Loneliness: History and Discovery
Loneliness is the distressing feeling that arises from a gap between the social connection a person wants and the connection they actually have. It is important to be clear from the outset: loneliness is not itself a medical disease. It is a feeling — a normal human emotion — and, when it becomes chronic, a recognised risk factor for poorer physical and mental health, much as smoking or high blood pressure are risk factors. This page traces how the very idea of loneliness came into being (historians argue the modern emotional sense is only about two centuries old), how social neuroscientists came to understand it as an evolved biological signal, how meta-analyses linked it to mortality, and how governments began treating it as a public-health concern. Throughout, claims about a discoverer, a date, or a “first” are stated only where they can be supported by sources, and an unresolved scientific idea is labelled a hypothesis, not a fact.
Table of Contents
- A Feeling, Not a Disease: Why Framing Matters
- The Word and the Concept: From “Oneliness” to “Loneliness”
- Modernity and the Birth of a Modern Emotion
- Naming and Measuring Loneliness in the 20th Century
- John Cacioppo and the Evolutionary Theory of Loneliness
- Holt-Lunstad and Loneliness as a Mortality Risk Factor
- From Private Feeling to Public Health: Ministers and Advisories
- What the History Does and Does Not Tell Us
- Research Papers and References
- Connections
- Featured Videos
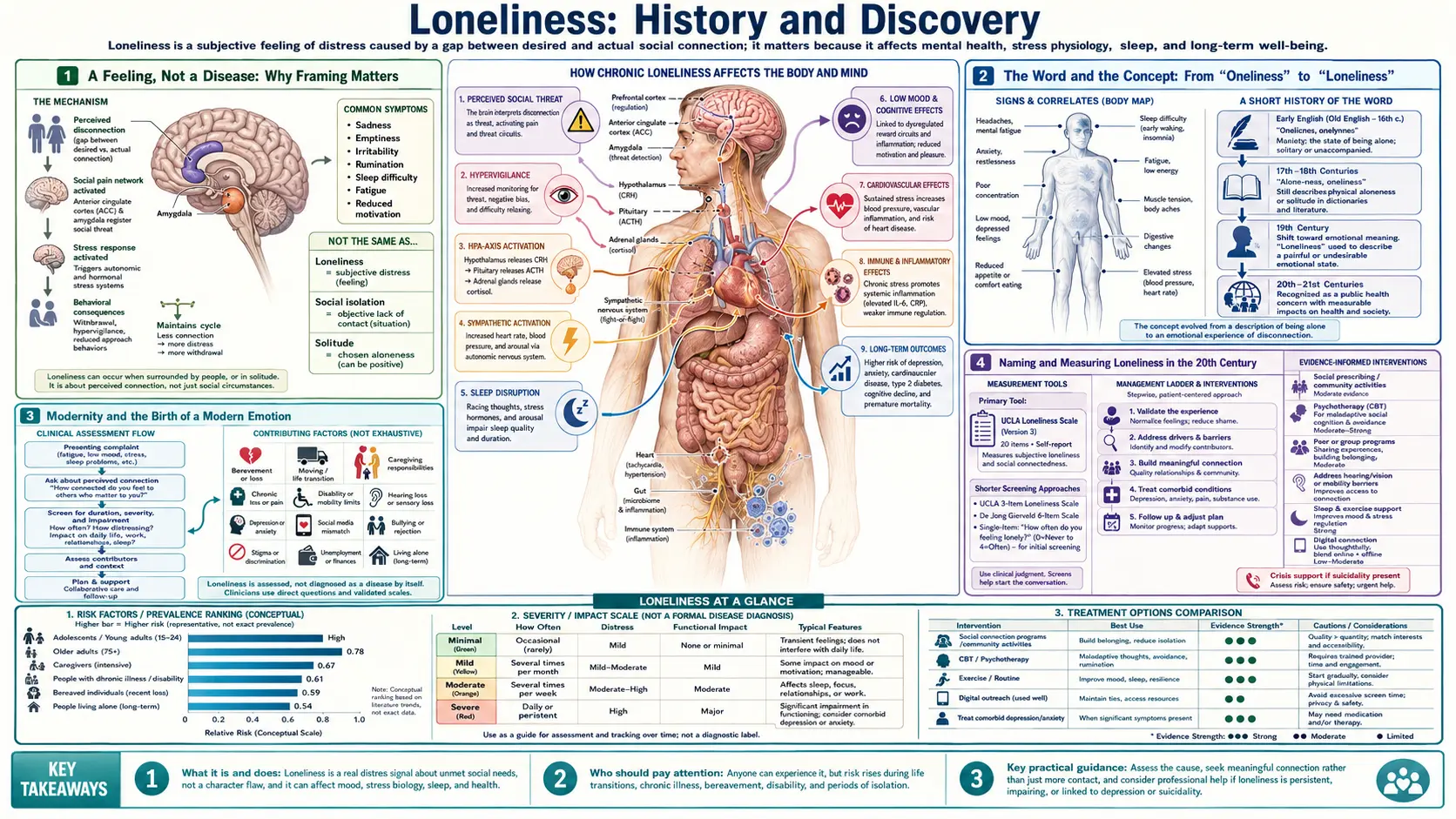
A Feeling, Not a Disease: Why Framing Matters
Before any history, the framing has to be honest, because real people who feel lonely read pages like this one. Loneliness does not appear as a diagnosable disease in the standard medical classifications. It is not a condition in the same sense that pneumonia or diabetes is. It is a subjective feeling — the painful sense that one's social relationships are fewer or shallower than one wants — and it is increasingly described in public-health language as a social determinant of health or a risk factor. That distinction is not a technicality. Calling loneliness a “disease” can make a normal, universal human experience feel like a personal pathology, which is both inaccurate and unkind.
Researchers are careful to separate two related but different things. Loneliness is the felt, subjective experience of inadequate connection; a person can feel deeply lonely in a crowd or in a marriage. Social isolation is the objective, measurable fact of having few social contacts; a person can be objectively isolated yet content. The two often travel together and both have been linked to health outcomes, but they are not the same, and good science keeps them apart. Much of the confusion in popular writing about a loneliness “epidemic” comes from blurring the feeling with the fact.
With that framing in place, the story that follows is genuinely surprising: the emotion we now treat as timeless and universal may, as an idea with its modern negative charge, be only a couple of centuries old — and the scientific recognition that chronic loneliness measurably harms the body is younger still, mostly a product of the last quarter-century.
The Word and the Concept: From “Oneliness” to “Loneliness”
One of the most influential modern arguments about loneliness is historical rather than medical. The cultural historian Fay Bound Alberti, in her book A Biography of Loneliness: The History of an Emotion (Oxford University Press, 2019), argues that loneliness in its modern emotional sense — a painful, negative state of lacking connection — is a relatively recent invention, one that she dates to roughly 1800. On her account, what earlier English speakers described was oneliness: the simple, neutral state of being alone or physically apart from others, carrying no necessary emotional sting.
The shift, Alberti contends, was from a neutral fact (being by oneself) to a charged feeling (suffering from the absence of others). In earlier centuries a person could be alone — in prayer, in the countryside, in solitude — without that aloneness automatically being read as a deficiency or a wound. The word “loneliness” gradually absorbed the modern sense of missing something one ought to have. This is a scholarly historical thesis, well-argued and widely cited, but it is an interpretation of language and culture, not a law of nature; it is presented here as Alberti's argument, which other historians of emotion engage with and sometimes qualify.
Why does an etymological point matter on a health page? Because it cautions against treating loneliness as a fixed, biological constant that has always meant the same thing. If the very concept has a history, then so do the social conditions that produce it — which is precisely why later chapters of this story move from philology to neuroscience to public policy.
Modernity and the Birth of a Modern Emotion
Alberti and other historians of emotion tie the emergence of modern loneliness to the broad transformation usually labelled modernity: the urbanisation, industrialisation, and reorganisation of life that accelerated across the eighteenth and nineteenth centuries. As people moved from tightly woven rural villages into anonymous cities, as extended households gave way to smaller family units, and as wage labour replaced older communal economies, the dense web of obligatory social ties that had surrounded most lives began to loosen.
A second strand of the argument concerns the rise of individualism — the increasingly central idea, visible in philosophy, religion, politics, and economics, of the self as a separate, self-determining unit. The decline of certain shared religious frameworks and the elevation of personal choice and personal feeling, the argument goes, made the absence of close connection something that could be experienced as a private, internal lack rather than simply a social circumstance. In this reading, loneliness is partly a side-effect of a culture that prizes the autonomous individual.
This is, again, a historical interpretation rather than a settled fact, and it should be read as such: it is a persuasive account of why the emotion may have crystallised when it did, not a demonstration that no one ever felt isolated before 1800. People in every era have written of grief, exile, longing, and abandonment. The specific claim is narrower and more careful — that the particular modern concept of “loneliness,” with its negative emotional charge and its sense of a connection one is owed, took shape alongside the modern world.
Naming and Measuring Loneliness in the 20th Century
If the nineteenth century gave loneliness its modern emotional meaning, the twentieth century tried to define and measure it. Psychologists and sociologists increasingly treated loneliness as a discrete experience worth studying rather than a vague mood. A landmark in popular and scholarly awareness was the sociologist David Riesman's widely-read The Lonely Crowd (1950), which used loneliness as a lens on the conformity and isolation of modern mass society — evidence that, by mid-century, loneliness had become a recognised theme of social analysis, not merely a private complaint.
The decisive methodological step was the creation of a reliable way to measure the feeling. The most influential instrument is the UCLA Loneliness Scale, first published by Daniel Russell, Letitia Anne Peplau, and colleagues in 1978 and revised in 1980 and again (the widely used Version 3) in 1996. By giving researchers a validated, repeatable questionnaire, the UCLA scale turned loneliness from an impression into a quantity that could be compared across people and correlated with health outcomes — the essential precondition for everything that followed. Peplau and Perlman's theoretical work in the early 1980s also helped formalise loneliness as the perceived gap between desired and actual relationships, the definition still used today.
This measurement revolution is easy to overlook but historically pivotal. Without a trusted scale, the later large-scale epidemiology — the meta-analyses linking loneliness to mortality, the population surveys behind government advisories — would not have been possible. The unglamorous work of building and validating a questionnaire is what allowed loneliness to enter the domain of public health.
John Cacioppo and the Evolutionary Theory of Loneliness
The figure most associated with the modern biological study of loneliness is the University of Chicago social neuroscientist John T. Cacioppo (1951–2018), often called a founder of the field of social neuroscience. Beginning in the early 2000s, Cacioppo and his collaborators — including Louise Hawkley and, in his popular writing, the science writer William Patrick — reframed loneliness not as mere sadness or weakness but as an evolved biological signal. Their general-audience synthesis appeared in the book Loneliness: Human Nature and the Need for Social Connection (W. W. Norton, 2008).
The core idea is the Evolutionary Theory of Loneliness (ETL), developed by Cacioppo and colleagues over the 2000s and 2010s and laid out at length by John and Stephanie Cacioppo in “Loneliness in the Modern Age: An Evolutionary Theory of Loneliness” (Advances in Experimental Social Psychology, 2018). The theory proposes that loneliness functions like physical pain or hunger: an unpleasant warning signal that motivated our highly social ancestors to repair or replace frayed connections. Because early humans survived through cooperation and group protection rather than individual strength, a felt cost to social disconnection would have been adaptive — nudging people back toward the safety of the group. This evolutionary account is a well-developed scientific hypothesis about why loneliness hurts; it is influential and supported by converging evidence, but, like all evolutionary-psychological explanations, it is a framework for interpretation rather than a directly proven historical fact, and it is presented here as such.
What is more firmly established from Cacioppo's programme of empirical work is that chronic loneliness is associated with measurable biological changes — in stress physiology, sleep, inflammation, and immune-related gene expression — and that, in longitudinal studies, loneliness can precede and predict later depressive symptoms rather than simply accompanying them. His central, durable contribution was to move loneliness out of the realm of mere mood and into biology and health, establishing it as a serious object of medical and neuroscientific study.
Holt-Lunstad and Loneliness as a Mortality Risk Factor
If Cacioppo supplied the mechanism, the psychologist Julianne Holt-Lunstad of Brigham Young University supplied the epidemiological weight. In a 2010 meta-analysis published in PLoS Medicine — “Social Relationships and Mortality Risk: A Meta-Analytic Review,” with Timothy Smith and J. Bradley Layton — she and her colleagues pooled 148 studies covering more than 300,000 participants and found that people with stronger social relationships had roughly a 50% greater likelihood of survival over the study periods (odds ratio about 1.5). Crucially, they reported that the effect of social connection on mortality was comparable to well-established risk factors such as smoking, and exceeded risks such as obesity and physical inactivity.
A second, frequently-cited 2015 meta-analysis in Perspectives on Psychological Science — “Loneliness and Social Isolation as Risk Factors for Mortality,” with Smith, Baker, Harris, and Stephenson — focused specifically on loneliness, social isolation, and living alone. It found each was associated with a meaningfully increased likelihood of death (on the order of 26–32% in the pooled estimates) even after statistical adjustment. Together these two papers are the empirical backbone of the now-common claim that loneliness and isolation carry health risks on a par with classic medical risk factors.
Two honest caveats belong here. First, these are observational, correlational findings: they show a strong and consistent association between social disconnection and earlier death, but a meta-analysis of observational studies cannot by itself prove that loneliness directly causes mortality, and researchers including Holt-Lunstad are careful about that boundary. Second, the widely-repeated “equivalent to smoking 15 cigarettes a day” figure is a vivid communication device drawn from comparing effect sizes; it conveys that the risk is substantial, but it should be read as an illustrative comparison rather than a precise biological equivalence. The serious, well-supported message is simpler: chronic loneliness and isolation are real risk factors for poor health, worth taking seriously at both the personal and the population level.
From Private Feeling to Public Health: Ministers and Advisories
By the 2010s, the accumulating evidence began to move loneliness from clinics and laboratories into government policy. In the United Kingdom, the catalyst was the murdered Member of Parliament Jo Cox, who before her death in 2016 had championed action on loneliness; the cross-party Jo Cox Commission on Loneliness carried that work forward. In January 2018 the UK government appointed Tracey Crouch as the ministerial lead for loneliness — widely reported as the world's first such role, the “Minister for Loneliness” — and in October 2018 published a national loneliness strategy, the first of its kind by a national government.
In the United States, the milestone came in May 2023, when Surgeon General Vivek Murthy issued a formal advisory titled Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General's Advisory on the Healing Effects of Social Connection and Community. The 80-plus-page advisory characterised widespread loneliness and isolation as a public-health concern, summarised the evidence linking social disconnection to cardiovascular disease, dementia, depression, and premature death, and proposed a national framework for strengthening social connection. A Surgeon General's advisory is a tool reserved for issues judged to need the nation's urgent attention — the same mechanism used historically for tobacco — which signalled how seriously loneliness had come to be taken.
These policy steps are themselves part of the history, and they should be read carefully. Naming loneliness an “epidemic” is a rhetorical and policy choice meant to mobilise attention; it does not convert a feeling into an infectious disease. What the UK ministry and the US advisory genuinely represent is official recognition that chronic loneliness and isolation are legitimate public-health risk factors deserving coordinated response — a remarkable destination for an emotion that, as a named concept, may be only about two hundred years old.
What the History Does and Does Not Tell Us
Pulling the threads together, the history of loneliness is really three intertwined histories. The first is a history of language and culture: the argument, associated with Fay Bound Alberti, that the modern emotional concept of loneliness emerged around 1800 out of an older, neutral “oneliness,” as modernity and individualism reshaped how people experienced being apart. The second is a history of science: the twentieth-century work to define and measure loneliness, and the twenty-first-century discovery — led by John Cacioppo's social neuroscience and Julianne Holt-Lunstad's meta-analyses — that chronic loneliness behaves like a genuine risk factor for illness and earlier death. The third is a history of policy: loneliness becoming, within the past decade, the subject of a national minister and a Surgeon General's advisory.
What this history does not tell us is equally important. It does not tell us that loneliness is a disease — it is a feeling and a risk factor, and presenting it otherwise would be inaccurate. It does not tell us that everyone who is alone is unwell, or that solitude is harmful; chosen solitude can be restorative, and the harm in the evidence concerns chronic, unwanted disconnection. And it does not tell us, from the observational data alone, the exact size of loneliness's causal contribution to any one person's health. The evolutionary account of why loneliness hurts remains a hypothesis, however well-supported.
The honest, encouraging takeaway is this: loneliness is a normal human signal, not a personal failing, and the same modern science that measured its costs also points to its remedy — rebuilding genuine social connection. Anyone whose loneliness is persistent and accompanied by low mood, hopelessness, sleeplessness, or thoughts of self-harm should reach out to a clinician, because the conditions loneliness travels with — including depression and anxiety — are real, common, and treatable.
Research Papers and References
The list below combines key peer-reviewed papers on loneliness as a health risk factor and on its scientific theory with curated PubMed topic-search links into the wider literature, plus the historical and policy sources named in the article. Where a confident DOI or PMID is available it is given; otherwise a PubMed topic search is provided. Each link opens in a new tab.
- Holt-Lunstad J, Smith TB, Layton JB. Social Relationships and Mortality Risk: A Meta-Analytic Review. PLoS Medicine. 2010;7(7):e1000316. — doi:10.1371/journal.pmed.1000316 (PMID: 20668659)
- Holt-Lunstad J, Smith TB, Baker M, Harris T, Stephenson D. Loneliness and Social Isolation as Risk Factors for Mortality: A Meta-Analytic Review. Perspectives on Psychological Science. 2015;10(2):227-237. — doi:10.1177/1745691614568352 (PMID: 25910392)
- Cacioppo JT, Cacioppo S. Loneliness in the Modern Age: An Evolutionary Theory of Loneliness (ETL). Advances in Experimental Social Psychology. 2018;58:127-197. — doi:10.1016/bs.aesp.2018.03.003
- Cacioppo JT, Hughes ME, Waite LJ, Hawkley LC, Thisted RA. Loneliness as a Specific Risk Factor for Depressive Symptoms: Cross-Sectional and Longitudinal Analyses. Psychology and Aging. 2006;21(1):140-151. — doi:10.1037/0882-7974.21.1.140 (PMID: 16594799)
- Hawkley LC, Cacioppo JT. Loneliness Matters: A Theoretical and Empirical Review of Consequences and Mechanisms. Annals of Behavioral Medicine. 2010;40(2):218-227. — doi:10.1007/s12160-010-9210-8 (PMID: 20652462)
- Russell D, Peplau LA, Cutrona CE. The Revised UCLA Loneliness Scale: Concurrent and Discriminant Validity Evidence. Journal of Personality and Social Psychology. 1980;39(3):472-480. — doi:10.1037/0022-3514.39.3.472 (PMID: 7431205)
- Holt-Lunstad J. The Potential Public Health Relevance of Social Isolation and Loneliness: Prevalence, Epidemiology, and Risk Factors. Public Policy & Aging Report. PubMed: Holt-Lunstad social isolation loneliness public health
- Office of the U.S. Surgeon General. Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General's Advisory on the Healing Effects of Social Connection and Community (2023). — Search PubMed
- Loneliness, social isolation, and inflammation / immune function PubMed: loneliness, isolation, inflammation and immune function
- Loneliness and risk of cardiovascular disease and stroke PubMed: loneliness, isolation and cardiovascular disease
- Loneliness, social isolation and risk of dementia and cognitive decline PubMed: loneliness, isolation and dementia risk
- Loneliness and depression: longitudinal and bidirectional studies PubMed: loneliness and depression (longitudinal)
- Interventions to reduce loneliness — effectiveness reviews PubMed: interventions to reduce loneliness
- History, concept, and measurement of loneliness PubMed: loneliness concept, history and measurement
External Authoritative Resources
- U.S. Surgeon General — Our Epidemic of Loneliness and Isolation (2023 advisory, full PDF)
- CDC — Social Connectedness and Health
- World Health Organization — Social Isolation and Loneliness
Connections
- Psychiatry
- Loneliness (Health Effects & Evidence)
- Depression
- Anxiety
- Grief
- Dementia
- Insomnia & Sleep Disorders
- All Conditions