PTSD: History and Discovery
The suffering we now call post-traumatic stress disorder is far older than its name. Soldiers and survivors have carried the invisible wounds of terror, grief, and horror for as long as there have been wars and catastrophes — and across the centuries, each generation gave the condition a new label, often blaming the body, the homeland, or the individual's character before it learned to blame the trauma itself. From ancient battlefield accounts, through the "nostalgia" of homesick mercenaries, the "soldier's heart" of the American Civil War, the "shell shock" of the trenches, and the "combat fatigue" of the Second World War, the story arrives at 1980, when the diagnosis "Post-Traumatic Stress Disorder" was finally written into the psychiatric manual — driven in large part by the experiences and advocacy of Vietnam War veterans. This page tells that history with care and respect for the veterans and trauma survivors whose pain made it visible.
Table of Contents
- Trauma in the Ancient World
- Nostalgia: Hofer and the Homesick Soldier (1688)
- Soldier's Heart: Da Costa and the Civil War (1871)
- Shell Shock: The First World War (1915)
- Combat Fatigue: The Second World War
- PTSD Enters the DSM-III (1980)
- Beyond the Battlefield: A Broadening Diagnosis
- The Rise of Trauma-Focused Treatment
- Legacy: Naming the Wound
- Research Papers and References
- Connections
- Featured Videos
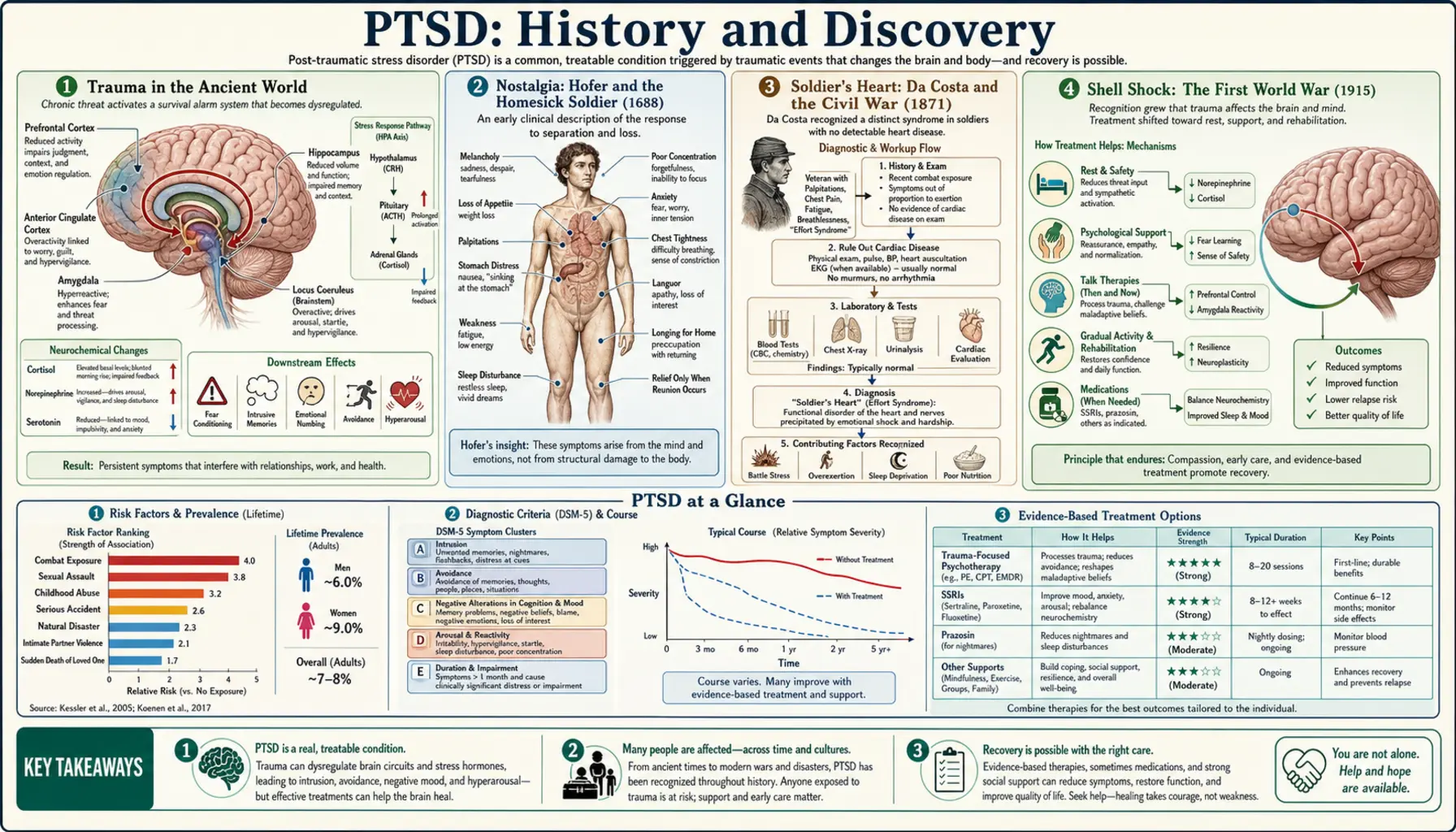
Trauma in the Ancient World
Descriptions of what looks very much like trauma response reach back to the earliest surviving literature. The Mesopotamian Epic of Gilgamesh, one of the oldest written stories known, portrays the hero overwhelmed by terror, grief, and intrusive preoccupation after witnessing the death of his companion Enkidu — a portrait of inconsolable mourning and dread that modern readers often recognize. Some scholars have also pointed to Mesopotamian and Assyrian texts (commonly dated to roughly the first millennium BCE) that record soldiers troubled by what we might now describe as flashbacks, disturbed sleep, and low mood after battle. These readings are interpretive, and historians rightly caution against simply stamping a modern diagnosis onto ancient words.
The single most-cited ancient example comes from the Greek historian Herodotus. In his account of the Battle of Marathon (490 BCE), an Athenian soldier named Epizelus was suddenly and permanently struck blind in the thick of the fighting — though he had not been wounded in the eyes or head. Epizelus himself explained it as a supernatural vision: a giant warrior had appeared, killed the man beside him, and left him sightless. Herodotus offered no medical interpretation; he reported it as a marvel of the gods. Only much later did writers propose it as perhaps the first recorded case of psychological ("conversion") blindness from the horror of combat.
The honest lesson of these ancient sources is twofold. They strongly suggest that the human mind has always been able to break under extreme terror and loss — this is not a modern weakness or invention. But they also show how every era read that breaking through its own lens: as a curse, a visitation from the gods, or a failure of courage, rather than as an injury caused by the trauma. Putting the cause where it belongs — on the event, not the person — took thousands of years.
Nostalgia: Hofer and the Homesick Soldier (1688)
The first attempt to name the condition as a medical illness came in 1688 from a young Swiss physician, Johannes Hofer. In his medical dissertation he coined the word nostalgia — joining the Greek nostos (a return home) and algos (pain) — to describe a debilitating, sometimes fatal homesickness he observed in Swiss mercenary soldiers serving far from their alpine valleys. The afflicted men wasted away with despondency, loss of appetite, weakness, palpitations, fever, and obsessive longing for home; some, it was reported, declined until they died.
For the next two centuries, "nostalgia" remained a recognized clinical category, diagnosed among soldiers, sailors, and displaced people across Europe and, later, in the armies of the American Civil War. Military physicians debated its cause — some blamed the thin mountain air or even the sound of Swiss cowbells, others a weak or sentimental temperament — and treatments ranged from sending the soldier home to harsh measures meant to shame the longing out of him. The framing was telling: the suffering was attributed to missing home, a yearning of the heart and mind, rather than to the terror and carnage of war itself.
Hofer's nostalgia matters in this history not because it was correct — it conflated homesickness with the deeper wound of trauma — but because it was a genuine first: an effort to lift the soldier's anguish out of the realm of cowardice or the supernatural and treat it as a condition a doctor could observe, name, and study. It was the opening move in a long, halting progression toward the modern understanding.
Soldier's Heart: Da Costa and the Civil War (1871)
During and after the American Civil War, physicians noticed a striking pattern among soldiers: a cluster of physical symptoms centered on the heart, appearing in men with no detectable heart disease. The Philadelphia physician Jacob Mendez Da Costa studied hundreds of such soldiers and, in 1871, published his landmark paper On Irritable Heart: A Clinical Study of a Form of Functional Cardiac Disorder and Its Consequences. He described pounding and racing heartbeat, chest pain, breathlessness, dizziness, fatigue on exertion, and sweating — a syndrome that came to be called "irritable heart," "soldier's heart," and later Da Costa's syndrome.
Da Costa framed the disorder as a functional cardiac problem — a disturbance of the heart's nervous regulation — rather than as psychological trauma, and the era's focus stayed firmly on the chest and circulation. Yet his careful description captured exactly the bodily storm of hyperarousal that we now understand as a core part of the trauma response: the racing heart, the panic, the exhaustion, the sense of physical breakdown in men who had survived the unbearable. It is now widely regarded as an important historical milestone on the road to recognizing PTSD, even though Da Costa himself did not interpret it that way.
The lineage that runs forward from "soldier's heart" is direct and well documented: through the "effort syndrome" and "neurocirculatory asthenia" of the First World War, and onward into twentieth-century concepts of anxiety and stress. Da Costa's great contribution was to take the soldier's suffering seriously as a real, observable, reproducible clinical entity — even if the field would need another century to locate its source in the mind's response to terror rather than in the heart alone.
Shell Shock: The First World War (1915)
The industrialized slaughter of the First World War produced psychological casualties on a scale that could no longer be ignored. Men emerged from the trenches mute, blind, paralyzed, amnesic, or shaking uncontrollably, often with no physical wound at all. The term that attached itself to this suffering was "shell shock." It was popularized in the medical literature by the British psychologist Charles S. Myers, whose paper in The Lancet in 1915 described three soldiers with strikingly similar symptoms after exposure to exploding shells. Myers himself later acknowledged that he did not invent the phrase — it had already arisen in the everyday speech of the soldiers in the trenches — and he came to regret the term, because it wrongly implied the cause was always the physical blast.
That ambiguity sat at the heart of the wartime debate. Was "shell shock" a physical injury — microscopic damage to the brain and nerves from the concussion of artillery — or was it a psychological collapse under unrelenting fear and horror? The distinction was not academic: it shaped whether a suffering soldier was treated with sympathy and care, dismissed as a malingerer, or, in the war's harshest episodes, punished. Over the course of the war it became increasingly clear that many men with no blast exposure at all developed identical symptoms, pushing the understanding toward the psychological.
Shell shock was the moment trauma response entered mass public consciousness. Hundreds of thousands of cases across all the warring nations made it impossible to frame the condition as rare cowardice. It spurred the growth of military psychiatry, forward treatment near the front, and a lasting cultural memory — the "shell-shocked" soldier — that still shapes how the public pictures the wounds of war. The term endured, imperfectly, as the standard name for combat trauma for a generation.
Combat Fatigue: The Second World War
By the Second World War, the favored language had shifted again. British and American military medicine increasingly spoke of "combat fatigue," "battle fatigue," and "combat stress reaction." The new vocabulary reflected a new theory: that breakdown was driven by the cumulative exhaustion of prolonged exposure to combat — that every soldier had a limit, and that enough days of fear, sleeplessness, and carnage would eventually overwhelm even the bravest and most stable man. This was, in its way, a more compassionate and democratic idea than "shell shock," because it located the cause in the unbearable conditions rather than in a defect of the individual.
Military psychiatry matured considerably during and after the war. Clinicians emphasized treating exhausted soldiers quickly and close to the front, with rest, food, and reassurance, in the expectation that many could recover — principles often summarized by the watchwords of proximity, immediacy, and expectancy. At the same time, the war exposed the limits of the "just fatigue" framing: many veterans returned home and went on suffering for years with nightmares, flashbacks, irritability, emotional numbness, and the inability to settle back into ordinary life, long after any reasonable "fatigue" should have lifted.
The aftermath of the Second World War — together with the experiences of Holocaust survivors and, in the United States, of returning veterans — planted the seeds of the modern view. It was becoming undeniable that overwhelming trauma could leave a lasting imprint that outlived the danger itself. The pieces were assembling: the bodily arousal Da Costa saw, the psychological collapse the shell-shock debate revealed, and now the recognition that the wound could become chronic. What was still missing was a single, unified name and definition.
PTSD Enters the DSM-III (1980)
The decisive turn came after the Vietnam War. Large numbers of returning American veterans struggled with persistent nightmares, flashbacks, hypervigilance, emotional numbing, survivor guilt, and difficulty reintegrating into civilian life — a pattern then informally described as "post-Vietnam syndrome." Veterans themselves, working alongside sympathetic psychiatrists and through anti-war and veterans' advocacy, pressed hard for the medical establishment to formally recognize their suffering as a legitimate, trauma-caused condition rather than as personal weakness or pre-existing mental illness.
Their advocacy converged with research on other survivor groups — Holocaust survivors, survivors of disasters, and survivors of rape, assault, and child abuse — all of whom showed remarkably similar long-term reactions. This convergence of evidence persuaded the American Psychiatric Association, and in 1980 the diagnosis Post-Traumatic Stress Disorder was formally introduced in the third edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-III). For the first time, a single named diagnosis united the scattered historical threads — nostalgia, soldier's heart, shell shock, combat fatigue — under one definition.
The conceptual breakthrough of the DSM-III definition was profound: it placed the cause of the disorder outside the individual, in an identifiable traumatic event, rather than treating the symptoms as a sign of inherent personal frailty. The injury came from what happened to the person, not from who they were. This reframing — hard-won and substantially driven by Vietnam veterans' insistence on being heard — is the foundation of everything in modern trauma care, and it is why 1980 stands as the true birth year of PTSD as we know it.
Beyond the Battlefield: A Broadening Diagnosis
Although PTSD was forged largely in the experience of soldiers, the diagnosis was never limited to combat — and it broadened steadily in the decades after 1980. Clinicians and researchers recognized the same core syndrome in survivors of sexual assault and rape, childhood abuse, domestic violence, serious accidents, natural disasters, terrorism, torture, and life-threatening medical events. The wound, it turned out, was about the encounter with overwhelming horror or threat, whatever its source. This broadening was one of the most important and humane consequences of naming the condition: it extended recognition and care to millions of trauma survivors who had never worn a uniform.
Successive revisions of the manual refined the definition. A significant change arrived with the DSM-5 in 2013, which moved PTSD out of the "anxiety disorders" category and into a newly created group of trauma- and stressor-related disorders — a recognition that PTSD is not purely a fear-and-anxiety condition but also involves persistent negative changes in mood and thinking, and disturbances of behavior. The criteria for what counts as a qualifying traumatic event, and the catalogue of symptoms, were also revised and clarified.
This widening came with genuine scientific debate — over how broadly "trauma" should be defined, and how to draw the line between normal, expected distress after a terrible event and a diagnosable disorder. Those debates continue, and they are healthy: they reflect a field trying to honor real suffering without medicalizing ordinary grief and fear. What is not in doubt is the central insight that the historical record had been circling for millennia — that catastrophic experience can leave lasting, treatable wounds in the mind, in soldiers and civilians alike.
The Rise of Trauma-Focused Treatment
Naming PTSD did more than validate suffering — it opened the door to developing and testing specific treatments, something the older, blurrier labels had never made possible. The most strongly evidence-supported approaches are the trauma-focused psychotherapies, which help a person process the traumatic memory rather than avoid it. Prolonged Exposure (PE) therapy, developed by psychologist Edna Foa and colleagues beginning in the 1980s, works by gradually and safely guiding survivors to confront trauma-related memories and situations until they lose their overwhelming power. Cognitive Processing Therapy (CPT) and other forms of trauma-focused cognitive behavioral therapy help survivors identify and rework the painful, often distorted beliefs that trauma leaves behind.
A distinctive and widely used approach is Eye Movement Desensitization and Reprocessing (EMDR), developed by psychologist Francine Shapiro, who first reported the method in 1989. In EMDR, the patient recalls distressing material while engaging in guided side-to-side eye movements or other bilateral stimulation; with repetition, the memory's emotional charge tends to diminish. The precise mechanism remains a subject of ongoing research and discussion, but multiple major clinical guidelines — including those used by veterans' health services and professional psychiatric bodies — now recommend EMDR as an effective treatment for PTSD.
Alongside these psychotherapies, certain medications — notably some SSRI and SNRI antidepressants — are established options that can reduce symptoms, and research continues into newer pharmacological and combined approaches. The arc of treatment mirrors the arc of the diagnosis: from the despairing era when the suffering had no name and no remedy, to a present in which trauma is understood as an injury that can be specifically and effectively treated, and from which many people genuinely recover. (For current treatment detail, see the main PTSD page; this page covers the history.)
Legacy: Naming the Wound
The history of PTSD is, at its core, the long struggle to see clearly what was always there. For most of recorded time, the agony of the traumatized was misread — as a divine curse, a wasting homesickness, a faulty heart, a defect of nerve, or a temporary fatigue. Each of those labels carried, to some degree, a hidden judgment about the sufferer. The 1980 diagnosis broke that pattern by putting responsibility where it belongs: on the overwhelming event, not on the wounded person. That single shift transformed shame into legitimacy and opened the way to treatment and respect.
This history also reframes a persistent and harmful myth — that trauma reactions are a modern indulgence or a sign of a softer generation. The opposite is true. The fact that ancient epics, Renaissance physicians, Civil War surgeons, and twentieth-century psychiatrists all independently described the same constellation of suffering tells us this is a deep and universal feature of the human response to horror. Soldiers at Marathon, mercenaries in the Alps, the wounded of the trenches, and survivors of the Holocaust and of personal violence all suffered something real, and they suffered it long before anyone had the right word for it.
For the veterans and trauma survivors whose pain and persistence finally forced the diagnosis into being, the history is more than academic. It is a story of being believed at last. Understanding where the diagnosis came from — and how hard it was won — is part of honoring them, and part of making sure that no one's suffering is dismissed again for want of a name.
Research Papers and References
The references below combine peer-reviewed historical scholarship with curated PubMed topic-search links into the literature on the history of PTSD and combat-trauma diagnoses. Historical primary sources — Herodotus' Histories, the Epic of Gilgamesh, Hofer's 1688 dissertation on nostalgia, Da Costa's 1871 paper, and Myers' 1915 Lancet article — are named in the article as historical sources. Each search link opens at PubMed (National Library of Medicine) in a new tab.
- Crocq MA, Crocq L. From shell shock and war neurosis to posttraumatic stress disorder: a history of psychotraumatology. Dialogues in Clinical Neuroscience. 2000;2(1):47-55. — doi:10.31887/DCNS.2000.2.1/macrocq
- Jones E, Wessely S. A paradigm shift in the conceptualization of psychological trauma in the 20th century. Journal of Anxiety Disorders. 2007;21(2):164-175. — doi:10.1016/j.janxdis.2006.09.009
- Friedman MJ, Resick PA, Bryant RA, Brewin CR. Considering PTSD for DSM-5. Depression and Anxiety. 2011;28(9):750-769. — doi:10.1002/da.20767
- Andreasen NC. Posttraumatic stress disorder: a history and a critique. Annals of the New York Academy of Sciences. 2010;1208:67-71. — doi:10.1111/j.1749-6632.2010.05699.x
- Wooley CF. Jacob Mendez Da Costa: medical teacher, clinician, and clinical investigator. American Journal of Cardiology. 1982;50(5):1145-1148. — doi:10.1016/0002-9149(82)90431-2
- Shapiro F. Eye movement desensitization: a new treatment for post-traumatic stress disorder. Journal of Behavior Therapy and Experimental Psychiatry. 1989;20(3):211-217. — doi:10.1016/0005-7916(89)90025-6
- Hofer, Johannes — "nostalgia" (1688) and the history of the concept — PubMed: Hofer, nostalgia, and homesickness in soldiers
- Da Costa's syndrome / irritable heart / soldier's heart — history — PubMed: Da Costa syndrome and irritable heart
- Shell shock, war neurosis, and the First World War — PubMed: shell shock and war neurosis
- Combat fatigue, battle fatigue, and combat stress reaction — PubMed: combat and battle fatigue
- History of PTSD, Vietnam veterans, and the DSM-III — PubMed: PTSD history and the DSM-III
- PTSD in the ancient world — Epizelus, Herodotus, Gilgamesh — PubMed: PTSD and the ancient world
- Prolonged exposure and trauma-focused cognitive behavioral therapy for PTSD — PubMed: prolonged exposure and trauma-focused CBT
- EMDR for post-traumatic stress disorder — efficacy and history — PubMed: EMDR for PTSD
External Authoritative Resources
- U.S. Department of Veterans Affairs — National Center for PTSD: History of PTSD in Veterans
- National Institute of Mental Health (NIMH) — Post-Traumatic Stress Disorder
- PubMed — All research on the history of PTSD
Connections
- Psychiatry
- PTSD (Post-Traumatic Stress Disorder)
- All Conditions
- Anxiety
- Depression
- Obsessive-Compulsive Disorder (OCD)
- Insomnia
- Grief