery if the cerclage is not removed before labor — always remind your provider if you have had a cerclage placed, especially in emergencies
What Parents Should Know: NICU Survival and Care
If your baby is born preterm, they will likely be cared for in a Neonatal Intensive Care Unit (NICU). This can be one of the most frightening experiences a parent can face. Here is honest information to help you understand what to expect.
Survival Rates by Gestational Age
- 22 weeks: 10–30% survival with the most aggressive intervention. Most survivors have significant disabilities. This is the edge of viability — decisions about intensive care at this age are deeply personal and should be made with your medical team.
- 23 weeks: About 50% survival with intensive care.
- 24 weeks: 60–70% survival. This is widely recognized as the threshold of viability where intensive care is generally offered.
- 26 weeks: About 80% survival.
- 28 weeks: About 90% survival.
- 32 weeks: About 95% survival — with NICU support.
- 34–36 weeks (late preterm): Same survival rate as full-term babies, but short-term NICU issues are common.
Common Issues in Premature Babies
- Respiratory distress syndrome (RDS): The lungs haven't made enough surfactant (the substance that keeps air sacs open). Treated with synthetic surfactant given directly into the lungs, and breathing support (CPAP or ventilator).
- Intraventricular hemorrhage (IVH): Bleeding into or around the ventricles of the brain. More common in babies born before 28 weeks. Graded 1 through 4; mild bleeds (grades 1–2) often resolve without long-term consequences; severe bleeds (grades 3–4) are associated with higher risk of developmental problems.
- Necrotizing enterocolitis (NEC): A serious condition where portions of the intestine become inflamed and may die. More common in extremely premature babies. Treatment ranges from antibiotics to surgery.
- Retinopathy of prematurity (ROP): Abnormal blood vessel growth in the eye that can lead to vision problems or blindness if untreated. All premature babies born before 32 weeks are screened by an ophthalmologist.
- Feeding difficulties: Premature babies have not yet developed the coordinated suck-swallow-breathe reflex needed for bottle or breast feeding. Feeding through a small tube in the nose or mouth is routine until the baby is ready.
- Temperature instability: Premature babies have very little body fat for insulation. They are cared for in incubators (isolettes) that maintain their temperature.
- Jaundice: Very common in premature babies. Treated with phototherapy (a special light).
Your Role in the NICU
You are not a bystander in the NICU — you are an essential part of your baby's care team:
- Kangaroo care (skin-to-skin): Holding your baby against your bare chest has proven benefits. Research shows it reduces infection rates, improves feeding, helps regulate the baby's temperature and heart rate, and shortens length of NICU stay. Ask your NICU team when you can start this — often earlier than parents expect.
- Talk and read to your baby: Your voice is recognized and comforting. NICU babies who hear their parents' voices regularly show better development outcomes.
- Ask questions: You have every right to understand what every medication, intervention, and monitor is doing. Ask your nurses and doctors to explain.
- Take care of yourself: NICU stays are a marathon, not a sprint. Eat, sleep, lean on support. Your wellbeing matters too — for you, and for your baby.
Signs That Need Immediate Evaluation
If you are pregnant and before 37 weeks, these are the signs that need immediate attention. Do not wait to see if things get better on their own.
Go to Labor and Delivery Immediately
- Contractions every 5 to 10 minutes, lasting 30 to 60 seconds, for more than one hour — even if they feel mild, even if they feel irregular, even if you are not sure they are real contractions
- 4 or more contractions per hour, even if they are painless — preterm contractions can be completely painless
- Low back pressure or pelvic fullness that does not go away with changing position or resting
- A feeling that something is "different" or "not right" — trust this feeling
- Fluid gushing or leaking from your vagina: do not insert anything into your vagina, lie down, and call 911 if you are soaking through clothing. This may be your water breaking (PPROM) — go in immediately.
- Any vaginal bleeding
Reassuring Signs (Less Urgent)
- Occasional tightening that changes when you change position
- Contractions that stop when you walk, rest, or drink water
- Irregular pattern with no regularity building up over time
- No cervical change on a recent exam (if you were just checked)
The Bottom Line
If you are asking yourself whether you should call your provider or go in, the answer is: go in. Preterm labor caught early has a better chance of being slowed or stopped. A false alarm is not a burden — it is the right call. Every provider would rather check you than miss something serious.
Key Research Papers
-
Blencowe H et al. — National, Regional, and Worldwide Estimates of Preterm Birth Rates in the Year 2010 (Lancet, 2012)
Landmark global epidemiological study estimating preterm birth rates across 184 countries; established the scale of the preterm birth burden worldwide and identified the US as having one of the highest rates among high-income nations.
Search PubMed -
Gyamfi-Bannerman C et al. — Antenatal Betamethasone for Women at Risk for Late Preterm Delivery (ALPS Trial, NEJM 2016)
Randomized controlled trial demonstrating that antenatal betamethasone reduces respiratory complications in late preterm infants (34–36 6/7 weeks) even when they appear clinically stable; led to FDA expansion of the indication for antenatal steroids to include the late preterm period.
PMID 27007960 -
Rouse DJ et al. — Magnesium Sulfate for the Prevention of Cerebral Palsy (BEAM Trial, NEJM 2008)
Multicenter RCT of 2,241 women showing that magnesium sulfate given before 32 weeks reduced the rate of cerebral palsy by 45% in surviving premature infants; established magnesium for neuroprotection as standard of care in the US.
Search PubMed -
Meis PJ et al. — Prevention of Recurrent Preterm Delivery by 17 Alpha-Hydroxyprogesterone Caproate (NEJM 2003)
RCT in women with prior preterm birth showing significant reduction in recurrent preterm birth with weekly 17-OHPC injections; formed the basis for FDA approval in 2011, though later contradicted by the PROLONG trial leading to withdrawal of approval in 2023.
Search PubMed -
Fonseca EB et al. — Progesterone and the Risk of Preterm Birth Among Women with a Short Cervix (NEJM 2007)
RCT demonstrating that vaginal progesterone (200 mg/night) significantly reduced preterm birth before 34 weeks in women with a cervical length below 15 mm; established vaginal progesterone for short cervix as evidence-based prevention.
PMID 17914045 -
Hassan SS et al. — Vaginal Progesterone Reduces the Rate of Preterm Birth in Women with a Sonographic Short Cervix (AJOG 2011)
Large RCT (n=458) confirming that vaginal progesterone gel (90 mg/day) in women with cervical length 10–20 mm reduced preterm birth before 33 weeks and composite neonatal morbidity; reinforced international guidelines favoring vaginal progesterone for short cervix.
Search PubMed -
To MS et al. — Cervical Cerclage for Prevention of Preterm Delivery in Women with Short Cervix (Lancet 2004)
Multicenter RCT demonstrating that cerclage did not significantly reduce preterm birth in women with a short cervix without a prior preterm birth history; clarified that cerclage benefit is restricted to women with prior preterm birth and short cervix, not short cervix alone.
Search PubMed -
Romero R et al. — The Role of Infection in Preterm Labour and Delivery (Paediatric and Perinatal Epidemiology 2001)
Comprehensive review of the evidence linking intrauterine infection and subclinical infection to preterm labor; describes the inflammatory cascade triggered by infection that activates uterine contractions and cervical ripening.
PMID 11520397 -
Goldenberg RL et al. — Epidemiology and Causes of Preterm Birth (Lancet 2008)
Landmark review of preterm birth epidemiology, causes, risk factors, and racial disparities in the US and globally; identified the multifactorial and often idiopathic nature of preterm birth and called for public health approaches to reduction.
PMID 18177778 -
Crowther CA et al. — Effect of Magnesium Sulfate Given for Neuroprotection Before Preterm Birth (ACTOMgSO4 Trial, JAMA 2003)
Australian RCT demonstrating that magnesium sulfate before preterm birth significantly reduced the risk of cerebral palsy and death in surviving children; one of the key trials supporting magnesium neuroprotection alongside BEAM.
Search PubMed -
Delnord M, Zeitlin J — Epidemiology of Late Preterm and Early Term Births: An International Perspective (Seminars in Fetal and Neonatal Medicine 2019)
International comparative study documenting the substantial health burden of late preterm births, which account for 70% of all preterm births; highlights their often-underestimated neonatal risks and long-term developmental outcomes.
Search PubMed -
Fuchs IB et al. — Cervical Length and Fetal Fibronectin as Predictors of Preterm Delivery in High-Risk Patients (AJOG 2004)
Prospective study evaluating the combined predictive value of cervical length measurement and fetal fibronectin testing; demonstrated that negative fFN has very high negative predictive value for ruling out preterm delivery within 14 days.
Search PubMed
Connections
- Reproductive Medicine
- Preeclampsia
- Gestational Diabetes
- Postpartum Hemorrhage
- Recurrent Pregnancy Loss
- Hyperemesis Gravidarum
- Ectopic Pregnancy
- Folate (Vitamin B9)
- Magnesium