Grief: History and Discovery
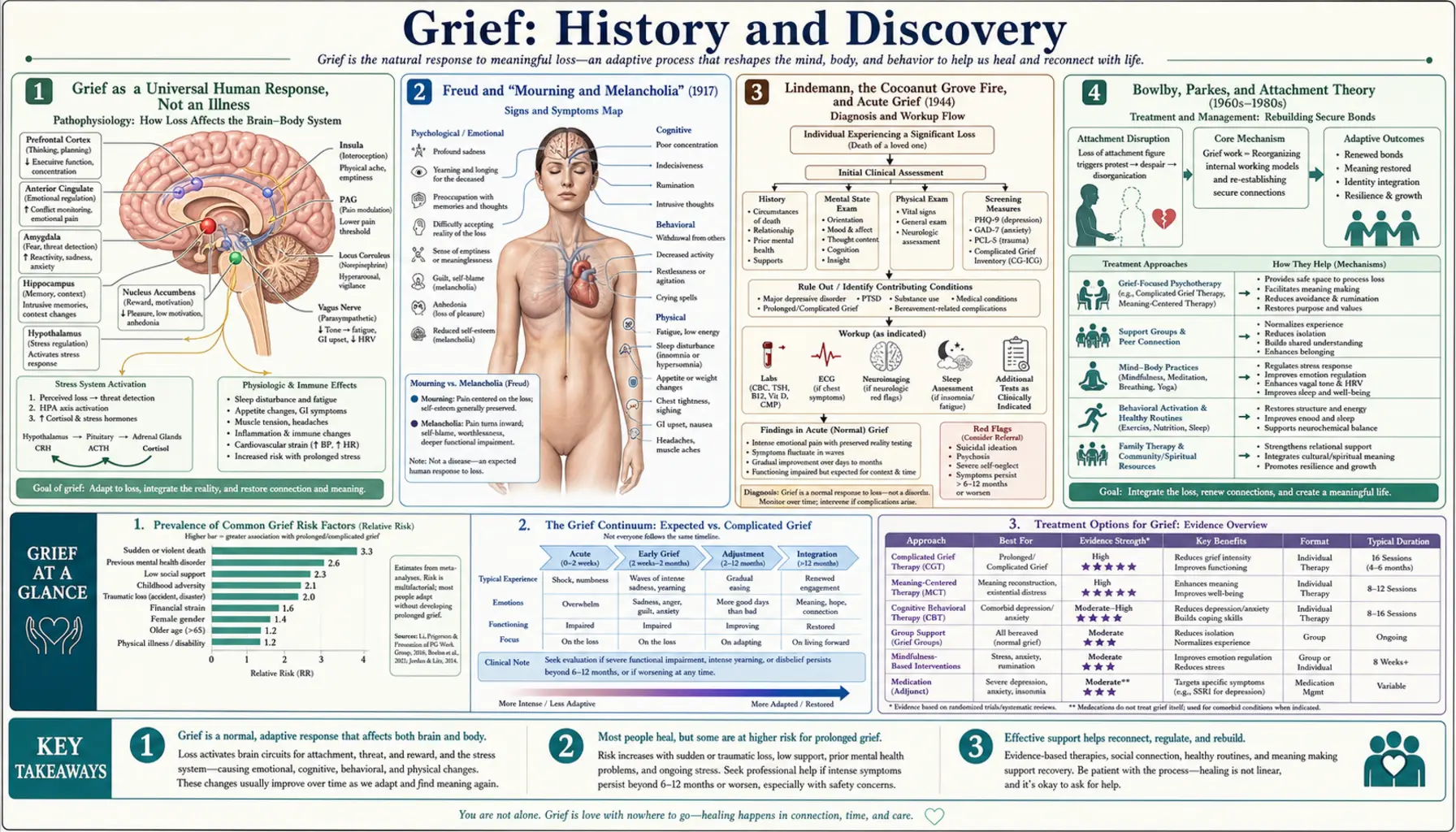
Grief is one of the oldest and most universal of all human experiences — the natural response to the loss of someone or something we love. It is not, in itself, an illness; mourning the dead is recorded in the earliest human writing, ritual, and art, and to grieve is simply to have loved. What does have a history is the scientific and psychological study of grief: the comparatively recent effort to describe, explain, and occasionally treat what happens to the mind and body after a loss. This article traces that intellectual history — from Sigmund Freud's 1917 essay distinguishing normal mourning from depression, through Erich Lindemann's wartime study of survivors, John Bowlby's attachment theory, and the famous (and famously misunderstood) "five stages," to the modern dual process model and the recent recognition of prolonged grief disorder as a distinct condition. A note of care throughout: most grief is healthy and needs companionship, not a diagnosis. Only a minority becomes the persistent, disabling condition that clinicians now recognize as a disorder.
Table of Contents
- Grief as a Universal Human Response, Not an Illness
- Freud and "Mourning and Melancholia" (1917)
- Lindemann, the Cocoanut Grove Fire, and Acute Grief (1944)
- Bowlby, Parkes, and Attachment Theory (1960s–1980s)
- Kübler-Ross and the Misunderstood "Five Stages" (1969)
- The Dual Process Model and Continuing Bonds (1990s)
- Prolonged Grief Disorder Enters ICD-11 and DSM-5-TR (2018–2022)
- What the History Teaches: Holding Science and Compassion Together
- Research Papers and References
- Connections
- Featured Videos
Grief as a Universal Human Response, Not an Illness
Before there was any science of grief, there was grief itself. The burial of the dead with care, ornament, and offering is among the most ancient signs of human culture; lamentation, mourning rites, and elegy appear in the earliest texts of Mesopotamia, Egypt, Greece, and the Hebrew Bible. Every known human society has rituals of mourning — wakes, vigils, funerals, periods of withdrawal, the wearing of particular clothes or colours — because the loss of a loved one is one of the few experiences that come to nearly everyone who lives long enough. To grieve, in this sense, is not a malfunction. It is the price and the proof of attachment.
This matters because the history that follows is a history of study, and study can quietly medicalize something that is, for the overwhelming majority of people, a normal and self-limiting process. Modern bereavement research is consistent on this point: most bereaved people, given time, support, and the ordinary rhythms of life, move through acute grief without any professional treatment and without developing a mental disorder. The pain can be severe — waves of sorrow, longing, disrupted sleep, loss of appetite, difficulty concentrating, even brief experiences of hearing or sensing the dead person — and still be an entirely healthy response that needs companionship, patience, and time rather than diagnosis or medication.
The thinkers in this article were all, in their better moments, trying to draw a careful line: to describe grief honestly, to recognize the small minority for whom it becomes genuinely disabling, and to offer help — without pathologizing love itself. Where they drew that line well, and where later popular culture blurred it, is much of the story. Throughout, it is worth holding the simplest truth first: grief is a normal human response to loss, and the great majority of it heals on its own.
Freud and "Mourning and Melancholia" (1917)
The modern psychological study of grief is usually traced to a single short essay. In 1917, Sigmund Freud published Trauer und Melancholie — "Mourning and Melancholia" — written during the First World War, a time of mass bereavement. Its central contribution was a distinction that still organizes the field: the difference between normal mourning (Trauer) and melancholia (a term that maps roughly onto what we now call clinical depression). Freud argued that both follow loss and share many features — profound dejection, loss of interest in the outside world, withdrawal from activity — yet they are not the same thing.
The key difference Freud identified was self-regard. In ordinary mourning, he wrote, the world becomes poor and empty; in melancholia, it is the self that becomes poor and empty, marked by relentless self-reproach, worthlessness, and a fall in self-esteem that mourning does not produce. In his account, the mourner consciously knows what has been lost and, over time, gradually withdraws emotional attachment from the lost person and reinvests it in life; the melancholic, by contrast, suffers a loss that is more unconscious and unresolved, turning the anger and disappointment of the severed bond inward against the self. Whatever one makes of the underlying psychoanalytic theory, the clinical observation was durable.
The importance of the essay for our purposes is not its now-dated mechanism but its founding move: it treated mourning as a normal, time-limited process distinct from pathological depression, and it insisted that the two could be told apart. That distinction — normal grief versus a depressive illness — is the seed from which a century of bereavement science grew, and it remains the first question any clinician asks of a grieving person today.
Lindemann, the Cocoanut Grove Fire, and Acute Grief (1944)
If Freud supplied the founding distinction, the first systematic clinical study of grief came out of catastrophe. On the night of 28 November 1942, the Cocoanut Grove nightclub in Boston caught fire; the blaze killed 492 people and injured hundreds more, the deadliest nightclub fire in United States history. Many of the injured and the suddenly bereaved were treated at Massachusetts General Hospital, where the psychiatrist Erich Lindemann studied the survivors and the grieving families in the weeks and months that followed.
From this work — combined with other bereaved patients he saw — Lindemann published "Symptomatology and Management of Acute Grief" in the American Journal of Psychiatry in 1944. He described acute grief as a recognizable syndrome with a characteristic, observable pattern: bodily distress coming in waves (tightness in the throat, shortness of breath, sighing, an empty feeling in the abdomen, exhaustion), intense preoccupation with the image of the deceased, guilt, irritability and anger, and a disruption of ordinary patterns of conduct. Crucially, he held that this acute syndrome was generally normal and self-limiting, but that it could become distorted, delayed, or chronic.
Lindemann coined the influential phrase "grief work" for the active psychological process he believed mourning required: loosening the bonds to the person who had died, readjusting to a world without them, and forming new relationships. The idea that grief is something a person must do — not merely suffer passively — shaped decades of theory and practice, and it helped launch the crisis-intervention and preventive-psychiatry movements Lindemann went on to lead. (Later research would qualify the "grief work hypothesis," finding that not everyone needs to actively "work through" grief in this way; but as the first rigorous clinical description of acute bereavement, the 1944 paper is foundational.)
Bowlby, Parkes, and Attachment Theory (1960s–1980s)
The next major framework reframed grief in terms of attachment. The British psychiatrist John Bowlby, developing his attachment theory from the late 1950s onward, proposed that human beings are biologically predisposed to form strong affectional bonds — first between infant and caregiver, and later between adults — and that grief is the natural, evolved response to the rupture of such a bond. In this view the searching, yearning, anxiety, and anger of the bereaved are not signs of weakness or illness but the misfiring of attachment behaviours that evolved to recover a lost figure who, in death, cannot be recovered.
Bowlby set out these ideas in his landmark trilogy Attachment and Loss — Attachment (1969), Separation: Anxiety and Anger (1972), and Loss: Sadness and Depression (1980) — building on an earlier paper, "Grief and Mourning in Infancy and Early Childhood" (1960). Working closely with him, the psychiatrist Colin Murray Parkes brought this framework to the study of adult bereavement and, drawing on his own research with widows, helped describe grief as unfolding through overlapping phases — numbness, yearning and searching, disorganization and despair, and reorganization. It is important to read these as loose, overlapping descriptions of common experiences, not a fixed staircase every mourner must climb.
The attachment account remains one of the most influential and empirically productive ways of understanding grief, because it ties the intensity of mourning to the strength and security of the bond that was broken, and it explains why loss can reactivate the same separation distress seen when a small child is parted from a parent. It grounds grief in normal human biology and love — an antidote to viewing it primarily as pathology.
Kübler-Ross and the Misunderstood "Five Stages" (1969)
No idea about grief is more famous — or more widely misapplied — than the "five stages." In her 1969 book On Death and Dying, the Swiss-American psychiatrist Elisabeth Kübler-Ross described five stages she observed in terminally ill patients coming to terms with their own approaching death: denial, anger, bargaining, depression, and acceptance (often abbreviated DABDA). The book grew out of seminars and interviews she conducted with roughly five hundred dying patients, at a time when medicine largely avoided honest conversation about death. As a humane call to listen to the dying, it was rightly celebrated and hugely influential.
Here the historical record needs to be clear, because this point is constantly gotten wrong. Kübler-Ross's five stages were originally observations of people facing their own dying, not a model of bereavement — not a description of how the surviving loved ones grieve a death. Only later, in popular culture and self-help writing, were the stages transplanted onto grief in general and hardened into a supposed sequence that mourners must pass through, in order, to "heal." That popular "stages of grief" framework is not a validated, universal, or sequential model, and treating it as one is a misreading.
The evidence does not support the idea that grieving people reliably move through fixed, ordered stages, and researchers and clinicians have repeatedly cautioned against using the stages as a checklist or a yardstick of "normal" grief. Real grief is far more variable, individual, and non-linear — it comes in waves, loops back, and looks different for different people and cultures. Kübler-Ross herself, with co-author David Kessler, later stressed that the stages "were never meant to help tuck messy emotions into neat packages" and were not meant as a rigid sequence. The honest summary: the five stages are a useful, humane vocabulary for some of the feelings loss can bring, but they are not a strongly evidence-based, step-by-step map of grief, and no one should feel they are grieving "wrong" for not following them.
The Dual Process Model and Continuing Bonds (1990s)
By the 1990s, researchers were moving decisively away from stage and phase models toward accounts that better matched what bereaved people actually do. The most influential of these is the Dual Process Model of Coping with Bereavement, proposed by Margaret Stroebe and Henk Schut in 1999. Rather than a sequence to complete, the model describes an ongoing oscillation between two kinds of coping: loss-oriented coping (confronting the loss itself — the sorrow, yearning, memories, and emotional work of mourning) and restoration-oriented coping (dealing with the practical, secondary changes loss brings — new roles, tasks, finances, identity, and rebuilding daily life).
The model's key insight is that healthy grieving involves moving back and forth between confronting the loss and taking breaks from it to attend to living — and that both the grieving and the distraction are necessary and adaptive. This reframes "avoidance" not as denial to be overcome but, in measured doses, as a normal and even protective part of coping. The dual process model is hypothesis-driven and continues to be researched and refined rather than treated as settled fact, but it has reshaped bereavement theory because it fits the lived, oscillating, day-to-day reality of grief far better than any staircase.
A second important 1990s shift was the continuing bonds perspective (Klass, Silverman, and Nickman, 1996), which challenged the older assumption — traceable to Freud and Lindemann's "grief work" — that mourning means severing ties to the dead. Researchers observed that many bereaved people maintain an ongoing, comforting inner relationship with the person who died — through memory, ritual, conversation, and a felt sense of presence — and that this can be entirely healthy rather than a failure to "let go." Together, the dual process and continuing-bonds models define the modern, more flexible, and more compassionate understanding of normal grief.
Prolonged Grief Disorder Enters ICD-11 and DSM-5-TR (2018–2022)
For most of the twentieth century there was no formal psychiatric diagnosis specifically for grief, precisely because grief is normal. Yet clinicians and researchers repeatedly noticed a minority of bereaved people — commonly estimated in research at roughly one in ten — for whom acute grief does not ease with time but instead remains intense, persistent, and severely disabling for many months or years, dominating their lives and impairing their ability to function. Over the 1990s and 2000s this was studied under several names, including complicated grief, traumatic grief, and persistent complex bereavement disorder, before the field converged on a single condition.
That condition is now recognized in both of the world's major diagnostic systems as prolonged grief disorder (PGD). The World Health Organization included prolonged grief disorder in the eleventh revision of the International Classification of Diseases (ICD-11), endorsed in 2019 and in effect from 2022; the American Psychiatric Association added prolonged grief disorder to the DSM-5-TR (the text revision of the DSM-5) in March 2022, classifying it among the trauma- and stressor-related disorders. The two systems define it similarly but not identically — notably in timing: the DSM-5-TR requires that the death have occurred at least 12 months earlier (in adults) before the diagnosis can be made, while the ICD-11 sets the threshold at an atypically prolonged response persisting beyond about 6 months. Both require that the grief be persistent, pervasive, and clearly beyond the expected social or cultural norm, causing significant impairment.
The single most important thing to understand about this diagnosis is what it is not. Prolonged grief disorder is not ordinary grief, and recognizing it is not an attempt to pathologize normal mourning or put a deadline on sorrow. The whole point of the time thresholds and the strict impairment criteria is to distinguish the small group who are genuinely stuck and suffering — and who may benefit from specific, evidence-based therapies — from the great majority whose grief, however painful, is healthy and will ease in its own time. The recognition of PGD was controversial for exactly this reason, and the debate it provoked is a healthy one: it keeps the field honest about the line between a normal human response and a treatable disorder. If your grief is intense but slowly softening, that is almost certainly normal grief, not a disorder; the diagnosis exists for persistent, disabling grief that is not getting better, and reaching out for help in that case is a sign of strength.
What the History Teaches: Holding Science and Compassion Together
Read as a whole, the history of grief research is a slow, sometimes faltering effort to do two things at once: to understand grief scientifically and to honour it humanely. Freud separated normal mourning from depression; Lindemann described the acute grief syndrome and named "grief work"; Bowlby and Parkes grounded grief in attachment and love; Kübler-Ross taught a generation to listen to the dying (even as her stages were later misapplied to the bereaved); Stroebe and Schut captured grief's real, oscillating rhythm; and the continuing-bonds researchers freed mourners from the demand to "let go." Finally, ICD-11 and DSM-5-TR carved out a careful diagnosis for the suffering minority — without claiming that grief as such is a disease.
The clearest lesson of that history is a warning against two opposite errors. The first is over-medicalizing grief — treating ordinary, healthy mourning as a disorder to be fixed, hurried, or medicated away, or judging people against a stage model the evidence never supported. The second is under-recognizing the genuine minority whose grief becomes a persistent, disabling condition that does respond to specific care. Good practice, like good history, holds both truths: grief is normal and usually needs companionship and time, and some grief becomes a disorder that deserves real help.
For anyone reading this while grieving: there is no correct timetable, no required sequence of stages, and no "right" way to mourn. Sorrow that comes in waves, that loops and returns, that coexists with ordinary moments of laughter or distraction, is the shape of normal grief. If, after many months, your grief remains as raw and consuming as the first weeks and is keeping you from living, that is worth talking to a clinician about — not because love is a pathology, but because, occasionally, grief needs more than time, and help is available. The century of study summarized here exists, in the end, to make ordinary mourning more understood and the rare disabling kind more treatable.
Research Papers and References
The list below combines the landmark historical papers in grief and bereavement research with curated PubMed topic-search links into the modern literature. Some of the foundational works (Freud's 1917 essay; Kübler-Ross's 1969 book On Death and Dying; Bowlby's Attachment and Loss trilogy of 1969–1980) are books and historical essays named in the article as primary sources rather than as DOI-linked journal articles. Where a stable DOI or PMID exists it is given; otherwise a PubMed topic search is provided. Each link opens in a new tab.
- Lindemann E. Symptomatology and management of acute grief. American Journal of Psychiatry. 1944;101(2):141-148. (Foundational study drawing on Cocoanut Grove fire survivors.) — doi:10.1176/ajp.101.2.141
- Lindemann E. Symptomatology and management of acute grief. 1944. American Journal of Psychiatry (Sesquicentennial Supplement reprint). 1994;151(6 Suppl):155-160. — doi:10.1176/ajp.151.6.155 (PMID: 8192191)
- Stroebe M, Schut H. The dual process model of coping with bereavement: rationale and description. Death Studies. 1999;23(3):197-224. — doi:10.1080/074811899201046
- Stroebe M, Schut H. The dual process model of coping with bereavement: a decade on. Omega (Westport). 2010;61(4):273-289. — doi:10.2190/OM.61.4.b
- Zisook S, Shear K. Grief and bereavement: what psychiatrists need to know. World Psychiatry. 2009;8(2):67-74. — doi:10.1002/j.2051-5545.2009.tb00217.x
- Maciejewski PK, Zhang B, Block SD, Prigerson HG. An empirical examination of the stage theory of grief. JAMA. 2007;297(7):716-723. (Tests, and largely qualifies, the "stages" idea.) — doi:10.1001/jama.297.7.716
- Prigerson HG, Horowitz MJ, Jacobs SC, et al. Prolonged grief disorder: psychometric validation of criteria proposed for DSM-V and ICD-11. PLoS Medicine. 2009;6(8):e1000121. — doi:10.1371/journal.pmed.1000121
- Eisma MC, et al. Prolonged grief disorder in ICD-11 and DSM-5-TR: challenges and controversies. — PubMed: PGD in ICD-11 and DSM-5-TR — challenges and controversies (PMID 36748103)
- Prolonged grief disorder in ICD-11 and DSM-5-TR: differences in prevalence and diagnostic criteria. Frontiers in Psychiatry. 2024. — PMC: differences in prevalence and diagnostic criteria
- Freud's "Mourning and Melancholia" (1917) — historical and modern commentary — PubMed: Freud, Mourning and Melancholia, grief and depression
- Bowlby attachment theory, loss, and grief — PubMed: Bowlby, attachment theory, grief and bereavement
- Continuing bonds in bereavement (Klass, Silverman & Nickman tradition) — PubMed: continuing bonds in bereavement and grief
- Complicated, traumatic, and prolonged grief — history of the concept — PubMed: complicated and prolonged grief disorder, history of the concept
- Normal versus pathological grief — distinguishing bereavement from depression — PubMed: normal grief versus depression in bereavement
External Authoritative Resources
- National Institute of Mental Health (NIMH) — Coping with Loss and Traumatic Events
- WHO ICD-11 — Prolonged Grief Disorder (6B42)
- American Psychiatric Association — Prolonged Grief Disorder (DSM-5-TR)
Connections
- Psychiatry
- Grief: Normal Mourning, Complicated Grief & Prolonged Grief Disorder
- Depression
- Depression: History and Discovery
- PTSD (Post-Traumatic Stress Disorder)
- PTSD: History and Discovery
- Loneliness
- Burnout
- All Conditions