Factitious Disorder (Munchausen Syndrome)
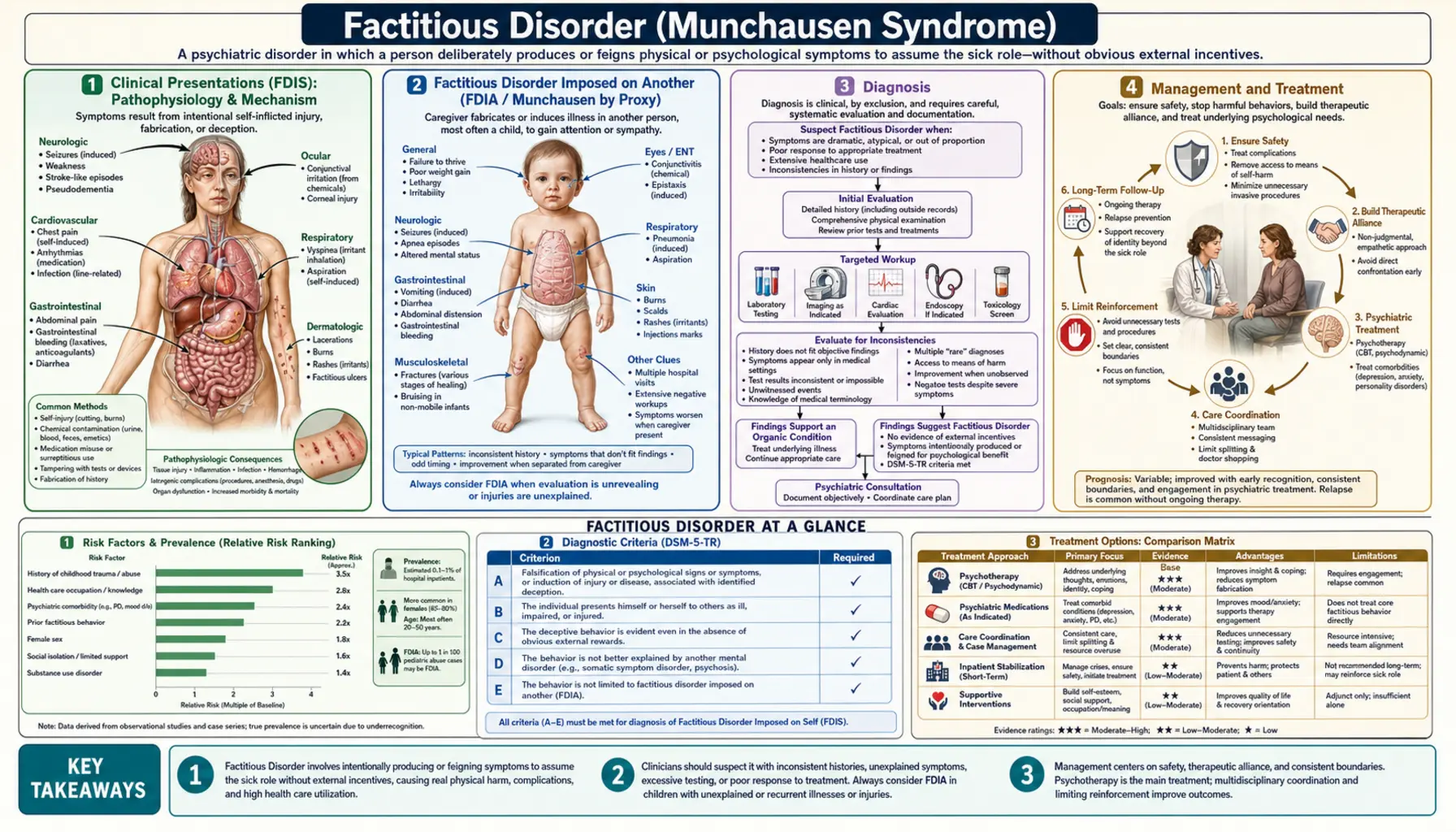
Factitious Disorder (historically called Munchausen Syndrome) involves the intentional feigning or production of physical or psychological signs and symptoms. The defining motive is to assume the "sick role" — not to obtain external gain (financial, legal, or otherwise), which distinguishes factitious disorder from malingering. DSM-5 recognizes two forms: Factitious Disorder Imposed on Self (FDIS) and Factitious Disorder Imposed on Another (FDIA) — formerly called Munchausen by Proxy — in which a caregiver induces illness in a child to assume the sick role by proxy, a pediatric abuse emergency. Prevalence is estimated at 0.02–0.6% of hospital patients, though the condition is massively underdiagnosed; estimates suggest 5–15% of unexplained symptoms in some specialty settings may have a factitious origin. A 3:1 female predominance is seen in classic FDIS. Healthcare workers are disproportionately represented among those affected. Commonly co-occurring personality disorders include borderline and antisocial personality disorder.
Clinical Presentations (FDIS)
Factitious Disorder Imposed on Self manifests across virtually every medical specialty, which is one reason it remains so difficult to detect. The presentations below represent the most commonly encountered and clinically dangerous patterns.
Fever: Patients may induce fever through self-injection of contaminated materials such as feces, saliva, or foreign substances. Others use technically simpler methods — microwaving a thermometer, holding it briefly to a heat source, or creating friction — to produce an artificially elevated reading. The absence of fever on objective electronic measurement (especially axillary or tympanic) while oral temperatures appear elevated is an important inconsistency to note.
Hypoglycemia: Exogenous insulin self-injection is one of the most medically dangerous factitious presentations. Patients may present with recurrent severe hypoglycemia requiring glucose infusion. The diagnostic key is the C-peptide assay: endogenous insulin production (as seen in insulinoma or other hyperinsulinism states) raises both insulin and C-peptide together, whereas exogenous insulin suppresses C-peptide while raising insulin levels. A low or undetectable C-peptide in the context of high insulin and hypoglycemia confirms exogenous insulin administration. Proinsulin levels are similarly suppressed by exogenous insulin and can add confirmatory value.
Anemia: Chronic self-phlebotomy can produce refractory iron-deficiency anemia with very low ferritin, requiring repeated transfusion. The pattern — transfusion dependency without evident bleeding, normal GI workup, no menorrhagia — can prompt extensive and unhelpful diagnostic workup if factitious origin is not considered.
Hematuria: Adding blood — typically from a self-inflicted wound or from menstrual blood — to urine samples produces a positive dipstick and can trigger extensive urological evaluation including cystoscopy. Observed urine collection, or catheterization for the specimen, resolves the discrepancy.
Rashes and wounds (dermatitis artefacta): Self-inflicted skin lesions often appear in unusual, geometric, or perfectly linear distributions that do not match the morphology of natural dermatological disease. Lesions may be created by caustics, hot objects, sharp instruments, or aggressive mechanical friction. The patient typically denies self-infliction, and all other causes must be rigorously excluded before considering the factitious diagnosis. Lesions tend to be exclusively on body areas the patient can reach with their dominant hand.
Neurological symptoms: Factitious seizures may be reported by the patient without witnesses, with a normal interictal EEG, no postictal period, and inconsistent or anatomically implausible lateralization. Some patients are diagnosed with epilepsy and treated with antiepileptic drugs for months or years before the pattern becomes apparent. Prolonged video-EEG monitoring capturing an episode without ictal correlate on EEG is the definitive distinguishing test.
Infections: Self-injection of feces, saliva, soil, or foreign material causing repeated bacteremia with unusual or mixed-flora organisms is the classic presentation that first brought Munchausen syndrome to medical attention. Repeated septic episodes in a patient without an obvious immune deficit or structural source, especially with organisms inconsistent with community-acquired infection, should raise clinical suspicion.
Factitious Disorder Imposed on Another (FDIA / Munchausen by Proxy)
Factitious Disorder Imposed on Another is among the most serious and covert forms of child abuse. The perpetrator — most commonly the biological mother, though fathers, foster parents, and other caregivers are also documented — induces illness in a dependent, typically a child under age 5, in order to assume the sick role by proxy. The perpetrator's psychological reward comes from occupying the role of devoted, worried caregiver of a medically complex child, attracting sympathy, attention, and medical engagement that they could not obtain independently.
The clinical pattern in the child is distinctive: repeated hospitalizations with unexplained or impossible-to-reproduce findings; symptoms that appear consistently when the caregiver is present and resolve or disappear entirely when the child is separated from the caregiver (especially during inpatient periods when the caregiver is absent); and test results or physical findings that are inconsistent with any natural disease course. Children may present with recurrent vomiting, diarrhea, apnea, seizures, infections, hypoglycemia, or bleeding — often with normal findings between caregiver-witnessed events.
Diagnosis is particularly challenging because the caregiver often presents as exceptionally devoted, medically knowledgeable, and emotionally distressed — a profile that initially inspires sympathy rather than suspicion. The caregiver may develop warm relationships with nursing and medical staff, making the eventual recognition of FDIA feel disorienting to the team.
In some institutions, covert video surveillance of the hospital room is used when FDIA is strongly suspected and child safety is at stake. This approach is legally and ethically complex — it typically requires authorization from the hospital ethics committee and legal counsel — but courts have upheld its use when child protection is the primary concern. Video evidence of a caregiver administering substances to the child, suffocating, or otherwise inducing symptoms is the most direct form of proof available.
FDIA is legally classified as child abuse in virtually all jurisdictions, triggering mandatory reporting obligations. Clinicians who identify credible suspicion of FDIA must report to child protective services regardless of their certainty level — mandatory reporting thresholds are based on reasonable suspicion, not proof. Child mortality from unrecognized FDIA is estimated at 6–10%. Even non-fatal FDIA causes lasting physical harm, developmental disruption, and significant psychological trauma in affected children, including iatrogenic injury from unnecessary procedures performed on clinical findings that were fabricated or induced.
Diagnosis
There is no single laboratory test or imaging finding that directly diagnoses factitious disorder — the diagnosis is built from the integration of clinical inconsistencies, strategic targeted testing, and the systematic exclusion of genuine pathology. It is fundamentally a diagnosis of both inclusion (evidence of intentional production) and exclusion (no better natural explanation).
Recognizing clinical inconsistencies: The most important diagnostic clue is internal inconsistency — symptoms that appear only when the patient believes they are being observed, laboratory values that are technically impossible in the context of claimed symptoms, wounds that follow unnatural geometric patterns, or conditions that resolve without any treatment during periods of closer observation. A pattern of unexplained medical conditions spread across multiple hospitals and specialties, revealed by retrospective record review, is highly suggestive.
Targeted workup: When factitious disorder is suspected, testing should be targeted to the specific presentation rather than broad and reflexive. For hypoglycemia, the C-peptide and proinsulin assay battery is essential. For suspected infection with unusual organisms, detailed speciation and sensitivity profiling of cultured organisms may reveal fecal flora or polymicrobial patterns inconsistent with endogenous infection. Expanded toxicology panels — including agents not routinely screened — can reveal administration of substances the patient has access to. For hematuria, direct observation during urine collection or catheterization for the specimen definitively resolves sample contamination.
Retrospective medical record review: Requesting records from prior institutions — often across multiple hospitals and specialties — frequently reveals a striking pattern of unexplained conditions, repeated negative workups, and a trail of unresolved diagnoses stretching back years. Patients with factitious disorder often move between institutions when suspicion mounts, a behavior sometimes called "hospital hopping." Some patients carry fabricated records or describe prior diagnoses that cannot be verified.
Confrontation strategy: Direct, unprepared confrontation — "you are faking this" — almost universally causes the patient to leave the hospital abruptly, cutting off any possibility of therapeutic engagement and placing them at ongoing risk. The preferred approach is multidisciplinary (treating physician, psychiatry, and social work acting together) with compassionate framing centered on the patient's welfare rather than accusation. A face-saving statement such as "sometimes people experience tremendous distress in ways they may not fully be aware of, and we want to help you with that underlying pain" provides psychological cover and creates space for ongoing care. The goal is to keep the patient engaged with treatment.
Management and Treatment
No randomized controlled trials exist for treatment of factitious disorder — the evidence base consists entirely of case series, case reports, and expert consensus. The field is further complicated by the fact that patients who are confronted and recognized frequently leave care, making long-term follow-up data sparse.
Compassionate confrontation is the cornerstone of management. The team approach — treating physician, psychiatry, and social work together — is more effective and less likely to precipitate abrupt departure than solo confrontation by a single clinician. The framing must be non-punitive, centered on the patient's suffering and need for care rather than on exposing deception. After confrontation, the immediate clinical priority is to avoid unnecessary further testing and procedures while remaining alert to the development of genuine illness — patients with factitious disorder also develop real conditions, and dismissing all symptoms as factitious is itself a clinical error.
Limiting reinforcing elements of the hospital environment is important: opioid analgesics and other reinforcing medications should be minimized; a single designated primary care coordinator should be identified to prevent "doctor shopping" across multiple providers and institutions; and care plans should be shared across the care team with the patient's knowledge to establish transparent expectations.
Psychotherapy is the primary treatment modality when patients engage. Comorbid borderline personality disorder — one of the most common co-occurring conditions — should be treated with dialectical behavior therapy (DBT), which has a strong evidence base for the emotion dysregulation and interpersonal dysfunction that drive much of the underlying behavior. Motivational interviewing may help patients begin to recognize and articulate the unmet needs that drive the sick-role behavior. Long-term individual therapy with a consistent, trusted therapist provides the stable attachment relationship that many of these patients have never had. Psychodynamic approaches addressing childhood trauma and unmet attachment needs have shown utility in case reports.
Hospitalization decisions require balancing the reinforcing nature of the hospital environment — which may perpetuate and reward the behavior — against genuine safety needs. For patients who have induced dangerous conditions (sepsis, severe hypoglycemia, significant blood loss), inpatient stabilization is non-negotiable. Outpatient management with a structured, consistent team is preferred once the acute situation is controlled.
Prognosis is guarded. Many patients continue the behavior across their lifetimes, accumulating significant medical harm from induced conditions and unnecessary procedures. A subset do engage with psychotherapy and achieve meaningful reduction in factitious behavior, particularly when underlying trauma, personality disorder, and attachment disruption are addressed directly.
Psychological Underpinnings
Factitious disorder is not primarily a condition of conscious deception for personal gain — it is a maladaptive coping mechanism driven by deep psychological need, most commonly the need for care, attention, identity, and structure that the person cannot access through healthy means. This distinction is clinically important because it shapes both how we understand the patient and how we engage therapeutically.
The sick role — the socially sanctioned status of being ill — provides benefits that are otherwise unavailable to the patient: permission to be cared for, exemption from ordinary responsibilities, a coherent and recognized identity, and the structured attention of medical professionals. For individuals whose early developmental experiences involved neglect, abuse, or emotional unavailability from caregivers, the medical setting may represent the only reliable context in which they have received consistent, attentive, non-judgmental care. Some patients report positive hospitalizations during childhood illness as formative experiences they seek to recreate.
Childhood trauma — physical abuse, emotional neglect, early illness — is a common antecedent. Many patients with factitious disorder have histories of genuine illness in childhood during which hospitalization brought positive parental engagement they did not otherwise receive, establishing the hospital as a psychologically safe environment associated with care. Unresolved grief, identity disturbance, and chronic emptiness — features also central to borderline personality disorder — frequently co-occur.
The degree to which the behavior is conscious versus driven by processes outside full awareness varies among patients and over time. Some patients are fully aware of their actions but cannot articulate why they cannot stop; others appear to have significant insight deficits about their motivations. The DSM-5 requirement that the deceptive behavior be "intentional" does not imply that the patient has complete conscious control over the compulsion driving it — the intentionality criterion is primarily meant to distinguish factitious disorder from somatic symptom disorder, where symptom production is not intentional.
The critical diagnostic and conceptual distinction from malingering deserves emphasis. In malingering, feigned illness serves an identifiable external reward: financial compensation, avoidance of legal or military obligations, obtaining controlled substances. Remove the external reward and the behavior stops. In factitious disorder, the reward is internal and psychological — the sick role itself — and persists in the absence of any external incentive. This is why factitious disorder is classified as a psychiatric condition while malingering is not.
Differential Diagnosis
Factitious disorder is a diagnosis of exclusion and must be distinguished from a range of conditions with overlapping features. The most critical distinction in all cases is between intentional symptom production (factitious disorder or malingering) and unintentional symptom experience (somatic symptom disorders and conversion disorder).
Somatic Symptom Disorder: Patients genuinely believe their symptoms are real and are not intentionally producing or feigning them. Their distress and help-seeking behaviors are excessive relative to the medical findings, but the symptoms themselves are experienced as authentically present. No deception is involved. The key distinguishing feature is intentionality — somatic symptom disorder involves no intentional production of symptoms.
Illness Anxiety Disorder (Health Anxiety / Hypochondriasis): Preoccupation with having or acquiring a serious illness, with genuine (not produced) concern and persistent health-checking behaviors despite medical reassurance. The patient seeks reassurance but is not producing symptoms. Distinguishing from factitious disorder: the patient in illness anxiety disorder wants to be told they are healthy; the patient with factitious disorder typically resists normal findings and escalates toward more severe illness.
Malingering: Intentional feigning of illness for clear external gain — disability payments, legal defense, avoidance of military service or incarceration, or procurement of controlled substances. When the external incentive is identified and removed, the behavior typically ceases. Malingering is not a psychiatric disorder in DSM-5 (it appears in the "V-codes" as a condition that may be a focus of clinical attention). The distinction from factitious disorder can be subtle, as some patients have mixed motivations.
Conversion Disorder (Functional Neurological Symptom Disorder): Neurological symptoms — weakness, paralysis, non-epileptic seizures, sensory loss, blindness — that cannot be explained by structural neurological disease. The patient is not intentionally producing the symptoms; they arise from a disruption in neural function mediated by psychological mechanisms. Positive signs (Hoover's sign for functional leg weakness, for instance) distinguish it from structural disease without implying deception.
True rare diseases: This is perhaps the most clinically consequential differential. Conditions like systemic mastocytosis, pheochromocytoma, hereditary angioedema, acute intermittent porphyria, or rare autoimmune diseases can produce bizarre, episodic, difficult-to-document presentations that initially appear implausible or factitious. Factitious disorder is a diagnosis of exclusion — rare conditions must be seriously pursued before concluding that the patient is producing symptoms intentionally. Premature diagnosis of factitious disorder in a patient with an unrecognized rare disease is a serious medical error with significant ethical and legal consequences.
Epidemiology and Risk Factors
Factitious disorder is almost certainly far more common than published prevalence figures suggest. Reported estimates of 0.02–0.6% of medical inpatients reflect only those cases that are recognized and documented — a small fraction of all cases. The condition is particularly concentrated in specialty settings where complex, unexplained syndromes accumulate: gastroenterology, infectious disease, neurology, and hematology units all report higher proportions of suspected factitious presentations than general medical wards.
The structural barriers to accurate prevalence estimation are substantial. Patients move between hospitals when suspicion mounts, preventing any single institution from capturing the full pattern. Clinicians frequently avoid documenting factitious disorder in the medical record — out of uncertainty, concern about legal consequences, or reluctance to confront — leaving cases invisible in retrospective chart audits. And because confrontation often drives patients out of care rather than into documented psychiatric treatment, confirmed cases are a subset of recognized cases, which are themselves a subset of true cases.
A 3:1 female predominance is consistently reported in classic FDIS across large case series, though the reasons for this are not fully established. Mean age of onset is typically in young adulthood, with the condition often persisting across decades. Healthcare workers — nurses, medical assistants, phlebotomists, laboratory technicians — are substantially overrepresented, likely because they have both the knowledge to simulate convincing presentations and access to the materials (medications, blood, infectious material) needed to do so.
Established risk factors include: a history of genuine illness with hospitalization in childhood; a history of physical, emotional, or sexual abuse or neglect; comorbid personality disorder (borderline and antisocial personality disorder are most frequently identified); healthcare employment; poor social support and limited social identity outside of the sick role; and prior experiences in which illness generated unusually positive caregiver responses. The presence of multiple risk factors substantially increases clinical suspicion when unexplained presentations accumulate.
Legal and Ethical Considerations
Factitious disorder sits at the intersection of medicine, psychiatry, law, and ethics in ways that require clinicians to be thoughtful about obligations that extend beyond the individual therapeutic relationship.
FDIA as child abuse: Factitious Disorder Imposed on Another is legally classified as child abuse in virtually every U.S. state and in most international jurisdictions. Mandatory reporting obligations apply: any clinician who has reasonable suspicion — not proof — that a child is a victim of FDIA must report to child protective services. Failure to report when suspicion exists is itself a legal violation in most states. Child protective services involvement triggers a parallel legal track that is independent of the medical team's clinical conclusions.
Covert video surveillance in FDIA: When the clinical team has strong reason to believe FDIA is occurring and the child's safety is at immediate risk, covert video monitoring of the hospital room has been used to directly observe the caregiver's behavior. This approach is legally and ethically complex. Most institutions require ethics committee review and legal counsel authorization before implementation. State laws vary significantly in what constitutes lawful surveillance in this context. Courts have generally upheld the practice when child safety is the primary justification, but institutional policies must be consulted. The clinician's role is to document the clinical evidence, involve child protective services early, and allow the institutional ethics and legal framework to guide surveillance decisions — not to conduct covert monitoring independently.
Documentation for adult FDIS: For competent adults with Factitious Disorder Imposed on Self, there is no mandatory reporting obligation in most jurisdictions — adults have the right to make decisions about their own medical care, including refusing psychiatric treatment. However, clinicians have an ethical obligation to protect the patient from ongoing self-harm, to avoid performing unnecessary procedures on fabricated symptoms, and to document their clinical reasoning clearly and objectively. Chart entries should describe clinical observations and test findings in neutral, factual language without accusatory framing; the working diagnosis of factitious disorder should be documented with the clinical reasoning that supports it.
Insurance and fraud implications: When patients receive procedures, hospitalizations, or reimbursements for conditions they have intentionally fabricated, insurance fraud may occur. This has legal implications that clinicians are generally not positioned to adjudicate, but the documentation of factitious disorder in the medical record creates a legal record that may have downstream consequences. Clinicians should be aware of this dimension without allowing it to distort their primary obligation to the patient's welfare.
Ethical tensions in management: The intersection of patient autonomy, clinical paternalism, and harm reduction creates genuine ethical tension in managing FDIS in competent adults. Clinicians must balance: the patient's right to refuse psychiatric care; the obligation not to perform harmful unnecessary procedures; the duty to treat genuine medical conditions that arise; and the goal of keeping the patient engaged enough in care to eventually accept help. There are no universally correct answers — these tensions require case-by-case ethical reasoning with input from ethics consultation when the situation is unclear.
Key Research Papers
- Krahn LE et al. (2003). Patients who strive to be ill: factitious disorder with physical symptoms. Am J Psychiatry. Search PubMed
- Bass C, Halligan P. (2014). Factitious disorders and malingering: challenges for clinical assessment and management. Lancet. Search PubMed
- Feldman MD. (1994). Munchausen by proxy: a serious and misunderstood form of child abuse. Postgrad Med. Search PubMed
- Overbosch J et al. (2011). Factitious hypoglycemia and C-peptide levels. Neth J Med. Search PubMed
- Fliege H et al. (2007). Risk factors and phenomenology of perioperative factitious disorders. Gen Hosp Psychiatry. Search PubMed
- Eastwood S, Bisson JI. (2008). Management of factitious disorders: a systematic review. Psychother Psychosom. PMID 18552511
- Sutherland AJ, Rodin GM. (1990). Factitious disorders in a general hospital setting. Psychosomatics. Search PubMed
- Pankratz L. (1981). A review of the Munchausen syndrome. Clin Psychol Rev. (Foundational review.) PubMed Search
- Artingstall K. (1999). Practical aspects of Munchausen by Proxy and Munchausen syndrome investigation. CRC Press. (Key reference text.) PubMed Search
- Solyom AE, Austad CC. (1990). Factitious disorder. — Search PubMed
- Meadow R. (1977). Munchausen syndrome by proxy. The hinterland of child abuse. Lancet. PMID 70692
- Yates GP, Feldman MD. (2016). Factitious disorder: a systematic review of 455 cases in the professional literature. Gen Hosp Psychiatry. Search PubMed
Connections
- Psychiatry
- Somatic Symptom Disorder
- Conversion Disorder (FND)
- Borderline Personality Disorder
- Dissociative Identity Disorder
- Anxiety
- Depression
- PTSD
- Narcissistic Personality Disorder
- Addiction