Insomnia: History and Discovery
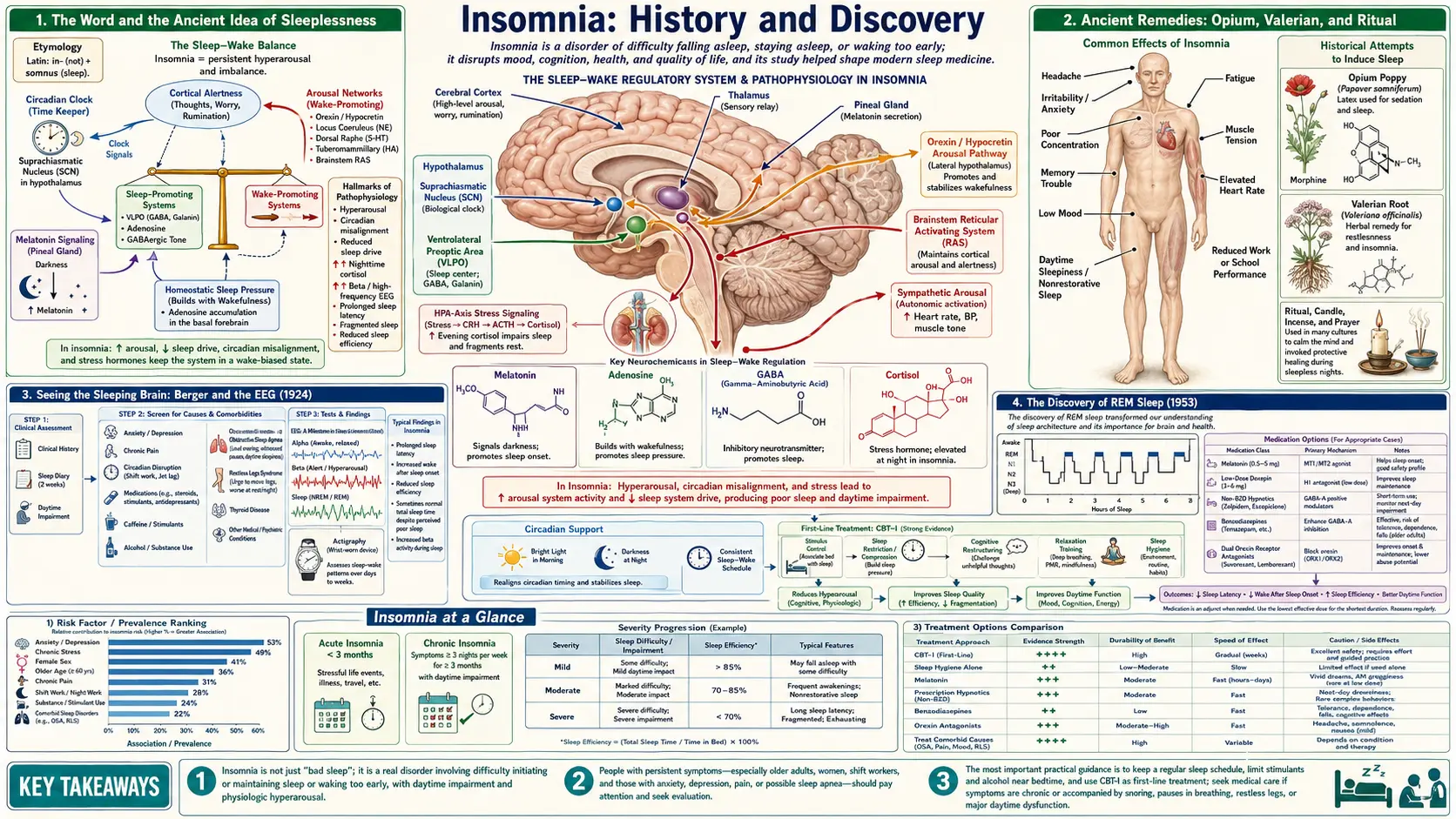
The word insomnia comes straight from Latin — in- (“not”) plus somnus (“sleep”), the same root that gives us Somnus, the Roman god of sleep, and his Greek counterpart Hypnos, from whom we get hypnotic. Sleeplessness is as old as humanity, and for most of recorded history people fought it with opium, valerian, ritual, and prayer, with no idea what sleep actually was. The scientific study of sleep is overwhelmingly a story of the last hundred years: Hans Berger’s recording of human brain waves in 1924 made it possible to see sleep, Eugene Aserinsky and Nathaniel Kleitman discovered REM (rapid-eye-movement) sleep in 1953, and a new medical specialty grew up around the sleep laboratory. The drugs evolved from dangerous barbiturates toward gentler agents, but the single most effective long-term treatment turned out not to be a drug at all — it is Cognitive Behavioral Therapy for Insomnia (CBT-I).
Table of Contents
- The Word and the Ancient Idea of Sleeplessness
- Ancient Remedies: Opium, Valerian, and Ritual
- Seeing the Sleeping Brain: Berger and the EEG (1924)
- The Discovery of REM Sleep (1953)
- The Birth of Sleep Medicine: Dement, the Clinic, and Polysomnography
- Why We Sleep When We Do: The Two-Process Model (1982)
- From Barbiturates to Orexin Blockers: A History of Sleeping Pills
- The Quiet Revolution: Cognitive Behavioral Therapy for Insomnia
- Insomnia Today: What the History Teaches
- Research Papers and References
- Connections
- Featured Videos
The Word and the Ancient Idea of Sleeplessness
The English word insomnia entered the language directly from Latin insomnia, meaning “sleeplessness” or “want of sleep,” built from the adjective insomnis (“sleepless”) — in-, “not,” joined to somnus, “sleep.” The same somnus survives in somnolent (drowsy) and somnambulist (sleepwalker). The Latin somnus is cognate with the Greek hypnos, which is why the modern medical word for a sleep-inducing drug is a hypnotic. In Roman myth Somnus was the personified god of sleep, the brother of Death and father of dreams — a reminder that long before sleep could be measured, it was felt to sit on the boundary between the living world and something else.
Sleeplessness itself needs no etymology to be understood: it is one of the most universally described human afflictions, recorded in the literatures of Mesopotamia, Egypt, Greece, India, and China. Physicians of antiquity treated wakefulness as a symptom — of fever, grief, mania, pain, or an imbalance of the bodily “humours” — rather than as a disease in its own right. That older framing, in which insomnia is so often the visible edge of anxiety, depression, pain, or another disorder, has proven remarkably durable; modern sleep medicine still distinguishes primary insomnia from the far more common insomnia that travels alongside another condition.
What the ancients lacked was any notion of what sleep was. To Aristotle and the Hippocratic writers, sleep was a passive cooling or settling of the body, a withdrawal of the senses — an idea that, with variations, held sway for more than two thousand years. The radical discovery of the twentieth century was that sleep is not an absence of brain activity at all, but a highly organized, active process with its own architecture. That single shift — from sleep-as-nothing to sleep-as-something — is what made a science of insomnia possible.
Ancient Remedies: Opium, Valerian, and Ritual
For most of history the treatment of insomnia meant reaching for whatever plant, drink, or rite seemed to bring sleep. The most powerful of the ancient sleep agents was the opium poppy (Papaver somniferum — the species name itself means “sleep-bringing”), whose milky latex was used for sedation and pain relief in ancient Egypt, Sumer, Greece, and Rome. Wine mixed with plant alkaloids was a common Greco-Roman soporific, and the so-called “soporific sponges” of the later medieval period combined opium with henbane, mandrake, and other sedating — and frequently toxic and hallucinogenic — nightshades.
The gentlest and most enduring of the herbal remedies was valerian (Valeriana officinalis). It carries an unusually well-documented pedigree: the Greek physicians Hippocrates (c. 460–370 BCE) and Dioscorides (first century CE) recorded its use, and the Roman physician Galen (c. 130–200 CE), who attended the emperor Marcus Aurelius, is traditionally said to have prescribed valerian for sleeplessness. Across the same centuries, traditional Chinese medicine relied on calming botanicals such as the seed of the sour jujube (suan zao ren), and many cultures wove sleep into ritual — prayers, sleep temples, lullabies, and bedtime customs — recognizing, in effect, the behavioral side of sleep long before anyone could explain it.
These remedies should be read as history, not as recommendations. Opium and the nightshade soporifics were genuinely dangerous, capable of killing as easily as soothing, and the line between an effective dose and a fatal one was perilously thin. What the ancient record does show is a continuity that runs straight to the present: people have always wanted both a substance to bring sleep and a practice to invite it — the two impulses that, in modern form, became the sleeping pill and CBT-I. Valerian, notably, is still studied and used today, the rare ancient sleep remedy that has survived into the era of controlled trials.
Seeing the Sleeping Brain: Berger and the EEG (1924)
The scientific study of sleep became possible only when it became possible to record the living human brain. That breakthrough belongs to the German psychiatrist Hans Berger (1873–1941), who on 6 July 1924, at the University Hospital in Jena, succeeded in recording electrical activity from the surface of a human scalp — the first human electroencephalogram, a term Berger himself coined. Filled with doubt about so improbable a result, he withheld publication for five years, finally releasing his landmark paper, Über das Elektrenkephalogramm des Menschen (“On the Electroencephalogram of Man”), in 1929. In it he described the rhythmic oscillations he named alpha waves (still sometimes called “Berger waves”) and the faster beta waves.
Berger’s findings were initially met with skepticism and even derision from the German scientific establishment; the work was vindicated only in 1934, when the eminent British physiologists Edgar Adrian and Bryan Matthews confirmed and championed it. Once accepted, the EEG transformed neuroscience. For sleep research, its importance is hard to overstate: for the first time, the brain’s state could be watched continuously through the night, and the long-held assumption that sleep was simply the brain “switched off” could finally be tested.
What the EEG revealed was that sleep is not a single flat state but a structured sequence of distinct electrical patterns that cycle through the night. Through the 1930s, researchers such as Alfred Loomis and colleagues used the EEG to sketch the first sleep stages, charting how the brain’s waves slow and deepen as a sleeper descends from drowsiness into deep sleep. The stage was set — literally and electrically — for the discovery that would split sleep in two.
The Discovery of REM Sleep (1953)
The pivotal moment in the history of sleep science came in 1953 in a physiology laboratory at the University of Chicago. Nathaniel Kleitman (1895–1999) — often called the father of modern sleep research, and author of the field-defining 1939 book Sleep and Wakefulness — had built the first laboratory in the world devoted to the systematic study of sleep. His graduate student Eugene Aserinsky, monitoring sleeping subjects (including, famously, his own young son) with instruments recording eye movements and brain waves, noticed something nobody had reported: recurring periods during the night when the eyes darted rapidly back and forth beneath closed lids, accompanied by a fast, low-voltage, waking-like EEG and irregular breathing and heart rate.
Aserinsky and Kleitman published the discovery of this rapid-eye-movement (REM) sleep in the journal Science in 1953, in a paper titled “Regularly occurring periods of eye motility, and concomitant phenomena, during sleep.” Crucially, when subjects were woken during these REM episodes they usually reported vivid dreams — tying a specific, measurable brain state to the experience of dreaming for the first time in history. Sleep, it turned out, was not one thing but two fundamentally different states: quiet (non-REM) sleep and the paradoxically active REM sleep, alternating in roughly 90-minute cycles across the night.
The discovery launched the modern science of sleep. A young physician named William C. Dement (1928–2020) joined Kleitman’s laboratory, and in 1957 he and Kleitman published the first systematic description of the human sleep cycle and its succession of stages. It was Dement who coined the now-universal term REM sleep. (In France, working independently, Michel Jouvet was tracing the brainstem machinery of REM in cats at the same time.) From a graduate student watching eyes flicker in the dark grew an entire scientific field.
The Birth of Sleep Medicine: Dement, the Clinic, and Polysomnography
Discovering the structure of sleep was one thing; turning that knowledge into the care of patients was another, and that step is largely the achievement of William Dement, frequently called the father of sleep medicine. After spending the rest of his career at Stanford University, Dement in 1970 opened the Stanford Sleep Disorders Clinic, widely regarded as the world’s first clinic devoted to diagnosing and treating sleep disorders. For the first time, a patient with chronic insomnia, crushing daytime sleepiness, or strange nighttime behavior had a medical home built specifically around the science of sleep.
Central to the new specialty was the all-night sleep study. Dement coined the term polysomnography (literally “many sleep writings”) — the simultaneous recording of brain waves (EEG), eye movements, muscle tone, breathing, and heart rhythm through the night — partly, as he later recounted, to give the procedure a formal name that insurers would recognize and reimburse. Polysomnography remains the gold-standard diagnostic tool of sleep medicine, the instrument that distinguishes insomnia from sleep apnea, restless legs, narcolepsy, and the parasomnias.
From these foundations sleep medicine grew into a recognized clinical discipline, with its own professional societies, board certification, and accredited sleep laboratories. The crucial lesson for insomnia was diagnostic humility: many people who complain of “not sleeping” in fact have an underlying, treatable disorder — obstructive sleep apnea above all — and the sleep laboratory exists precisely to find it. Insomnia, the field came to insist, is a symptom to be explained, not merely a complaint to be sedated.
Why We Sleep When We Do: The Two-Process Model (1982)
If the EEG showed what sleep looks like and REM showed that sleep has parts, a further question remained: what governs when we feel sleepy and when we wake? The most influential answer is the two-process model of sleep regulation, proposed by the Swiss sleep scientist Alexander Borbély in 1982 in the paper “A two process model of sleep regulation” (Human Neurobiology). The model is now a cornerstone framework taught in every sleep course, and it is essential to understanding insomnia and its treatment.
The model proposes that sleep is driven by the interaction of two independent processes. Process S is the homeostatic sleep drive — a kind of “sleep pressure” that builds steadily the longer one stays awake and dissipates during sleep; the longer you are awake, the harder this process pushes you toward sleep. Process C is the circadian process — the roughly 24-hour internal clock that sets alternating windows of alertness and sleepiness regardless of how long you have been awake. Sleep comes most easily when high sleep pressure (S) coincides with the down-swing of the circadian alerting signal (C); insomnia often arises when the two fall out of alignment.
The two-process model is more than theory — it is the engine behind the most effective behavioral treatments for insomnia. Sleep restriction therapy, a core component of CBT-I, works by deliberately raising homeostatic sleep pressure (Process S) so that sleep becomes deeper and more consolidated. Advice to keep a fixed wake time, get morning light, and avoid long naps is, in effect, advice to strengthen and align Process C. The framework that began as a mathematical sketch of sleep regulation became, in practice, a manual for repairing broken sleep without drugs.
From Barbiturates to Orexin Blockers: A History of Sleeping Pills
The pharmacological treatment of insomnia is a cautionary tale of repeating hope and disappointment. The first true synthetic hypnotic of the modern era was barbital (Veronal), whose sedative properties were discovered by Emil Fischer and Joseph von Mering in 1903; phenobarbital followed in 1911. Barbiturates dominated as “sleeping pills” for the first half of the twentieth century — but they carried a narrow margin of safety, high potential for dependence, and a lethal risk in overdose. Barbiturate overdose, accidental and deliberate, became a defining hazard of the mid-century medicine cabinet.
The search for something safer produced the benzodiazepines. The first, chlordiazepoxide (Librium), reached the market in 1960, soon followed by diazepam (Valium) and dedicated hypnotics such as temazepam and flurazepam. Acting on the brain’s GABA-A receptors, they were far safer in overdose than barbiturates and quickly became among the most-prescribed drugs in the world. Yet by the 1970s and 1980s their own liabilities were clear: tolerance, next-day grogginess, rebound insomnia, and physical dependence with a difficult withdrawal.
Next came the “Z-drugs” — zolpidem (Ambien), zaleplon, and eszopiclone — with zolpidem introduced in Europe in 1988 and in the United States in 1993. Though chemically distinct from benzodiazepines, they act on the same GABA-A system and were marketed as more selective and shorter-acting. They too, it emerged, can cause dependence, rebound insomnia, and unsettling complex sleep behaviors such as sleep-walking, sleep-eating, and sleep-driving — risks serious enough to draw prominent regulatory warnings. The newest class works on an entirely different target: the dual orexin receptor antagonists, beginning with suvorexant (Belsomra), approved by the U.S. Food and Drug Administration on 13 August 2014. Rather than broadly sedating the brain, these drugs block orexin (hypocretin), the wake-promoting signal — in effect dialing down wakefulness instead of forcing sleep.
The honest through-line of this two-century history is that no sleeping pill has proven to be the hoped-for clean solution; each generation traded one set of problems for another, and dependence and next-day impairment have shadowed nearly all of them. That sobering record is exactly why the field’s center of gravity has shifted away from drugs and toward a non-pharmacological treatment — and why current guidelines reserve hypnotics largely for short-term or adjunctive use.
The Quiet Revolution: Cognitive Behavioral Therapy for Insomnia
The most important development in the modern treatment of chronic insomnia is not a molecule but a method: Cognitive Behavioral Therapy for Insomnia (CBT-I). Its roots reach back to the behavioral sleep medicine of the 1970s. In 1972 the American psychologist Richard Bootzin introduced stimulus-control therapy, built on a simple but powerful insight: in chronic insomnia the bed itself becomes a learned cue for wakefulness and frustration rather than for sleep, and that association can be deliberately re-trained (get out of bed when you cannot sleep; reserve the bed for sleep alone; keep a fixed rising time). Later in the decade the psychologist Peter Hauri popularized the concept of sleep hygiene as it is understood today.
These behavioral techniques were gradually combined — stimulus control, sleep-restriction therapy (consolidating sleep by limiting time in bed, drawing directly on the homeostatic Process S), cognitive restructuring (challenging the anxious, catastrophic beliefs about sleep that keep people awake), relaxation training, and sleep-hygiene education — into the structured, multi-component package now called CBT-I, typically delivered over six to eight sessions. Rather than sedating the brain, CBT-I rebuilds the natural drive to sleep and dismantles the worry that perpetuates insomnia.
A large body of clinical-trial evidence has established that CBT-I is effective, that its benefits are durable long after the sessions end (unlike sleeping pills, which typically stop working once stopped), and that it lacks the dependence and next-day impairment of hypnotics. On that basis, major bodies including the American College of Physicians now recommend CBT-I as the first-line treatment for chronic insomnia in adults — positioning medication as a secondary or short-term option rather than the default. In a real sense this closes the historical circle: the ancient impulse toward a sleep practice, refined by a century of sleep science, has become the most powerful insomnia treatment we have. The chief obstacle now is access, which digital and self-guided CBT-I programs are working to widen.
Insomnia Today: What the History Teaches
The arc from somnus to CBT-I carries several lessons that still shape good care. The first is that sleep is active, structured, and measurable — the discovery that overturned two millennia of treating sleep as mere absence, and the foundation of everything that followed. Berger’s EEG and the Aserinsky–Kleitman discovery of REM did not just satisfy curiosity; they made it possible to ask, for any sleepless patient, what is actually happening in the brain at night.
The second lesson is diagnostic: insomnia is frequently the visible edge of something else — anxiety, depression, chronic pain, or, very commonly, obstructive sleep apnea — which is exactly why sleep medicine built the sleep laboratory and why a careful evaluation matters more than a quick prescription. The third lesson is therapeutic and hard-won: across more than a century, sleeping pills have repeatedly promised more than they delivered, while a drug-free, learning-based treatment quietly proved itself the most durable answer. The two-process model explains why CBT-I works, grounding a behavioral therapy in the underlying biology of sleep regulation.
None of this is medical advice, and the older remedies in particular — opium, the nightshade soporifics, even the casual long-term use of strong hypnotics — carry real dangers that this history is meant to illuminate rather than endorse. Anyone with persistent insomnia, especially when paired with loud snoring, daytime exhaustion, low mood, or thoughts of self-harm, deserves a proper evaluation. The encouraging truth at the end of this long story is that chronic insomnia is now one of the more treatable conditions in medicine — and that the most effective treatment is also among the safest.
Research Papers and References
The list below combines key peer-reviewed and historical sources on the science and history of sleep with curated PubMed topic-search links. Where a stable identifier is available it is given; otherwise the link opens a PubMed (National Library of Medicine) topic search in a new tab. Ancient and historical primary texts (Hippocrates, Dioscorides, Aristotle, Berger’s 1929 paper) are named in the article as historical sources.
- Aserinsky E, Kleitman N. Regularly occurring periods of eye motility, and concomitant phenomena, during sleep. Science. 1953;118(3062):273–274. — doi:10.1126/science.118.3062.273
- Dement W, Kleitman N. Cyclic variations in EEG during sleep and their relation to eye movements, body motility, and dreaming. Electroencephalography and Clinical Neurophysiology. 1957;9(4):673–690. — doi:10.1016/0013-4694(57)90088-3
- Borbély AA. A two process model of sleep regulation. Human Neurobiology. 1982;1(3):195–204. — PubMed: 7185792
- Borbély AA, Daan S, Wirz-Justice A, Deboer T. The two-process model of sleep regulation: a reappraisal. Journal of Sleep Research. 2016;25(2):131–143. — doi:10.1111/jsr.12371
- Bootzin RR, Epstein DR. Understanding and treating insomnia. Annual Review of Clinical Psychology. 2011;7:435–458. — doi:10.1146/annurev.clinpsy.3.022806.091516
- Qaseem A, Kansagara D, Forciea MA, et al. Management of chronic insomnia disorder in adults: a clinical practice guideline from the American College of Physicians. Annals of Internal Medicine. 2016;165(2):125–133. — doi:10.7326/M15-2175
- Trauer JM, Qian MY, Doyle JS, Rajaratnam SMW, Cunnington D. Cognitive behavioral therapy for chronic insomnia: a systematic review and meta-analysis. Annals of Internal Medicine. 2015;163(3):191–204. — doi:10.7326/M14-2841
- Hans Berger and the centennial of the human electroencephalogram (1924–2024) — PubMed: Hans Berger EEG history
- History and discovery of REM sleep (Aserinsky, Kleitman, Dement) — PubMed: history of REM sleep
- History of hypnotic and sedative drugs: barbiturates, benzodiazepines, Z-drugs — PubMed: history of hypnotic drugs
- Suvorexant and dual orexin receptor antagonists for insomnia — PubMed: orexin antagonists for insomnia
- Valerian (Valeriana officinalis) for insomnia — history and evidence — PubMed: valerian for insomnia
- Cognitive behavioral therapy for insomnia (CBT-I) — efficacy and components — PubMed: CBT-I efficacy
- Stimulus-control and sleep-restriction therapy for insomnia — PubMed: behavioral therapy for insomnia
External Authoritative Resources
- National Heart, Lung, and Blood Institute (NIH) — Insomnia
- National Institute of Neurological Disorders and Stroke — Sleep Disorders
- PubMed — Insomnia and the history of sleep science
Connections
- Psychiatry
- Insomnia (main article)
- All Conditions
- Anxiety
- Depression
- Obstructive Sleep Apnea
- PTSD
- Bipolar Disorder