Hyperemesis Gravidarum
Table of Contents
- Overview and Definition
- Epidemiology
- Risk Factors
- Pathogenesis
- Clinical Presentation
- Diagnosis and Differential
- Laboratory Findings
- Treatment
- Thiamine and Wernicke's Encephalopathy
- Prognosis and Outcomes
- Key Research Papers
- Featured Videos
Overview and Definition
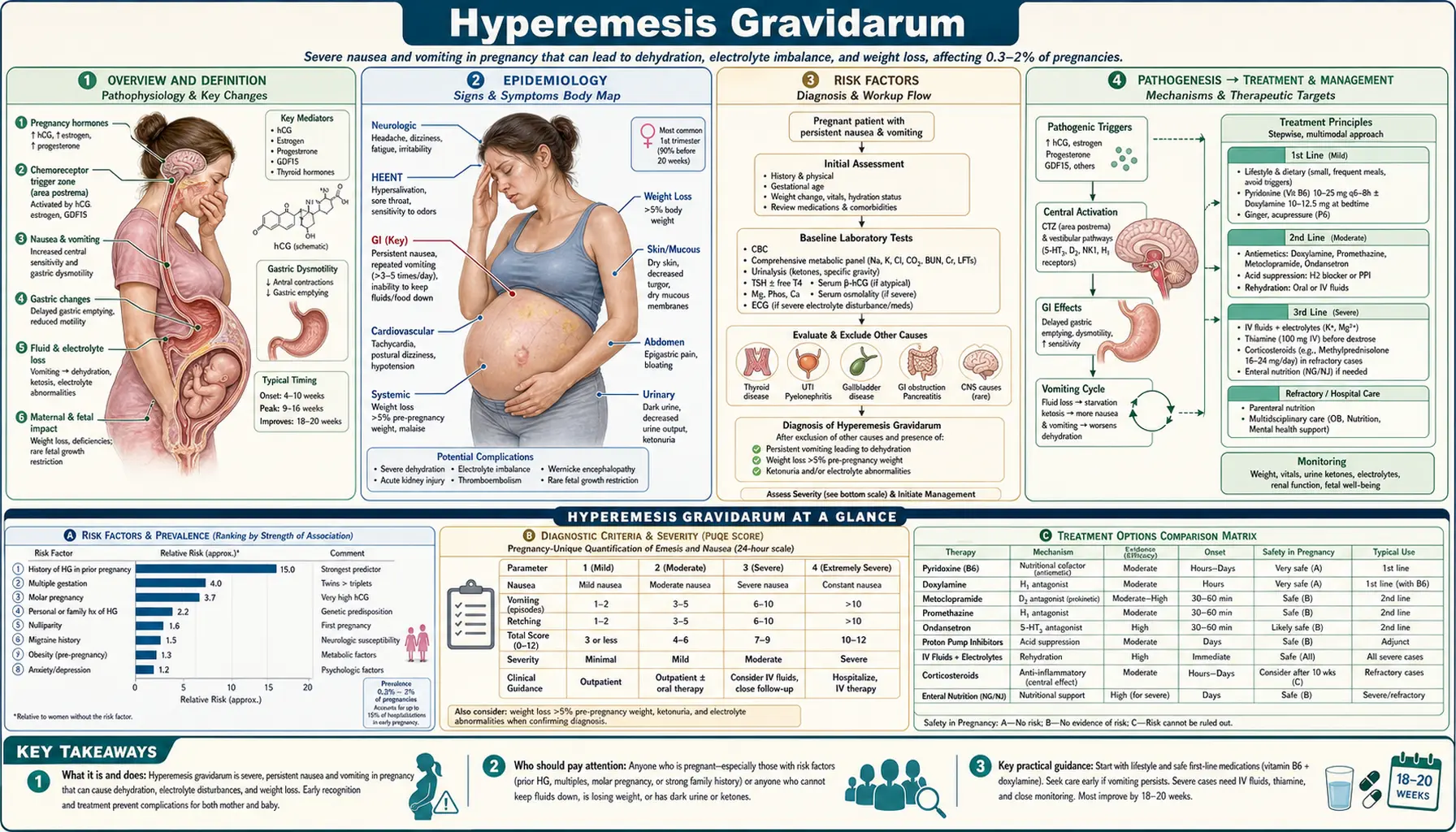
Hyperemesis Gravidarum (HG) is the severe end of the spectrum of pregnancy-related nausea and vomiting. It represents a pathological condition far beyond the common morning sickness experienced by most pregnant women, and can result in serious maternal and fetal complications when not promptly recognized and treated.
The diagnostic criteria for hyperemesis gravidarum include all of the following:
- Persistent nausea and vomiting in pregnancy
- Weight loss of 5% or more of pre-pregnancy body weight
- Ketonuria (reflecting starvation ketosis from carbohydrate depletion)
- Dehydration and electrolyte disturbance may also be present
HG must be distinguished from common nausea and vomiting of pregnancy (NVP), which affects approximately 70–80% of all pregnancies. NVP typically resolves by 14 weeks of gestation, rarely causes significant weight loss, and almost never requires hospitalization. In contrast, HG is severe, prolonged, and significantly impairs daily functioning and nutritional status.
The condition sits at the extreme end of a clinical continuum: mild NVP → moderate NVP → hyperemesis gravidarum. This distinction has practical importance because treatment escalates substantially across the spectrum.
Epidemiology
Hyperemesis gravidarum affects approximately 0.5–2% of all pregnancies worldwide, with prevalence estimates varying by diagnostic criteria applied and population studied. Despite its relatively low frequency compared to NVP, HG carries a disproportionate burden of morbidity.
Key epidemiological features:
- Gestational timing: Symptoms typically peak between 6 and 12 weeks of gestation, correlating with peak human chorionic gonadotropin (hCG) levels. Most cases resolve by 20 weeks.
- Persistent cases: Approximately 10–20% of HG cases persist through the third trimester or even until delivery, representing a particularly challenging subset of patients.
- Hospitalization burden: HG is the leading cause of pregnancy-related hospitalization during the first trimester in many countries, accounting for substantial healthcare costs and resource utilization.
- Psychological impact: HG is associated with significant psychological morbidity, including depression, anxiety, and post-traumatic stress disorder (PTSD). A subset of affected women request pregnancy termination as a direct result of severe, uncontrolled symptoms.
- Quality of life: Studies consistently document dramatic impairment in daily activities, ability to work, and interpersonal relationships during active HG episodes.
Risk Factors
Several clinical, biological, and genetic factors have been identified as increasing a woman's risk of developing hyperemesis gravidarum:
- Prior hyperemesis gravidarum: The strongest individual predictor. Women who experienced HG in a prior pregnancy face a 15–20% recurrence risk in subsequent pregnancies.
- Multiple gestation: Twin and higher-order pregnancies produce markedly elevated hCG levels, increasing HG risk proportionally.
- Hydatidiform mole: Molar pregnancies are associated with markedly elevated hCG and a very high rate of severe hyperemesis.
- Female fetal sex: Pregnancies carrying female fetuses are associated with higher rates and severity of HG, possibly through differential placental hormone production.
- Helicobacter pylori infection: Seroprevalence of H. pylori is significantly higher in women with HG compared to controls; eradication therapy has been shown to improve symptoms in H. pylori-positive patients.
- Hyperthyroid conditions: Pre-existing thyroid disease and gestational transient thyrotoxicosis are associated with increased HG risk.
- Family history: Female relatives (mothers, sisters) with a history of HG confer increased risk, consistent with a heritable component.
- First pregnancy: Primigravidas have modestly higher rates of HG compared to multigravidas (who have had prior HG-free pregnancies).
- Obesity: Paradoxically, obesity appears to confer a lower risk of HG, though the mechanism is incompletely understood.
- GDF15 genetic variants: Emerging evidence implicates variants in the gene encoding growth differentiation factor 15 (GDF15) as a significant genetic risk factor, representing one of the most important recent advances in understanding HG pathogenesis.
Pathogenesis
The pathogenesis of hyperemesis gravidarum is multifactorial. No single mechanism fully explains the condition, and current evidence supports the interplay of hormonal, neurological, gastrointestinal, infectious, and genetic factors.
The hCG Hypothesis
Human chorionic gonadotropin (hCG) is the primary hormonal driver of first-trimester HG. As hCG rises sharply in the first trimester, it stimulates the thyroid gland through cross-reactivity with the TSH receptor, producing a relative transient hyperthyroid state. hCG also directly stimulates the area postrema — the brainstem's chemoreceptor trigger zone — which mediates nausea and vomiting.
This hypothesis is supported by the clinical observation that HG symptoms peak at 6–12 weeks of gestation, precisely when hCG levels are highest, and by the significantly higher severity seen in multiple gestations and molar pregnancies where hCG production is markedly amplified.
GDF15 (Growth Differentiation Factor 15)
GDF15 represents one of the most compelling recent advances in understanding hyperemesis gravidarum. This placental hormone is produced in increasing quantities during the first trimester. Large-scale epidemiologic and genetic studies have established a robust link: maternal genetic variants associated with chronically low pre-pregnancy GDF15 exposure produce heightened sensitivity when pregnancy dramatically raises circulating levels.
GDF15 acts through its receptor, GFRAL, which is expressed selectively in the area postrema and nucleus tractus solitarius of the brainstem — the key brain regions governing nausea and vomiting. This receptor-mediated signaling pathway mediates the emetic response. Critically, this mechanism has become a target for novel pharmacotherapy currently under investigation in clinical trials.
Estrogen Sensitivity
The high estrogen milieu of pregnancy may sensitize central nausea/vomiting centers, contributing to HG susceptibility. The observation that HG is more common with female fetuses (who produce relatively more estrogen) supports this hypothesis.
Gastrointestinal Dysmotility
Pregnancy-associated changes in gastrointestinal function — including slowed gastric emptying, altered gastric motility, and reduced lower esophageal sphincter pressure — may amplify HG severity in susceptible individuals.
Helicobacter pylori
Studies demonstrate significantly higher H. pylori seroprevalence in women with HG versus controls. The mechanism may involve H. pylori-induced changes in gastric motility, mucosal inflammation, and altered hormone metabolism. Importantly, H. pylori eradication has been shown to improve HG symptoms in H. pylori-positive patients, supporting a causal contribution rather than mere association.
Clinical Presentation
Hyperemesis gravidarum typically begins before 9–10 weeks of gestation. The inability to tolerate any oral intake — including fluids — is a hallmark feature that distinguishes HG from ordinary NVP.
Core clinical features include:
- Persistent nausea and vomiting: Continuous, not just morning-limited; often triggered by food odors, tastes, or motion
- Weight loss: At least 5% of pre-pregnancy body weight, often more in severe cases
- Dehydration: Dry mucous membranes, tachycardia, decreased skin turgor, reduced urine output
- Ketonuria: Urine ketones from starvation ketosis as the body metabolizes fat for energy in the absence of dietary carbohydrate
- Electrolyte disturbances: Most commonly hypokalemia; also hyponatremia and hypochloremia
- Ptyalism: Excessive salivation, a distressing symptom some women report as the most disruptive aspect of HG
In severe or prolonged cases, life-threatening complications can develop:
- Wernicke's encephalopathy: From thiamine (vitamin B1) depletion due to prolonged vomiting and inadequate intake — a medical emergency requiring immediate IV thiamine
- Mallory-Weiss tear: Longitudinal mucosal laceration at the gastroesophageal junction from forceful retching, presenting with hematemesis
- Boerhaave's syndrome: Full-thickness esophageal rupture from severe retching — rare but potentially fatal; presents with severe chest and back pain following a vomiting episode
- Fetal growth restriction: In prolonged, severe cases with inadequate maternal nutrition
Diagnosis and Differential
Hyperemesis gravidarum is a clinical diagnosis based on the combination of persistent nausea/vomiting, weight loss ≥5%, and ketonuria in a pregnant woman, after exclusion of other causes.
A thorough differential diagnosis is essential, as several serious conditions can mimic or coexist with HG:
- Urinary tract infection: Nausea and vomiting can accompany pyelonephritis; obtain urinalysis and urine culture
- Cholecystitis and cholelithiasis: Biliary disease is more common in pregnancy; right upper quadrant pain and elevated bilirubin distinguish it from HG
- Pancreatitis: Elevated lipase; epigastric pain radiating to the back
- Hepatitis: Markedly elevated transaminases, jaundice; viral serologies
- Neurological causes: Increased intracranial pressure (migraine, pseudotumor cerebri, intracranial mass) can cause vomiting
- Appendicitis: Position of appendix shifts with advancing pregnancy; right-sided pain with fever
- Gastroparesis: May predate pregnancy; delayed gastric emptying study
Key Differential: Gestational Transient Thyrotoxicosis (GTT) vs. True Graves' Disease
GTT occurs when hCG cross-stimulates the TSH receptor, producing suppressed TSH and mildly elevated free T4. This is biochemically indistinguishable from hyperthyroidism but is self-limited and directly driven by hCG. Critical distinguishing features:
- GTT: Suppressed TSH + mildly elevated free T4, negative thyroid autoantibodies (TRAb and TPO-Ab are absent), self-limited (resolves as hCG falls after first trimester), does not require antithyroid drug treatment
- Graves' disease: Positive TRAb; requires active management; antithyroid drugs (propylthiouracil in first trimester, methimazole after) are indicated
This distinction matters enormously: treating GTT with antithyroid drugs would expose the fetus to unnecessary teratogenic risk (particularly agranulocytosis risk and, with methimazole, aplasia cutis) without clinical benefit.
Laboratory Findings
Laboratory evaluation in HG reflects the consequences of prolonged vomiting, dehydration, and starvation. Key findings include:
- Hypokalemia: The most common electrolyte abnormality. Repeated vomiting results in loss of gastric acid containing potassium ions, leading to significant potassium depletion. Severe hypokalemia can cause dangerous cardiac arrhythmias and muscle weakness.
- Hyponatremia: From volume depletion and free water intake without adequate sodium replacement.
- Hypochloremia: Loss of hydrochloric acid in gastric contents.
- Metabolic alkalosis: Consequence of hydrogen ion loss through vomiting; serum bicarbonate is elevated.
- Elevated hematocrit: Hemoconcentration from dehydration; artifactually "normal" hemoglobin may mask true anemia.
- Ketonuria: Detected on urine dipstick; reflects starvation ketosis. A required element of the diagnostic criteria.
- Elevated BUN and creatinine: Prerenal azotemia from volume depletion; BUN:creatinine ratio typically greater than 20:1.
- Elevated liver transaminases: AST and ALT are elevated in up to 40% of hospitalized HG patients. The mechanism involves centrilobular hepatocyte damage from nutritional deprivation and metabolic stress. These abnormalities resolve with rehydration and nutritional repletion and do not require specific hepatic treatment.
- Suppressed TSH with mildly elevated free T4: Reflecting gestational transient thyrotoxicosis (see Diagnosis section); TRAb and TPO-Ab are negative.
- Thiamine level: Should be checked in any patient with prolonged HG, particularly before initiating IV glucose; low levels confirm thiamine deficiency and mandate immediate replacement.
Treatment
Management of hyperemesis gravidarum follows a stepwise approach, escalating from lifestyle modification and oral medications to IV fluids, enteral nutrition, and in refractory cases, parenteral nutrition.
Outpatient and Mild Measures
- Small, frequent meals: Bland, low-fat, high-carbohydrate foods; eat before rising from bed
- Ginger: Evidence-based efficacy at 1 gram per day (divided doses); reduces nausea severity in multiple RCTs
- Trigger avoidance: Identify and avoid specific food odors, tastes, or environmental triggers
- Acupressure: P6 (Neiguan) wristbands provide modest benefit in some patients with minimal risk
- Rest and supportive care
First-Line Pharmacological Therapy
- Pyridoxine (Vitamin B6): 10–25 mg three times daily; reduces nausea severity; FDA Pregnancy Category A; well-established safety profile; often used as monotherapy for milder cases
- Pyridoxine + Doxylamine (Diclegis/Bonjesta): The FDA-approved combination for NVP/HG; considered first-line pharmacotherapy; Category A; multiple safety studies do not demonstrate significant teratogenic risk
- Antihistamines: Diphenhydramine, dimenhydrinate; effective for nausea/vomiting; generally considered safe in pregnancy
Antiemetic Agents
- Ondansetron (Zofran): A 5-HT3 receptor antagonist; the most widely used IV and oral antiemetic for HG. Some observational studies have raised concern about a possible small increase in risk of cardiac septal defects when used in early first trimester (6–10 weeks). The absolute risk increase, if real, remains small. Clinical guidance: discuss the risk/benefit with the patient; consider avoiding at 6–10 weeks if alternatives are sufficient; use when benefits outweigh risks in severe HG.
- Metoclopramide: Dopamine antagonist; also has prokinetic properties helpful in gastric dysmotility. Risk of extrapyramidal side effects (akathisia, dystonic reactions) at higher doses or with prolonged use; tardive dyskinesia with very long-term use.
- Prochlorperazine: Phenothiazine antiemetic; effective but higher sedation profile.
- Promethazine: Also effective but associated with significant maternal sedation and respiratory depression in high doses.
Intravenous Fluids and Electrolyte Replacement
- IV fluid resuscitation: Normal saline (0.9% NaCl) or Lactated Ringer's solution for rehydration
- Critical rule — Thiamine BEFORE glucose: Always administer thiamine 100 mg IV before any dextrose-containing IV fluids. Administering glucose without thiamine in a thiamine-depleted patient can precipitate or worsen Wernicke's encephalopathy (see dedicated section below).
- Potassium chloride (KCl): Added to IV fluids for correction of hypokalemia; rate of replacement determined by severity and cardiac monitoring
- Magnesium: Replacement if hypomagnesemia is present
Nutritional Support
- Enteral nutrition: Nasogastric (NG) or nasojejunal (NJ) tube feeding is preferred when oral intake is impossible but the gastrointestinal tract remains functional. NJ feeding bypasses the stomach and may be better tolerated. Enteral nutrition is always preferred over parenteral when feasible.
- Total Parenteral Nutrition (TPN): Reserved as a last resort for refractory HG when enteral feeding is not possible or tolerated. Associated with significant risks including central line sepsis, thrombosis, metabolic derangements, and cholestasis. Should be managed by a multidisciplinary team including nutrition support specialists.
Corticosteroids
Methylprednisolone (16 mg three times daily for 3 days, then gradually tapered) has been used for refractory HG. Evidence is mixed, with some trials showing benefit and others not. Important caveat: avoid before 10 weeks of gestation due to a small but documented association with oral cleft formation (cleft palate/lip) in early organogenesis. Reserve for severe, refractory cases after other therapies have been exhausted.
Emerging Therapies
Given the identification of GDF15 as a central pathogenic hormone, anti-GDF15 therapies are now in active clinical development. Early-phase trials have shown promising results in reducing HG severity. These agents represent the first mechanism-targeted pharmacological approach to HG and may represent a major advance in treatment for this poorly-managed condition.
Thiamine and Wernicke's Encephalopathy
Wernicke's encephalopathy (WE) is a medical emergency that can develop in women with hyperemesis gravidarum due to thiamine (vitamin B1) depletion. Because thiamine is water-soluble and not stored in significant quantities, prolonged vomiting and inadequate dietary intake rapidly deplete thiamine stores — sometimes within weeks.
Classic Triad of Wernicke's Encephalopathy
- Confusion / altered mental status: Ranging from mild cognitive impairment to frank encephalopathy
- Ophthalmoplegia: Lateral rectus palsy (sixth nerve palsy) causing horizontal diplopia; nystagmus; gaze palsies
- Ataxia: Unsteady gait from cerebellar and vestibular involvement
The complete triad is present in only about 30% of cases. A high index of clinical suspicion is essential — any pregnant patient with prolonged vomiting who develops neurological symptoms must be treated immediately.
The Critical Rule: Thiamine BEFORE Dextrose
This is one of the most important safety principles in managing HG with IV fluids. Administering intravenous glucose (dextrose) to a thiamine-depleted patient causes acute demand for thiamine in glucose metabolism — specifically in the pyruvate dehydrogenase and alpha-ketoglutarate dehydrogenase complexes of the Krebs cycle. Without thiamine, these enzymatic steps fail, leading to lactate accumulation and neuronal death in metabolically vulnerable brain regions.
Rule: ALWAYS administer thiamine 100 mg IV BEFORE any dextrose-containing IV fluid in a patient with prolonged vomiting or suspected thiamine deficiency.
Thiamine dose for Wernicke's treatment: 100–500 mg IV thiamine, three times daily, until no further neurological improvement is seen.
Korsakoff Psychosis
Untreated or inadequately treated Wernicke's encephalopathy progresses to Korsakoff syndrome (Korsakoff psychosis), characterized by severe anterograde amnesia (inability to form new memories), confabulation, and retrograde amnesia. Unlike Wernicke's encephalopathy (which responds to thiamine), Korsakoff syndrome may be permanent and irreversible. Prevention — by prompt thiamine administration before the Wernicke's stage — is far more effective than treatment after the fact.
Prognosis and Outcomes
The prognosis for hyperemesis gravidarum is generally favorable in terms of fetal survival, but maternal morbidity — including psychological sequelae — can be significant and lasting.
Resolution of Symptoms
The majority of HG cases resolve by 20 weeks of gestation, paralleling the decline in hCG levels. However, 10–20% of affected women experience symptoms that persist through the third trimester or even until delivery, representing a particularly burdened group requiring ongoing multidisciplinary support.
Fetal Outcomes
- In mild to moderate HG with adequate treatment, fetal outcomes are generally normal
- Severe, prolonged HG with inadequate nutrition is associated with fetal growth restriction and increased risk of preterm birth
- Some studies suggest associations with small-for-gestational-age infants in the most severe cases
- Paradoxically, some data suggest that women with HG have lower rates of miscarriage compared to NVP — possibly reflecting the hormonal vigor of a healthy first-trimester pregnancy
Maternal Psychological Sequelae
Psychological morbidity following HG is common and underrecognized. Depression, anxiety disorders, and PTSD can persist well beyond resolution of the physical symptoms. Many women report that HG was among the most traumatic experiences of their lives. A significant proportion of women who experienced HG do not complete planned subsequent pregnancies, citing fear of recurrence.
Recurrence
Women who experienced HG in one pregnancy face approximately a 15–20% risk of recurrence in subsequent pregnancies. This risk can inform preconception counseling and allow for early, proactive management in future pregnancies.
Key Research Papers
-
ACOG Practice Bulletin 153: Nausea and Vomiting of Pregnancy (2016)
American College of Obstetricians and Gynecologists. Comprehensive clinical practice guidelines covering diagnosis, differential, and stepwise management of NVP and HG.
Search PubMed -
Fejzo M et al. — GDF15 and Hyperemesis Gravidarum (Nature, 2023)
Landmark genome-wide association and functional study establishing GDF15 as a central hormonal driver of HG. Demonstrated that maternal variants causing low pre-pregnancy GDF15 exposure increase sensitivity to the elevated levels of the first trimester. Identified GFRAL as the relevant brainstem receptor — opening the door to targeted therapy.
Search PubMed -
Fejzo MS et al. — Genetics of Severe Nausea and Vomiting of Pregnancy
Early genetic study establishing hereditary components of severe NVP and HG, supporting familial clustering and susceptibility loci.
Search PubMed -
London V et al. — Hyperemesis Gravidarum: A Review (2020)
Comprehensive review covering pathophysiology, clinical management, and emerging therapies for HG, with emphasis on multidisciplinary care approaches.
Search PubMed -
Grooten IJ et al. — H. pylori and Hyperemesis Gravidarum: Systematic Review and Meta-Analysis (2017)
Systematic review establishing a significant association between H. pylori infection and HG; meta-analysis supporting that H. pylori eradication improves HG outcomes in seropositive patients.
Search PubMed -
Boelig RC et al. — Interventions for Treating Hyperemesis Gravidarum (Cochrane Review, 2013)
Cochrane systematic review evaluating the evidence base for pharmacological and non-pharmacological interventions in HG, including antiemetics, corticosteroids, and nutritional support.
Search PubMed -
Madjunkova S et al. — Ondansetron Safety During Pregnancy (2018)
Prospective cohort study examining ondansetron safety in first-trimester pregnancy exposure, contributing data on the cardiac septal defect signal and risk quantification.
PMID 30001660 -
Koren G et al. — Thiamine Deficiency in Hyperemesis Gravidarum (2019)
Study documenting the prevalence of thiamine deficiency in HG patients and the risk of Wernicke's encephalopathy; reinforces the clinical protocol of thiamine administration before IV glucose.
Search PubMed -
Russo-Stieglitz KE et al. — Hyperemesis Gravidarum (2014)
Clinical review covering differential diagnosis, laboratory evaluation, and inpatient versus outpatient management strategies for HG.
Search PubMed -
Goodwin TM — Hyperemesis Gravidarum (2008)
Foundational review of the hormonal pathogenesis of HG, with particular focus on the hCG hypothesis and its relationship to gestational thyrotoxicosis.
Search PubMed -
Klebanoff MA, Koslowe PA et al. — Epidemiology of Vomiting in Early Pregnancy (1985)
Epidemiological study examining prevalence, timing, and risk factors for nausea and vomiting in pregnancy, establishing foundational population data.
PMID 17267839 -
Castillo MJ et al. — Hyperemesis Gravidarum and Neonatal Outcomes (2021)
Study examining maternal and neonatal outcomes associated with HG, including rates of fetal growth restriction, preterm birth, and maternal psychological morbidity.
Search PubMed
Connections
- Reproductive Medicine
- Ectopic Pregnancy
- Gestational Trophoblastic Disease
- Preeclampsia
- Gestational Diabetes
- Thiamine (Vitamin B1)
- Pyridoxine (Vitamin B6)