Infertility: History and Discovery
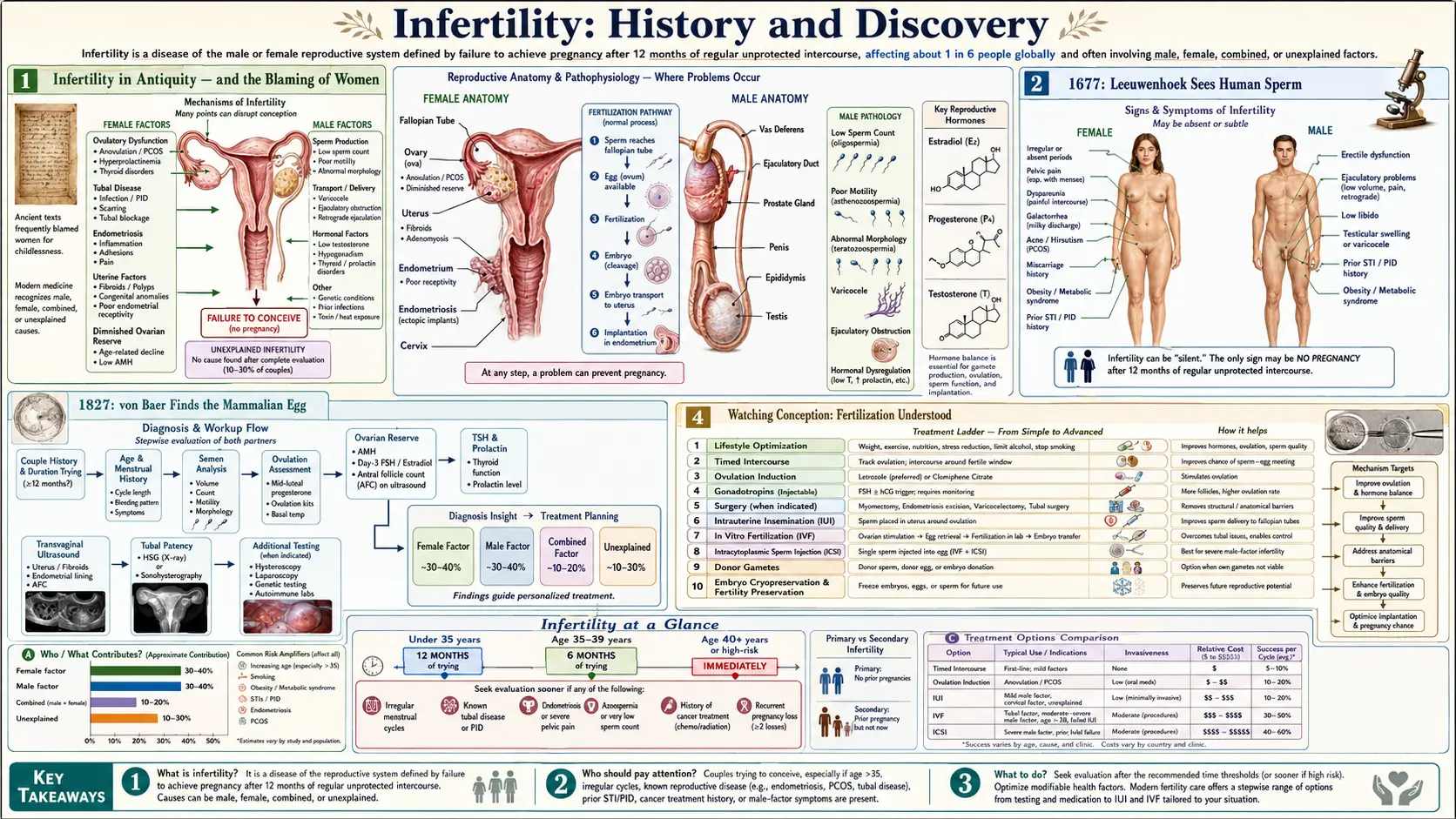
Infertility has been recognized since the earliest written records of medicine, yet for most of human history it was blamed almost entirely on women — a deep and persistent bias that shaped both how people were treated and what physicians bothered to study. We now know that male-factor infertility contributes to roughly half of all cases, but that understanding is barely a century old, and the supporting biology arrived in slow, hard-won steps. The microscopists of the 1600s and 1700s were the first to glimpse the cells involved: Antonie van Leeuwenhoek saw human sperm in 1677, and it took until 1827 for Karl Ernst von Baer to find the mammalian egg. Only in the later nineteenth century did anyone watch a sperm and an egg actually fuse. The single greatest turning point came on 25 July 1978, when Louise Joy Brown — the first baby conceived by in vitro fertilization (IVF) — was born in England, the work of Patrick Steptoe, Robert Edwards, and Jean Purdy. This page traces that long road, names its discoverers honestly, and marks clearly where the history is settled and where it is not.
Table of Contents
- Infertility in Antiquity — and the Blaming of Women
- 1677: Leeuwenhoek Sees Human Sperm
- 1827: von Baer Finds the Mammalian Egg
- Watching Conception: Fertilization Understood
- Artificial Insemination and John Hunter
- The IVF Breakthrough: Louise Brown, 1978
- After IVF: ICSI, Egg Freezing, and Male-Factor Care
- From Stigma to Science: Infertility Today
- Research Papers and References
- Connections
- Featured Videos
Infertility in Antiquity — and the Blaming of Women
Childlessness was a recognized and feared condition in the oldest medical writings we possess. The Kahun Gynaecological Papyrus from ancient Egypt — usually dated to around 1825 BCE — already contains tests meant to predict whether a woman could bear children, including the well-known scheme of moistening barley and emmer grain with a woman's urine and watching what sprouted. Egyptian medicine, notably, treated difficulty conceiving as an illness to be diagnosed and managed rather than a curse. Centuries later, Greek and Roman physicians in the Hippocratic tradition catalogued elaborate (and largely pseudoscientific) theories of why a woman's body might fail to conceive.
The honest and uncomfortable thread running through nearly all of this history is that infertility was assumed to be the woman's fault. Across most ancient societies the inability to produce children was framed as a female deficiency, with heavy social, legal, and religious consequences for the woman — grounds for divorce, abandonment, or shame. Male infertility was rarely considered, and when it appears in ancient sources it is usually only indirect. This was not a neutral oversight: it meant that for thousands of years medical inquiry, blame, and treatment were aimed almost exclusively at women, while the male contribution went unexamined.
That bias has real consequences for how we read the history of discovery. Because the field assumed the problem lived in the female body, the science of the egg, the womb, and the menstrual cycle was pursued long before anyone seriously investigated sperm quality or male reproductive disorders. Stating this plainly is not editorializing — it is simply the documented record, and it explains why the recognition that men account for roughly half of infertility had to wait until the twentieth century, even though the cells involved had been visible under a microscope since the 1600s.
1677: Leeuwenhoek Sees Human Sperm
The microscope opened the first real window onto human reproduction. The Dutch draper and self-taught microscopist Antonie van Leeuwenhoek (1632–1723), building single-lens microscopes of remarkable power, became the first person to observe human spermatozoa. In a letter to the Royal Society in London dated 1677, he described the multitude of tiny moving cells he saw in semen — the "animalcules" with a rounded head and a long, eel-like tail. (The initial observation is often credited to a student, Johan Ham, who brought a specimen to Leeuwenhoek; Leeuwenhoek made and reported the detailed observations.) Leeuwenhoek is, on the strength of this and his many other discoveries, remembered as a father of microbiology.
Seeing the sperm cell did not mean understanding it. For more than a century afterward, two camps argued bitterly over what these "animalcules" even were. The spermists believed each sperm contained a fully preformed miniature human (the fanciful "homunculus") that merely needed the womb as soil; the ovists believed the preformed individual resided in the egg. Both were versions of preformationism, and both were wrong. What mattered historically is that the male cell was now a visible, countable object — a necessary first step, even though its true role would not be settled for two hundred years.
It is worth pausing on the irony: the very cell that we now know is responsible for about half of infertility was the first reproductive cell ever seen, observed in 1677 — yet the medical assumption that infertility was a female problem persisted essentially unchallenged for another two and a half centuries.
1827: von Baer Finds the Mammalian Egg
If sperm were seen early, the mammalian egg proved remarkably elusive. The search had run since the 1600s — William Harvey had famously declared ex ovo omnia ("everything from the egg") without ever finding a mammalian one, and Regnier de Graaf in the 1670s described the ovarian follicles now named after him, mistaking the whole follicle for the egg. The true mammalian egg cell — far smaller than the follicle that contains it — was not identified until 1827, when the Baltic-German naturalist and embryologist Karl Ernst von Baer (1792–1876), then at Königsberg, found the ovum inside the ovarian follicle of a dog and recognized that the human egg followed the same plan.
Von Baer announced the discovery in a Latin letter to the St. Petersburg Academy, De ovi mammalium et hominis genesi ("On the genesis of the egg of mammals and of man"). With this, both reproductive cells were finally on the table: the sperm (1677) and the egg (1827), separated by 150 years of looking. Von Baer is also remembered as a founder of comparative embryology, and his work on how embryos develop laid groundwork that reaches into modern developmental biology.
Even now, however, the relationship between sperm and egg was unknown. Identifying both cells did not reveal that conception is the union of one sperm with one egg. That insight — the actual mechanism of fertilization — required watching it happen, which only became possible in the second half of the nineteenth century.
Watching Conception: Fertilization Understood
The decisive observations came not in humans but in sea urchins, whose eggs are produced in vast numbers and are transparent enough to watch under a microscope. In 1876, the German embryologist Oscar Hertwig (1849–1922) reported that fertilization consists of a single sperm penetrating the egg, followed by the fusion of the sperm nucleus with the egg nucleus — a single cell with one nucleus becoming, briefly, a cell with two nuclei that then merge. This established conception as the union of the two parents' germ cells, overturning older ideas that the sperm merely triggered the egg by some vibration or chemical influence. The Belgian cytologist Hermann Fol independently observed sperm entry into the egg in the same period (his detailed account of a single sperm penetrating the egg is usually dated to 1879), and the two are often credited together for establishing the picture of fertilization.
This was the conceptual keystone of reproductive biology. Once it was clear that a new individual begins when one sperm fuses with one egg, the entire framework of inheritance, embryology, and — eventually — assisted reproduction had a foundation. It also, finally, made the logic of infertility symmetrical: if conception requires a functional sperm and a functional egg meeting in a viable environment, then a failure on either side, or in between, can cause childlessness. The scientific basis for taking male-factor infertility seriously was now in place, even though clinical medicine and society would lag far behind.
Over the following decades, the discovery of chromosomes and their behaviour during fertilization and cell division filled in the details, showing how each parent contributes half of the genetic material to the offspring. By the early twentieth century, the cellular story of conception was essentially understood, setting the stage for attempts to assist or replace the natural process.
Artificial Insemination and John Hunter
Long before anyone could fertilize an egg in a laboratory, physicians attempted the simpler intervention of placing semen where it needed to go. The first widely credited human case is attributed to the Scottish surgeon and anatomist John Hunter (1728–1793), who around 1790 advised a man with a urethral abnormality (hypospadias) on how to collect his own semen and use a warmed syringe to introduce it into his wife; a pregnancy reportedly followed. This is generally described as the first reported case of successful human artificial insemination, though, as with many late-eighteenth-century medical reports, the documentation is thin and the exact date is given variously, so it is best treated as approximate.
Artificial insemination developed slowly and quietly through the nineteenth century, often surrounded by social and religious controversy, especially once donor sperm (rather than the husband's) began to be used. The technique mattered for infertility history because it was the first deliberate medical attempt to overcome a barrier to conception — and, notably, several of its early uses addressed problems on the man's side, such as anatomical defects or low fertility, quietly anticipating the modern recognition of male-factor infertility.
The twentieth century added crucial enabling technologies. The development of methods to freeze and bank sperm in the mid-twentieth century (cryopreservation using glycerol as a protectant was a key advance of the 1940s–1950s) made donor insemination practical and reliable and laid groundwork for the sperm banks that support fertility treatment today. Artificial insemination remains a first-line treatment for many couples, and it forms the conceptual bridge between simply assisting nature and the far more radical step of fertilizing an egg outside the body.
The IVF Breakthrough: Louise Brown, 1978
The landmark of modern reproductive medicine is in vitro fertilization (IVF) — fertilizing an egg with sperm in the laboratory ("in glass") and transferring the resulting early embryo to the uterus. Achieving it in humans took a long collaboration between three people in England: the gynaecologist and surgeon Patrick Steptoe (1913–1988), who pioneered the laparoscopy used to retrieve eggs; the Cambridge physiologist Robert Edwards (1925–2013), who worked out how to mature and fertilize human eggs; and the nurse and embryologist Jean Purdy (1945–1985), who managed the embryo culture and was, by Edwards's own account, the first to see the dividing embryonic cells. Purdy's essential role was long under-credited and has only recently been more fully recognized — a fitting echo of this field's long pattern of overlooking women's contributions.
Their patient, Lesley Brown, had blocked fallopian tubes and had been unable to conceive for years. After the egg-retrieval and fertilization procedure in November 1977, the pregnancy went to term, and Louise Joy Brown was born by planned caesarean section on 25 July 1978 at Oldham General Hospital — the first human being conceived by IVF. The team reported it with characteristic brevity in a short letter to The Lancet a few weeks later. The birth was a worldwide sensation, hailed as one of the great medical breakthroughs of the century and, in some quarters, fiercely debated on ethical and religious grounds.
Recognition for the science came decades later and is itself part of the historical record. In 2010, Robert Edwards was awarded the Nobel Prize in Physiology or Medicine "for the development of in vitro fertilization." The Nobel Prize is not awarded posthumously, and both Patrick Steptoe (who died in 1988) and Jean Purdy (who died in 1985) had passed away, so neither could share it; the Nobel committee and Edwards himself publicly acknowledged their indispensable contributions. Since 1978, IVF and related techniques have led to the birth of millions of children worldwide.
After IVF: ICSI, Egg Freezing, and Male-Factor Care
IVF was a platform, not an endpoint, and the decades after 1978 brought refinements that dramatically widened who could be helped — including, at last, men. Standard IVF still relies on large numbers of motile sperm finding and fertilizing the egg in the dish, so it does little for severe male-factor infertility. The answer arrived in 1992, when a team at the Vrije Universiteit Brussel led by Gianpiero Palermo, with Hubert Joris, Paul Devroey, and André Van Steirteghem, reported intracytoplasmic sperm injection (ICSI) — injecting a single sperm directly into the egg. ICSI made fatherhood possible for men with very low sperm counts, poor motility, or sperm that could only be retrieved surgically, and it rapidly became the standard treatment for male-factor infertility.
Other advances broadened reproductive options further. Techniques for freezing embryos, and later for reliably freezing unfertilized eggs (oocyte cryopreservation, greatly improved by the vitrification or "flash-freezing" methods refined in the 2000s), allowed fertility to be preserved before chemotherapy, deferred for medical or personal reasons, and used in donor-egg programmes. Preimplantation genetic testing made it possible to screen embryos for certain serious genetic conditions before transfer. Together, IVF, ICSI, and egg/embryo freezing form the core of what is now called assisted reproductive technology (ART).
These tools transformed the practical meaning of an infertility diagnosis, but they did not erase its difficulty: treatment can be physically demanding, expensive, emotionally taxing, and is never guaranteed to succeed. Their deeper historical significance is that, for the first time, medicine could directly treat male-factor infertility — the half of the problem that earlier eras had ignored — rather than placing every intervention, and every burden, on the woman.
From Stigma to Science: Infertility Today
The modern understanding of infertility is strikingly different from the one that prevailed for most of recorded history. Infertility affects a large share of couples — the World Health Organization estimates that around one in six people experience infertility at some point in their lives — and it is now firmly understood as a shared condition. Male-factor problems contribute to roughly half of all cases, whether as the sole cause or alongside female factors, and standard evaluation today investigates both partners, beginning with a semen analysis for the man as routinely as it examines ovulation and the reproductive tract in the woman.
This shift — from a moral and almost entirely female framing to a medical, evidence-based, and shared one — rests directly on the chain of discovery traced above: Leeuwenhoek's sperm, von Baer's egg, Hertwig and Fol's account of fertilization, Hunter's insemination, and the IVF and ICSI revolutions. Each step made it harder to pretend that infertility was simply a flaw in women, and easier to see it as a biological condition with many possible causes in either partner, much of it treatable.
Acknowledging the long history of blaming women is not a footnote to this story; it is central to telling it honestly. For thousands of years that bias caused real and unjust harm and slowed the science. Recognizing it openly is part of what it means to present infertility accurately today: a common, often treatable medical condition that belongs to a couple, not a failing that belongs to a woman. For current causes, diagnosis, and treatment options, see the main Infertility article.
Research Papers and References
The list below pairs the landmark primary papers of reproductive medicine — cited with real DOIs or PubMed IDs where they are confidently identified — with curated PubMed topic-search links into the historical and ethnographic literature. The ancient sources discussed above (the Kahun Gynaecological Papyrus and the Hippocratic and Greco-Roman writings) are named in the article as historical primary documents rather than as modern citations. Each link opens at the National Library of Medicine (PubMed / PMC) in a new tab.
- Steptoe PC, Edwards RG. Birth after the re-implantation of a human embryo. Lancet. 1978;2(8085):366. — PMID: 79723
- Palermo G, Joris H, Devroey P, Van Steirteghem AC. Pregnancies after intracytoplasmic injection of single spermatozoon into an oocyte. Lancet. 1992;340(8810):17-18. — PMID: 1351601
- The Nobel Prize in Physiology or Medicine 2010 (Robert G. Edwards, for the development of in vitro fertilization) — NobelPrize.org — 2010 Prize
- Spermatozoa: a historical perspective (the discovery by van Leeuwenhoek and the centuries of debate that followed) — PMC: Spermatozoa — A Historical Perspective
- Why couple infertility is historically a female-driven problem (a review of the centuries-long bias toward blaming women) — PMC: Why couple infertility is historically a female-driven problem
- Reproduction concepts and practices in ancient Egypt mirrored by modern medicine (the Kahun papyrus and early fertility testing) — PMID: 15916845
- Antonie van Leeuwenhoek and the discovery of spermatozoa — PubMed: Leeuwenhoek and the discovery of spermatozoa
- Karl Ernst von Baer and the discovery of the mammalian ovum — PubMed: von Baer and the mammalian ovum
- Oscar Hertwig, Hermann Fol, and the discovery of the mechanism of fertilization — PubMed: history of the discovery of fertilization
- History of human artificial insemination (John Hunter and after) — PubMed: history of human artificial insemination
- History and milestones of in vitro fertilization (IVF) and assisted reproduction — PubMed: history of IVF and assisted reproduction
- The pioneering and historical development of intracytoplasmic sperm injection (ICSI) — PubMed: history of ICSI
- Male-factor infertility — epidemiology and its contribution to about half of cases — PubMed: male-factor infertility epidemiology
- History of oocyte and embryo cryopreservation and fertility preservation — PubMed: history of egg and embryo freezing
External Authoritative Resources
- World Health Organization — Infertility Fact Sheet
- NobelPrize.org — Robert G. Edwards (2010, IVF)
- PubMed — History of infertility and assisted reproduction
Connections
- Reproductive Medicine
- Infertility (main article)
- All Conditions
- PCOS (Polycystic Ovary Syndrome)
- Endometriosis
- Uterine Fibroids
- Ovarian Cysts
- Menopause & HRT