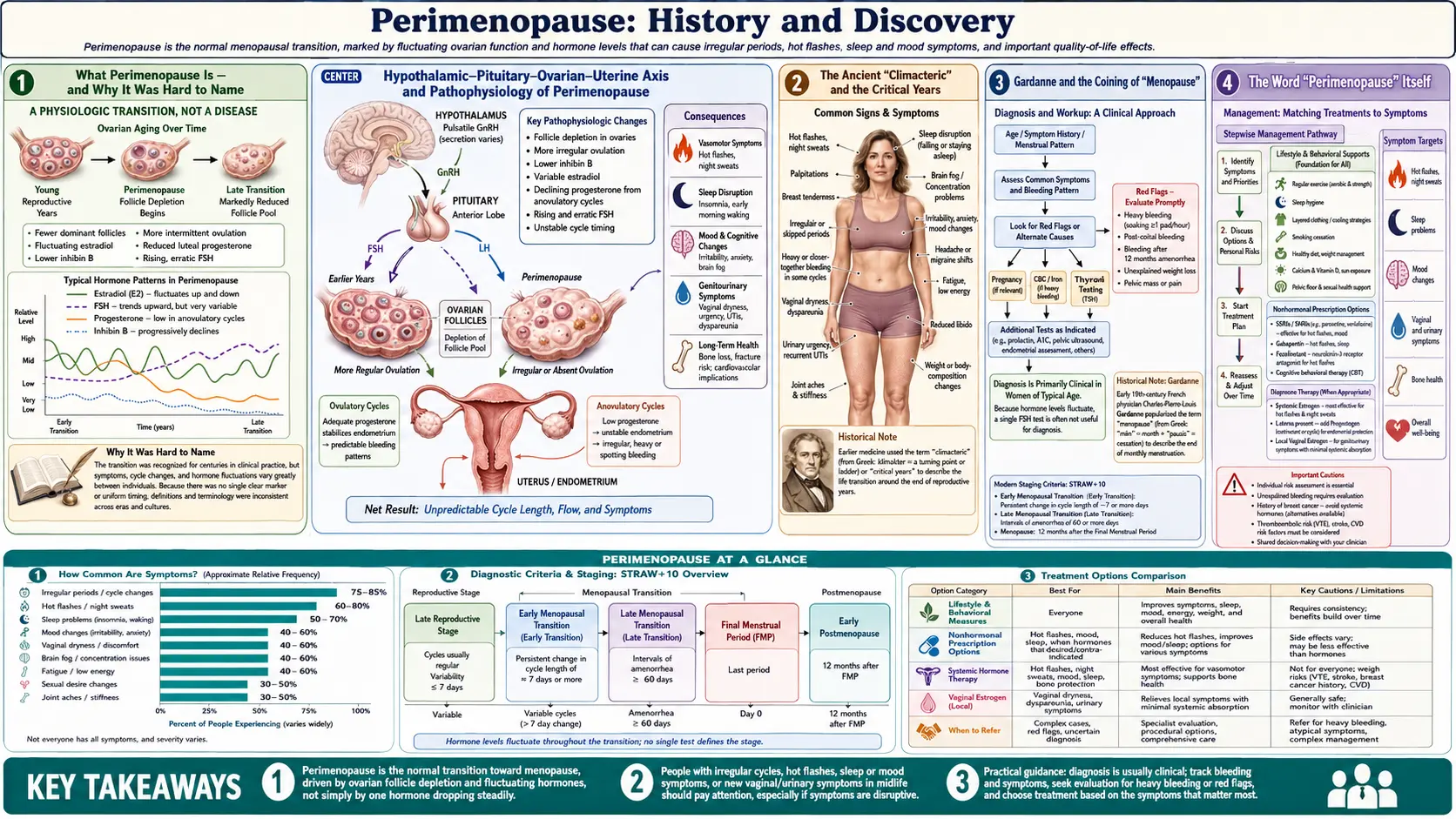
Perimenopause: History and Discovery
Perimenopause — the menopausal transition — is the stretch of years when a woman's hormones begin to fluctuate and her menstrual cycles grow irregular on the way to her final period. For most of recorded history it had no separate name at all: it was folded into the broad, ancient idea of the climacteric, the "critical years" of midlife. The word menopause itself was only coined in the early nineteenth century by the French physician Charles de Gardanne, and even then it named the ending of menstruation rather than the turbulent run-up to it. The idea that the transition deserves its own clear definition — with measurable stages marked by changes in the menstrual cycle and the hormone FSH — is largely a story of the late twentieth and early twenty-first centuries, culminating in the STRAW staging system of 2001 and its 2011 update. This page traces how a vague, often-feared "change of life" became a well-mapped, normal life stage. Perimenopause is a natural transition, not a disease, though its symptoms sometimes need real medical attention.
Table of Contents
- What Perimenopause Is — and Why It Was Hard to Name
- The Ancient "Climacteric" and the Critical Years
- Gardanne and the Coining of "Menopause"
- The Word "Perimenopause" Itself
- Discovering the Endocrinology: Estrogen and FSH
- Mapping the Transition: The Great Cohort Studies
- STRAW: Putting Stages on the Transition (2001 and 2011)
- Understanding the Symptom Picture
- A Normal Life Stage, Better Understood
- Research Papers and References
- Connections
- Featured Videos
What Perimenopause Is — and Why It Was Hard to Name
Perimenopause literally means "around menopause" (from the Greek peri, near or around). It is the transitional phase — often several years long — during which the ovaries gradually wind down, the levels of reproductive hormones swing and then decline, and menstrual cycles become irregular before stopping altogether. It begins, in the modern understanding, when cycles first start to vary noticeably in length, and by convention it is considered to end twelve months after the very last menstrual period. That last period is menopause in the strict sense: not a phase but a single moment in time, and one that can only be identified looking backward, once a full year has passed with no bleeding.
This is the central reason perimenopause was so hard to pin down for so long. Menopause is defined retrospectively — you only know the final period was the final one after a year of waiting — so the transition leading up to it has fuzzy edges by its very nature. A woman in the thick of perimenopause cannot know in the moment whether a given period is her last; she may bleed again after six months of silence. For centuries, that ambiguity meant the run-up to menopause and menopause itself were simply lumped together as one blurry midlife event rather than separated into a process (the transition) and a landmark (the final period).
Crucially, perimenopause is a normal stage of life, not an illness. Every woman who lives long enough passes through it, just as every adolescent passes through puberty. Framing it as a disease has done real historical harm. At the same time, the hormonal turbulence of the transition can produce genuinely disruptive symptoms — hot flashes, disturbed sleep, mood changes, heavy or unpredictable bleeding — that deserve to be taken seriously and, when needed, treated. The modern history of perimenopause is in large part the story of learning to hold both truths at once: that it is natural, and that its symptoms can still merit care.
The Ancient "Climacteric" and the Critical Years
Long before anyone spoke of menopause or perimenopause, midlife change was understood through the old idea of the climacteric. The word comes from the Greek klimakter, meaning the rung of a ladder, and figuratively a critical step or turning point in life. In classical and Renaissance thought, the "climacteric years" were specific ages — often the years that were multiples of seven, with the sixty-third year (the so-called grand climacteric) regarded as especially dangerous — when the whole body was believed to pass through a perilous transition that could lead either to renewed vigor or to decline and death.
Two features of this older framework are worth underlining because they explain why the transition went unnamed for so long. First, the climacteric was understood to apply to both sexes: it described a general critical passage of midlife, not a specifically female or specifically reproductive event. Second, it was vague by design — a broad span of bodily change rather than a precise physiological process tied to the ovaries. By the eighteenth and nineteenth centuries, in medical usage the term had drifted to refer especially to the changes around the end of menstruation in women, and "the climacteric" became, for a time, a near-synonym for what we would now call the menopausal years. But it still bundled the transition and its endpoint together, and still carried the old freight of danger and crisis. The scholarly history of this shift — from the ancient anni climacterici to the modern concept of menopause — has been traced in the medical-history literature, and the etymology is well documented in standard reference works.
The persistence of "climacteric" well into the twentieth century — it is still encountered in older medical writing and in some non-English traditions — is a reminder that the modern, finely-staged picture of perimenopause is recent. For most of the past, the years of fluctuating hormones and irregular cycles had no name of their own; they were simply part of the critical years.
Gardanne and the Coining of "Menopause"
The first decisive step toward a modern vocabulary came in early-nineteenth-century France. The physician Charles-Pierre-Louis de Gardanne set out to give the end of menstruation a name of its own, distinct from the sprawling old climacteric. In an 1812 work he tried out an awkward coinage — rendered as menespausie (or la ménespausie) — and by his revised 1821 treatise he had refined it into the word we still use: ménopause. The 1821 book bore a title that perfectly captures the transitional moment in medical thinking: De la ménopause, ou de l'âge critique des femmes ("On menopause, or the critical age of women") — the new, specific term sitting right alongside the old language of the "critical age."
Gardanne built the word from Greek roots: men (month, as in menstruation) and pausis (a pause or cessation) — literally, the cessation of the monthly cycle. The exact dating is worth stating carefully, because it is sometimes given simply as "1812" and sometimes as "1821": the historical record indicates an initial, clumsier form around 1812 and the now-standard term in the 1821 edition. Both dates are therefore correct for different stages of the coinage, and reputable histories of menopause cite them together.
What matters for the history of perimenopause is what Gardanne's word did and did not do. It gave a clean name to the cessation of menstruation — the endpoint — and over the following century "menopause" gradually displaced "the climacteric" in much of medicine. But it still did not single out the transition leading up to that endpoint. For more than a century after 1821, "menopause" was routinely used loosely to cover both the years of change and the final cessation. Distinguishing the process from the point — the perimenopausal transition from menopause itself — would take the endocrinology and the epidemiology of the twentieth century.
The Word "Perimenopause" Itself
The term perimenopause is younger than menopause, but it is older than many people assume, and accuracy matters here. It is sometimes said to be a purely late-twentieth-century invention; that is not quite right. The word is documented in the medical literature by at least the early 1930s — it appears, for example, in the obstetrics-and-gynecology textbook tradition of Joseph B. DeLee and J. P. Greenhill — so "perimenopause" as a piece of medical vocabulary is roughly a century old, not a few decades old.
What genuinely is recent is its rise to common, precise, clinically-defined usage. For most of the twentieth century the word was uncommon and loosely applied; "menopause" still did most of the work, often standing in for the whole transition. It was in the later decades of the twentieth century — as researchers began to track the transition prospectively and to measure its hormones — that "perimenopause" and "the perimenopausal period" came into wide use specifically to name the transition itself, distinct from menopause-the-moment. The honest summary is therefore: the word has existed since at least the 1930s, but its modern role — a defined, staged transitional phase set apart from menopause — is a development of the late twentieth century, crystallized by the staging work described below.
Alongside "perimenopause," the World Health Organization and others helped standardize a fuller nomenclature — premenopause, perimenopause (the menopausal transition plus the year after the final period), menopause (the final menstrual period), and postmenopause. Getting these words to mean consistent things across studies and clinics turned out to be surprisingly difficult, and tidying up that "confusing nomenclature" was an explicit goal of the staging effort that followed.
Discovering the Endocrinology: Estrogen and FSH
The modern understanding of perimenopause rests on hormones that were themselves only discovered in the twentieth century. Estrogen was isolated and characterized in the late 1920s and early 1930s, and the pituitary gonadotropins — follicle-stimulating hormone (FSH) and luteinizing hormone (LH) — were worked out over the same era. Only once these messengers were known and measurable could the transition be understood as an endocrine process rather than a vague "change."
The picture that emerged is this. The ovaries hold a finite reserve of follicles that declines steadily across a woman's life. As that reserve dwindles in the forties, the ovaries respond less reliably to the pituitary's signals. The brain compensates by pushing harder — so FSH levels rise — while estrogen output becomes erratic, swinging high and low before its eventual decline. This is why perimenopause is characterized not by a smooth fall in estrogen but by hormonal turbulence: cycles can shorten, lengthen, or be skipped, and symptoms can come and go with the swings. A sustained rise in FSH, together with the menstrual changes, became the key biochemical signature of the transition — though, importantly, because hormones fluctuate so much from day to day, a single blood test is a notoriously unreliable way to "diagnose" perimenopause in an individual woman.
This endocrine framing — declining and fluctuating estrogen, rising FSH, driven by a falling follicle reserve — is a distinctly modern achievement. It transformed perimenopause from a cluster of subjective complaints into a measurable physiological process, and it supplied the hormonal criteria that the staging systems would later use to draw lines through the transition.
Mapping the Transition: The Great Cohort Studies
Knowing the hormones in principle is not the same as knowing how the transition actually unfolds in real women over real years. That required longitudinal cohort studies — following the same women for years, tracking their cycles, hormones, and symptoms as they passed through the change. Several such studies, launched mostly in the 1990s, are the empirical backbone of everything we now say about perimenopause.
The largest and most influential is the Study of Women's Health Across the Nation (SWAN), a multi-site, multi-ethnic United States cohort that enrolled roughly 3,300 women in their forties (about ages 42–52 at baseline) in the mid-1990s and has followed many of them for two decades and more. SWAN was designed expressly to characterize the physiological and psychosocial changes of the menopausal transition across different racial and ethnic groups, and its findings — on the timing and duration of hot flashes, on bleeding patterns, on bone, mood, sleep, and cardiovascular risk — have repeatedly reshaped the field. Other important longitudinal projects, such as the Melbourne Women's Midlife Health Project and the Seattle Midlife Women's Health Study, contributed complementary data from other populations.
These cohorts did something the older, cross-sectional snapshots never could: they showed the transition as a trajectory. They demonstrated, for instance, that vasomotor symptoms often begin in perimenopause (not only after the final period) and can last far longer than once believed; that the duration of the transition varies widely; and that experience differs meaningfully across ethnic groups. This accumulated, prospective evidence is precisely what made a rigorous staging system both possible and necessary — there was now enough real data to draw the lines.
STRAW: Putting Stages on the Transition (2001 and 2011)
The landmark moment for the field was the Stages of Reproductive Aging Workshop (STRAW), convened in Park City, Utah, in July 2001. A group of experts gathered specifically to fix the "confusing nomenclature" of the reproductive years and to build, for the first time, a standardized staging system for female reproductive aging. The result, published in 2001 (Soules and colleagues), divided a woman's reproductive life into seven stages anchored on the final menstrual period (FMP): five stages before it and two after. The stages immediately preceding the FMP — the menopausal transition — were defined using concrete criteria: changes in menstrual cycle length together with elevated FSH. For the first time, the transition was not a vague impression but a set of stages with explicit, reproducible definitions.
A decade later the system was revisited and refined. The STRAW + 10 update, published in 2012 (Harlow and colleagues, reporting the 2011 workshop), drew on the by-then-mature cohort data — including SWAN and the ReSTAGE Collaboration's work on cycle criteria — to sharpen the bleeding-pattern definitions for the early and late transition, to better specify the late reproductive and early postmenopausal stages, and to refine how FSH and other markers are used. Importantly, STRAW + 10 recommended that the staging apply broadly regardless of a woman's age, ethnicity, body size, or lifestyle, making it a genuinely general framework. It remains the international gold standard for describing where a woman sits along the path from full fertility to postmenopause.
The significance of STRAW for the history of perimenopause is hard to overstate. It took a transition that had been blurry since antiquity — bundled into the climacteric, then loosely covered by the word "menopause" — and gave it a precise, staged, evidence-based map. After STRAW, "perimenopause" could be defined and located rather than merely gestured at, and research and clinical care across the world could finally speak a common language about the transition.
Understanding the Symptom Picture
Hand in hand with the staging came a clearer, more honest understanding of what the transition actually feels like. The hallmark vasomotor symptoms — hot flashes and night sweats — had been associated with "the change" for generations, but the cohort studies revealed how variable and how durable they really are: they frequently begin during perimenopause, while periods are still occurring, and for many women they persist for years, sometimes well into postmenopause. The old assumption that flashes were a brief, post-menopausal nuisance gave way to a picture of a longer, earlier, and more individual experience.
The transition's reach beyond hot flashes also came into focus. Modern research links perimenopause to disturbed sleep, to changes in mood (including a window of heightened vulnerability to depressive symptoms in some women), to irregular and sometimes heavy menstrual bleeding, and to longer-term shifts in bone density and cardiovascular risk factors that accelerate around the final menstrual period. Understanding these as connected manifestations of the same hormonal transition — rather than as unrelated midlife complaints — is itself a modern synthesis, and it is what allows symptoms to be anticipated, explained, and managed.
This is also where the "normal life stage, but symptoms can still need care" theme becomes practical. Recognizing that perimenopausal symptoms are real and biologically grounded — not imagined, and not a personal failing — has been an important corrective to centuries of dismissiveness. The practical management of these symptoms (lifestyle measures, hormonal and non-hormonal therapies, and when to seek evaluation for abnormal bleeding) is taken up on the companion Perimenopause overview and the related Menopause and HRT page.
A Normal Life Stage, Better Understood
Seen as a whole, the history of perimenopause is a movement from fear and vagueness toward clarity and dignity. The ancient world saw only the climacteric — the dangerous critical years, shared by both sexes and explained by numerology as much as biology. Gardanne, in 1812 and 1821, named the endpoint, menopause. The twentieth century supplied the hormones — estrogen, FSH — and then the long cohort studies that watched the transition unfold in thousands of real women. STRAW, in 2001 and again in 2011, finally drew the map, turning the perimenopausal transition into a set of defined, measurable stages.
A recurring and welcome theme in this modern history is the explicit reframing of perimenopause and menopause as normal stages of life rather than diseases or deficiencies. Gardanne's own title still called it the "critical age," and for much of the nineteenth and twentieth centuries the transition was medicalized, pathologized, and too often dismissed. The contemporary view — reflected in the language of bodies like the World Health Organization — treats it as a universal, natural transition that nonetheless can produce symptoms worth treating. That balance, hard-won, is the central insight of the whole story.
It is also worth being clear about what remains uncertain. The biology of the menopausal transition is now well mapped at the level of stages and hormones, but questions of why human females undergo menopause at all — the evolutionary explanations, including the much-discussed "grandmother hypothesis" — remain genuinely open scientific hypotheses rather than settled facts, and they are presented as such in the research literature. The history of perimenopause, in other words, is still being written: a once-nameless passage of midlife has become one of the most carefully staged transitions in human biology, even as some of its deepest questions stay unanswered.
Research Papers and References
The list below combines the key peer-reviewed sources on the staging and epidemiology of the menopausal transition with curated PubMed topic-search links into the historical and nomenclature literature. Historical primary texts — notably Gardanne's 1821 De la ménopause, ou de l'âge critique des femmes — are named in the article as historical sources rather than as modern citations. Each link opens in a new tab; the National Library of Medicine (PubMed) is the host for the search links.
- Soules MR, Sherman S, Parrott E, et al. Executive summary: Stages of Reproductive Aging Workshop (STRAW). Fertility and Sterility. 2001;76(5):874-878. — doi:10.1016/S0015-0282(01)02909-0 · PMID 11704104
- Harlow SD, Gass M, Hall JE, et al. Executive summary of the Stages of Reproductive Aging Workshop + 10: addressing the unfinished agenda of staging reproductive aging. Menopause. 2012;19(4):387-395. — doi:10.1097/gme.0b013e31824d8f40 · PMID 22343510
- A review of menopause nomenclature (premenopause, perimenopause, menopause, postmenopause). Reproductive Health / NLM. — PMC8805414: review of menopause nomenclature
- Santoro N. Perimenopause: From Research to Practice. Journal of Women's Health. 2016;25(4):332-339. — PMID 26653408
- Study of Women's Health Across the Nation (SWAN) — design, cohort, and findings on the menopausal transition. — PubMed: SWAN and the menopausal transition
- Historical roots of the "climacteric": from anni climacterici to menopause. — PMID 17153291
- History and medicalization of menopause — Gardanne and the coining of the term. — PubMed: history of menopause and the term "menopause"
- Vasomotor symptoms (hot flashes) across the menopausal transition — onset, duration, and trajectory. — PubMed: vasomotor symptoms and the menopausal transition
- FSH and estradiol changes across the perimenopausal transition. — PubMed: FSH and estradiol in the menopausal transition
- Depression, mood, and sleep during perimenopause. — PubMed: mood and sleep in perimenopause
- ReSTAGE Collaboration — menstrual-cycle criteria for staging the menopausal transition. — PubMed: ReSTAGE menstrual-cycle staging criteria
- Evolution of menopause and the "grandmother hypothesis" (presented as an evolutionary hypothesis). — PubMed: evolution of menopause and the grandmother hypothesis
- WHO Scientific Group — research on the menopause and definitions of the menopausal transition. — PubMed: WHO definitions of menopause and perimenopause
External Authoritative Resources
- World Health Organization — Menopause (fact sheet)
- The Menopause Society (formerly NAMS) — professional & patient resources
- PubMed — all research on perimenopause and the menopausal transition
Connections
- Reproductive Medicine
- Perimenopause: Symptom Tracker & Hormonal Testing — the practical companion to this history — why a single FSH or estradiol draw misleads, what the STRAW+10 stages mean for you now, a three-month tracking method, and when to start HRT.
- Perimenopause (overview)
- Menopause and Hormone Replacement Therapy (HRT)
- Osteoporosis
- Postmenopausal Osteoporosis and Hormone Therapy
- Uterine Fibroids
- Ovarian Cysts
- Menopause — the landmark final period that perimenopause leads up to, and the term Gardanne coined in 1821.
- All Conditions