COPD: History and Discovery
Chronic obstructive pulmonary disease (COPD) has no single discoverer and no single moment of invention — because COPD is not, strictly speaking, one disease that someone found. It is a modern umbrella term, coined in the mid-twentieth century, that gathers together two much older conditions: chronic bronchitis and emphysema. The umbrella is young; the rain it shelters from is ancient. The component diseases were described by anatomists in the 1600s, given clinical shape by René Laennec and the stethoscope in the early 1800s, made measurable by John Hutchinson's spirometer in 1846, and finally welded into a single, smoking-driven clinical entity by the landmark epidemiology of the 1960s and 1970s. This page traces that long road — carefully separating what was genuinely first observed by whom, from the unifying label that came much later.
Table of Contents
- An Umbrella Term, Not a Single Disease
- The Anatomists: Bonet, Ruysch, and Morgagni (1679–1769)
- Charles Badham Names "Bronchitis" (1808–1814)
- Laennec, the Stethoscope, and Emphysema (1819)
- John Hutchinson and the Spirometer (1846)
- Measuring Airflow: Tiffeneau, Pinelli, and the One-Second Breath (1947)
- Naming COPD: CIBA, the ATS, and Briscoe (1959–1965)
- A Genetic Cause: Alpha-1 Antitrypsin Deficiency (1963)
- Fletcher, Peto, and the Natural History of Decline (1977)
- Research Papers and References
- Connections
- Featured Videos
An Umbrella Term, Not a Single Disease
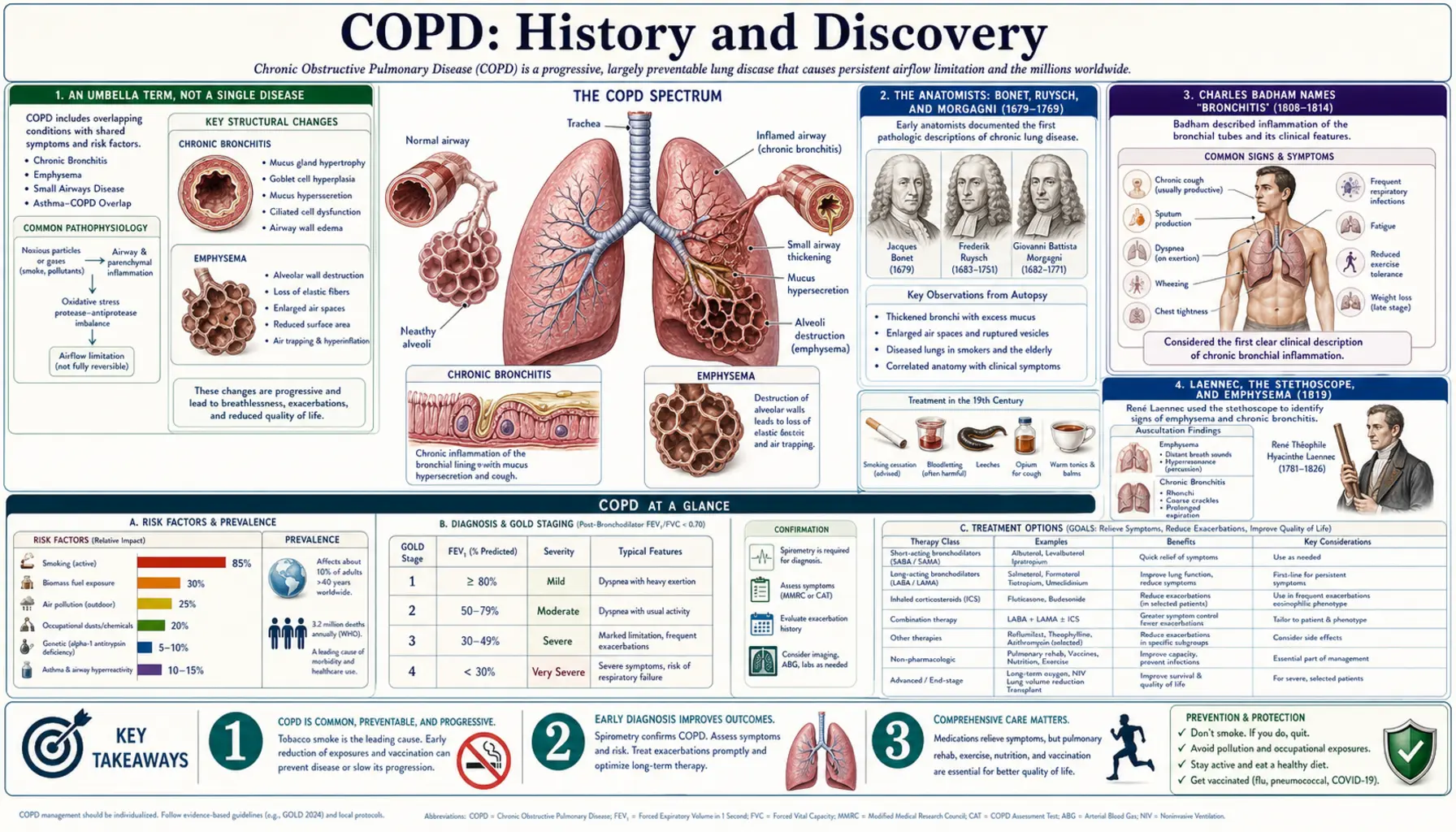
The single most important fact about the history of COPD is also the one most often blurred: "chronic obstructive pulmonary disease" is a unifying clinical concept, not a discovery. There was no Wednesday afternoon on which a physician peered down a microscope and announced the finding of COPD. Instead, two long-recognized lung conditions — chronic bronchitis (chronic cough with excess mucus from inflamed airways) and emphysema (destruction of the alveolar air sacs, leaving over-inflated, poorly elastic lungs) — were observed to overlap so often, to share the same dominant cause (tobacco smoke), and to produce the same functional problem (airflow that is obstructed and does not fully reverse) that mid-twentieth-century physicians decided to treat them as facets of one disorder.
This matters for honest history because it means the "firsts" belong to the components, not to the umbrella. Emphysema was described by anatomists in the seventeenth century and given clinical and pathological shape by René Laennec in 1819. The word "bronchitis" was coined by Charles Badham in the early nineteenth century. The tools that turned these descriptions into measurable disease — the spirometer and, later, the timed forced breath — arrived in 1846 and 1947 respectively. Only after all of that did the umbrella term itself appear, around 1959–1965. When a source says someone "discovered COPD," it is almost always shorthand for one of these narrower, datable contributions.
A second caution belongs here. The boundary of the umbrella has shifted over time. Mid-century definitions sometimes folded in asthma and even bronchiectasis under broad labels such as "chronic obstructive lung disease"; modern practice deliberately separates asthma (typically reversible airflow obstruction) from COPD (persistent, largely non-reversible obstruction), while recognizing that the two can coexist. Reading the older literature therefore requires care: the same words did not always mean the same diseases. With that framing in place, the rest of this page follows the genuine, verifiable thread of who saw what, and when.
The Anatomists: Bonet, Ruysch, and Morgagni (1679–1769)
The earliest threads of the COPD story are anatomical, recorded by the great dissectors of the seventeenth and eighteenth centuries who opened the chest after death and described what diseased lungs actually looked like. The Swiss physician Théophile Bonet (Bonetus) is generally credited as the first to describe the changes of emphysema. In his Sepulchretum of 1679 — a vast compendium of autopsy findings — he recorded lungs that were abnormally large and over-distended, the appearance later summarized in the histories as "voluminous lungs." He could describe the appearance, but the mechanism — the breakdown of the delicate air-sac walls — would not be understood for generations.
The Dutch anatomist Frederik Ruysch, celebrated for his extraordinarily preserved anatomical specimens, is also cited among the early observers of the over-inflated, emphysematous lung around the turn of the eighteenth century. The decisive figure of the era, however, was the Italian anatomist Giovanni Battista Morgagni, the founder of modern pathological anatomy. In his monumental De Sedibus et Causis Morborum ("On the Seats and Causes of Diseases") of 1769, Morgagni corroborated and extended the earlier reports, describing lungs that were "turgid" and would not collapse — among the clearest pre-modern accounts of what we now call emphysema. Histories of COPD routinely place Bonet (1679) and Morgagni (1769) as the twin anatomical anchors of the disease.
What these anatomists supplied was the raw observation: that some people die with lungs that are too big, too airy, and too stiff to deflate. They did not have the word "emphysema" in its modern clinical sense, nor any way to study the disease in a living patient. That second step — moving from the autopsy table to the bedside — required a new instrument and a new way of thinking, both of which arrived in early-nineteenth-century Paris.
Charles Badham Names "Bronchitis" (1808–1814)
If emphysema is one pillar of COPD, chronic bronchitis is the other — and we can name the man who gave it its name. The English physician Charles Badham is credited with coining the term "bronchitis" in 1808, in his work Observations on the Inflammatory Affections of the Mucous Membrane of the Bronchiae. An expanded second edition followed in 1814 under the title An Essay on Bronchitis. Badham did this notably before Laennec's great treatise, which means the vocabulary of bronchial inflammation was already in place when the stethoscope arrived.
Badham's contribution was more than a label. He distinguished bronchitis from the neighbouring chest diseases of pleurisy and pneumonia, and he separated the disease into forms — including acute and a chronic variety. He used the older word "catarrh" for the cardinal symptoms that any modern COPD patient would recognize instantly: a persistent cough and the over-production of mucus. In naming and dividing the condition, Badham described chronic bronchitis as a genuinely disabling disorder, not merely a nuisance cough — an early recognition of the long, grinding burden the disease imposes.
It is worth marking how the two halves of COPD entered medicine from different directions. Emphysema came in through the anatomist's autopsy — a structural finding in the dead. Chronic bronchitis came in through the clinician's description of symptoms — cough and phlegm in the living. For more than a century these two strands ran in parallel, studied by different methods and often by different people, before the umbrella term finally tied them together.
Laennec, the Stethoscope, and Emphysema (1819)
The physician who, more than any other, dragged emphysema out of the autopsy room and into living clinical medicine was the Frenchman René Théophile Hyacinthe Laennec (1781–1826). In 1816 Laennec invented the stethoscope — famously beginning with a rolled tube of paper to listen to a patient's chest — and with it founded the discipline of mediate auscultation, the art of diagnosing disease inside the body by the sounds it makes. He published his findings in the landmark treatise De l'Auscultation Médiate in 1819.
Laennec's genius was to connect what he heard in the living patient with what he later found at autopsy in the same patient. For emphysema, this meant pairing the physical signs — breathlessness, an over-resonant chest, faint or distant breath sounds, and wheezing — with the over-inflated, air-trapped lungs the anatomists had described. He effectively gave emphysema a recognizable clinical picture for the first time, sitting it alongside his careful descriptions of pneumonia, bronchiectasis, pleurisy, pneumothorax, and phthisis (tuberculosis). Laennec did not "discover" emphysema — Bonet and Morgagni had described it long before — but he is the figure who united its symptoms, its sounds, and its pathology into a coherent disease a doctor could identify at the bedside.
The stethoscope's arrival was a turning point for the whole future field of COPD. For the first time, a physician could gather evidence about airflow and lung structure in a breathing patient rather than waiting for a post-mortem. Laennec's instrument and method made the airways and air sacs clinically visible, so to speak, decades before any machine could put a number on how well they worked. That numerical step — measurement — was the next great advance.
John Hutchinson and the Spirometer (1846)
Description and auscultation could tell a physician that a lung was diseased; they could not say how much. The leap to measurement came from the English surgeon John Hutchinson (1811–1861), who in 1846 introduced the spirometer — the instrument that, in refined electronic form, still anchors the diagnosis of COPD today. Hutchinson adapted a common gasometer into a precise calibrated device: an inverted, water-sealed bell into which a person exhaled, so the volume of air displaced could be read off directly. His instrument stood about as tall as the patient using it.
Hutchinson's most enduring legacy is a single phrase. He named the maximum volume of air a person could expel from fully inflated lungs the "vital capacity," a term still in daily use nearly two centuries later. Working partly as a medical examiner for life-insurance applicants, Hutchinson measured the vital capacity of more than two thousand people and showed that it varied predictably with height, age, and build — establishing the powerful idea that lung volume is a measurable vital sign that can be compared against a healthy norm. A person whose measured capacity fell short of the prediction could be flagged as having diseased or weakened lungs.
What Hutchinson's spirometer could not yet capture was the dimension that defines COPD specifically: not merely how much air the lungs hold, but how fast it can be pushed out. Vital capacity measured volume; obstruction is fundamentally about the speed of airflow being throttled by narrowed, floppy airways. Bridging that gap — adding the clock to the bell — took another century.
Measuring Airflow: Tiffeneau, Pinelli, and the One-Second Breath (1947)
The decisive refinement — the one that finally let physicians quantify obstruction — came from Paris in December 1947, when Robert Tiffeneau and André Pinelli described the forced expiratory manoeuvre. Their key insight was to time the breath: instead of merely asking how much air a person could eventually exhale, they measured the maximal volume blown out in the first one second of a hard, fast exhalation after a full breath in. They called this the "pulmonary capacity usable on exercise" (capacité pulmonaire utilisable à l'effort), intended as a less exhausting substitute for older maximum-breathing tests.
This one-second measurement is the direct ancestor of FEV1 (forced expiratory volume in one second), which — expressed as a fraction of the total forced vital capacity, the FEV1/FVC ratio — remains the defining diagnostic test for COPD to this day. A reduced ratio that does not normalize after a bronchodilator is, in effect, the operational definition of the airflow obstruction that the word "obstructive" in COPD refers to. In honour of its originators, the FEV1/FVC ratio is still widely known as the Tiffeneau–Pinelli index.
A point of accuracy is owed to the historical record. The closely related English phrase "timed vital capacity" is usually attributed to the American physiologist Edward Gaensler, who introduced it in 1951; the terminology then evolved further, with "forced expiratory volume" adopted in Britain later in the decade. Tiffeneau and Pinelli's 1947 work is the conceptual origin of the timed forced breath, even though the exact term "timed vital capacity" belongs to Gaensler a few years afterward. With this tool in hand, medicine could at last measure the very thing that distinguishes COPD — and the stage was set to give the combined disease a name.
Naming COPD: CIBA, the ATS, and Briscoe (1959–1965)
By the late 1950s, clinicians had the descriptions (emphysema, chronic bronchitis), the instrument (spirometry), and the defining measurement (timed forced expiration). What they lacked was an agreed framework — and, crucially, an agreed name. The mid-century literature was a thicket of competing labels: chronic obstructive bronchopulmonary disease, chronic airflow obstruction, chronic obstructive lung disease, nonspecific chronic pulmonary disease, and diffuse obstructive pulmonary syndrome, among others. The disease was real and increasingly common; the vocabulary was chaos.
Two formal efforts began to impose order. The CIBA Guest Symposium of 1959 in London brought experts together to standardize definitions of chronic bronchitis, emphysema, and the airflow obstruction that links them — a foundational moment for the modern concept. Shortly afterward, in 1962, the American Thoracic Society's Committee on Diagnostic Standards issued its own influential definitions. Between them, these two efforts established the idea that chronic bronchitis and emphysema should be understood together as a single problem of chronic, largely irreversible airflow obstruction.
The specific term "chronic obstructive pulmonary disease" is most often credited to the American physician William A. Briscoe, who is reported to have used it at the 9th Aspen Emphysema Conference in June 1965. That label — concise, descriptive, and acronym-friendly — outcompeted its many rivals and became the standard. It is essential to read this correctly: Briscoe did not discover a disease in 1965; he is credited with popularizing the name for a disease concept that the anatomists, Laennec, Hutchinson, Tiffeneau, and the CIBA and ATS committees had spent nearly three centuries assembling. (Because attributions of a term's "first use" can vary between historical reviews, Briscoe's 1965 coinage is best stated as the widely credited account rather than an absolute, undisputed first.)
A Genetic Cause: Alpha-1 Antitrypsin Deficiency (1963)
Almost all COPD is caused by long-term exposure to inhaled irritants — overwhelmingly cigarette smoke, with biomass cooking smoke and occupational dusts also important worldwide. But a small, important minority of cases is driven by an inherited cause, and its discovery is one of the few sharply datable "firsts" in the COPD story. In 1963, the Swedish clinical chemist Carl-Bertil Laurell and the resident physician Sten Eriksson, working in Sweden (Lund / Malmö), discovered alpha-1 antitrypsin (AAT) deficiency.
The finding was a model of alert observation. While running serum protein electrophoresis on roughly 1,500 samples, Laurell and Eriksson noticed that in five of them the normal "alpha-1" protein band was missing. Following up on those few anomalous samples, they found that several of the affected patients had developed emphysema at an unusually young age, and that the trait ran in families. Their report, published in the Scandinavian Journal of Clinical and Laboratory Investigation in 1963, established that a missing protective protein could let the lungs be damaged from within.
The discovery's importance reaches well beyond the rare patients it directly explains. Alpha-1 antitrypsin normally shields lung tissue from enzymes (such as neutrophil elastase) that would otherwise digest its elastic walls; without enough of it, the alveoli are slowly destroyed — emphysema. This gave powerful support to the protease–antiprotease (or "elastase–antielastase") hypothesis of emphysema: the idea that the disease results from an imbalance between enzymes that break down lung tissue and the proteins that protect it. That mechanism — framed here as the leading explanatory hypothesis it remains — helped explain how cigarette smoke, which both recruits these destructive enzymes and impairs their inhibitors, drives the far commoner acquired form of the disease.
Fletcher, Peto, and the Natural History of Decline (1977)
The final landmark in this history is the study that, more than any other, defined what COPD does over a lifetime and nailed down its principal cause. In 1977, the British researchers Charles Fletcher and Richard Peto published The Natural History of Chronic Airflow Obstruction in the British Medical Journal, summarizing an eight-year study that followed a large group of working London men and tracked their lung function (FEV1) over time.
Their results reshaped the field. They showed that FEV1 declines gradually across everyone's adult life, but that in most non-smokers — and even many smokers — it never falls far enough to cause disabling airflow obstruction. In susceptible smokers, however, the rate of decline was steeply accelerated, marching them toward symptomatic, disabling COPD. The widely reproduced "Fletcher–Peto curve" made the message visually unforgettable: smoking drives an excess loss of lung function, and the damage already done is not recovered — but quitting at any point resets the future rate of decline back toward normal, sparing what function remains.
Just as importantly, the Fletcher–Peto study helped overturn an older idea then known as the "British hypothesis" — the proposal that recurrent chest infections with mucus (chronic bronchitis) were the main driver of progressive airflow obstruction. Their data instead pointed to cigarette smoking itself, independent of infections, as the engine of decline. This cemented the modern understanding of COPD as a largely preventable, smoking-driven disease, and it supplied the public-health rationale that still underlies every smoking-cessation message given to patients today — the single most effective intervention in the entire history of the disease.
Research Papers and References
The references below combine peer-reviewed historical reviews of COPD and its component diseases with curated PubMed topic-search links into the primary literature. Several foundational works are early-modern primary texts — Bonet's Sepulchretum (1679), Morgagni's De Sedibus et Causis Morborum (1769), Badham's essays on bronchitis (1808, 1814), and Laennec's De l'Auscultation Médiate (1819) — and are named in the article as historical sources rather than as modern citations. Each link opens at the publisher or at PubMed (National Library of Medicine) in a new tab.
- Petty TL. The history of COPD. International Journal of Chronic Obstructive Pulmonary Disease. 2006;1(1):3–14. — PMC2706597 (full text)
- Ziment I, et al. A Historical Perspective on Chronic Obstructive Pulmonary Disease: From Past to Present. Cureus / PubMed. 2023. — PubMed 37651249
- Petty TL. Early History of Chronic Obstructive Pulmonary Disease 1808–1980. COPD: Journal of COPD. 2015. — doi:10.3109/15412555.2015.1043521
- Roguin A. René Théophile Hyacinthe Laënnec (1781–1826): The Man Behind the Stethoscope. Clinical Medicine & Research. 2006;4(3):230–235. — doi:10.3121/cmr.4.3.230
- Petty TL. John Hutchinson's Mysterious Machine Revisited. Chest. 2002;121(5 Suppl):219S–223S. — doi:10.1378/chest.121.5_suppl.219S
- Yernault JC. The birth and development of the forced expiratory manoeuvre: a tribute to Robert Tiffeneau (1910–1961). European Respiratory Journal. 1997;10(12):2704–2710. — doi:10.1183/09031936.97.10122704
- Fletcher C, Peto R. The natural history of chronic airflow obstruction. British Medical Journal. 1977;1(6077):1645–1648. — doi:10.1136/bmj.1.6077.1645
- Rennard SI, Drummond MB. Early chronic obstructive pulmonary disease: definition, assessment, and prevention — Fletcher and Peto 40 years on. American Journal of Respiratory and Critical Care Medicine. 2017. — doi:10.1164/rccm.201702-0346ED
- Laurell CB, Eriksson S. The electrophoretic α1-globulin pattern of serum in α1-antitrypsin deficiency. Scandinavian Journal of Clinical and Laboratory Investigation. 1963;15:132–140. — PubMed: Laurell & Eriksson 1963
- Stoller JK, Aboussouan LS. A review of α1-antitrypsin deficiency. American Journal of Respiratory and Critical Care Medicine. 2012;185(3):246–259. — doi:10.1164/rccm.201108-1428CI
- History and origin of the term "chronic obstructive pulmonary disease" (Briscoe; Aspen Emphysema Conference; CIBA and ATS definitions). — PubMed: COPD history and terminology
- Bonet, Morgagni, and the early anatomy of emphysema ("voluminous lungs"; turgid non-collapsing lungs). — PubMed: history of emphysema pathology
- 200 years of bronchitis — Charles Badham and the naming of bronchitis (1808). — PubMed 19343614
- Protease–antiprotease (elastase–antielastase) hypothesis of emphysema. — PubMed: protease–antiprotease hypothesis
External Authoritative Resources
- GOLD — Global Initiative for Chronic Obstructive Lung Disease
- NHLBI (NIH) — COPD overview
- PubMed — All research on the history of COPD
Connections
- Pulmonology
- COPD (main article)
- Asthma
- Pneumonia
- Interstitial Lung Disease
- Pulmonary Hypertension
- Acute Respiratory Distress Syndrome
- All Conditions
- Bronchitis — acute and chronic bronchitis, one of the two older conditions the COPD umbrella gathers.