Dementia: History and Discovery
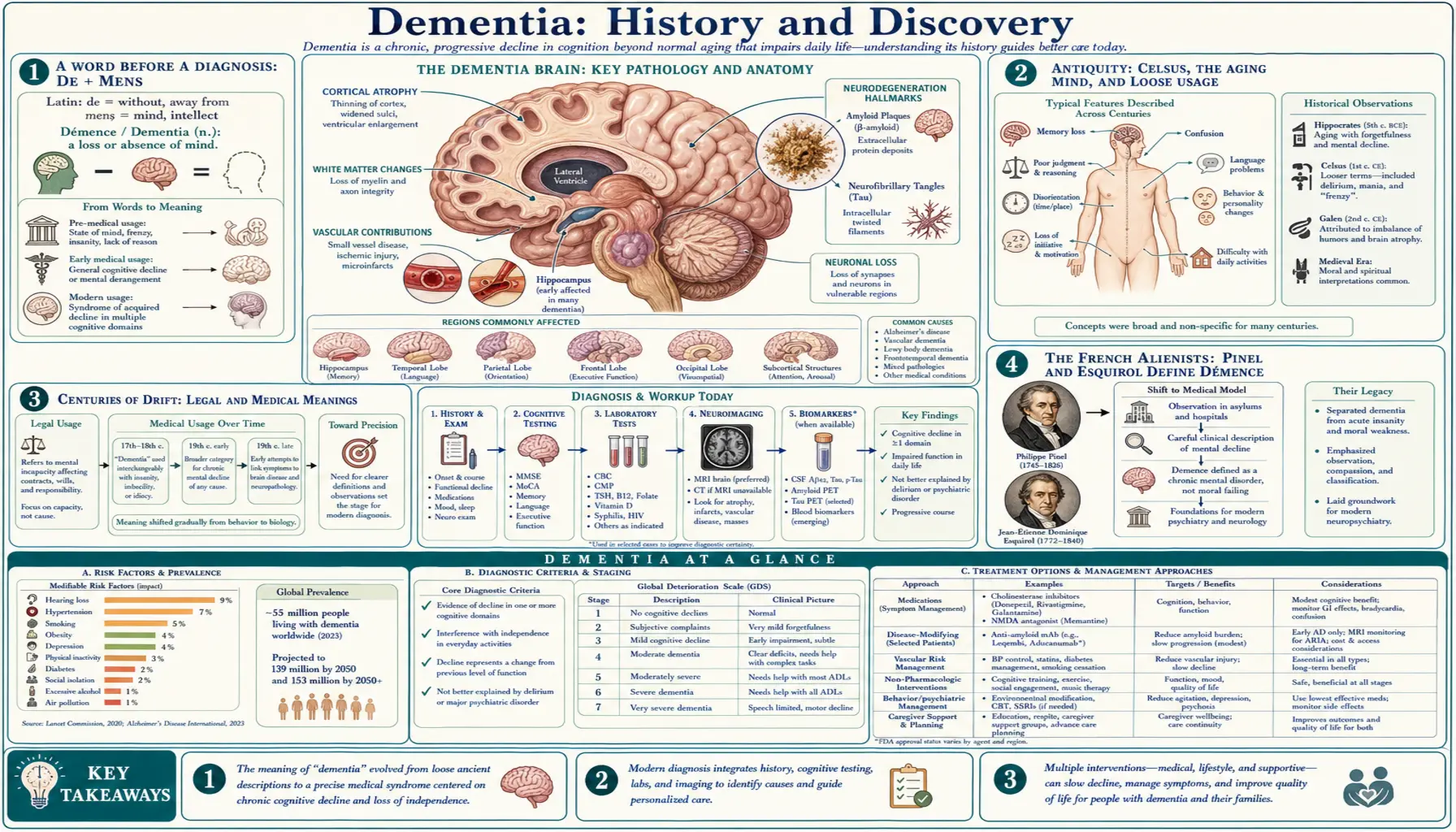
The word dementia comes from the Latin de- (out, away from) plus mens (mind) — literally “out of one’s mind.” For most of recorded history it was a loose label for madness or loss of reason at any age, not the specific condition we mean today. The modern medical meaning was forged in the early 1800s by French alienists, above all Jean-Étienne Dominique Esquirol, who defined démence as an acquired loss of intellectual function and carefully separated it from lifelong idiocy and from temporary delirium. The deepest change, though, came later: dementia is now understood not as a single disease but as a syndrome — a recognizable clinical picture of acquired cognitive decline — produced by many different causes, including Alzheimer’s disease (1906), vascular disease, Lewy body disease, and frontotemporal degeneration. This page traces that long journey from an ancient insult to a precise clinical syndrome, and the recent move toward the less stigmatizing term “major neurocognitive disorder.”
Table of Contents
- A Word Before a Diagnosis: De + Mens
- Antiquity: Celsus, the Aging Mind, and Loose Usage
- Centuries of Drift: Legal and Medical Meanings
- The French Alienists: Pinel and Esquirol Define Démence
- “Senile Dementia” and the Nineteenth-Century Brain
- From One Word to Many Causes
- Dementia as a Syndrome, Not a Disease
- DSM-5 and “Major Neurocognitive Disorder”
- Stigma, Language, and the Modern Picture
- Research Papers and References
- Connections
- Featured Videos
A Word Before a Diagnosis: De + Mens
Few medical terms wear their meaning so plainly. Dementia is built from the Latin preposition de- (out, away, down from) and the noun mens, mentis (mind), through the adjective demens — “out of one’s mind,” “mad,” “senseless.” The related Latin verb dementare meant “to drive mad.” In its original sense the word was not a clinical category at all but an everyday description of a person whose reason had departed, applicable to fury, raving, foolishness, or simple incapacity.
This origin matters because it shaped how the word behaved for two thousand years. A term that literally means “mindlessness” is broad by design: it can attach to a child, a fever patient, a person in a rage, or a frail elder, with no implication about cause, age, or whether the state will pass. The precise, narrow modern meaning — an acquired, usually progressive loss of memory and thinking from brain disease — is a comparatively recent achievement laid on top of this old, capacious word.
It is worth keeping three distinct things separate as the history unfolds: the word “dementia” and how its usage shifted; the medical concept of an acquired decline of the intellect; and the underlying diseases of the brain that we now know produce that decline. These three threads were tangled together for most of history and only pulled apart, one at a time, over the last two centuries.
Antiquity: Celsus, the Aging Mind, and Loose Usage
The Latin term and its cognates appear in classical writing. The Roman encyclopedist Aulus Cornelius Celsus (first century CE), in his medical work De Medicina, used cognate language in describing disorders of the mind, and later historians of psychiatry have pointed to phrases such as dementia in connection with the aftermath of phrenesis (delirium). Historians caution, however, that the surviving usage is loose and that attributing a fixed clinical term to Celsus overstates the case; the word at this stage names a state of mindlessness, not a defined disease. We therefore describe Celsus and his contemporaries as using the cognate term in its broad ancient sense rather than crediting any single “first” description of the modern syndrome.
Greco-Roman physicians and philosophers nonetheless observed, repeatedly, that memory and judgment often fade in old age. From Pythagoras and Hippocrates through Plato, Aristotle, Cicero, and Galen, classical authors discussed the decline of the mind in the elderly — sometimes treating it as an inevitable companion of aging, sometimes (as in Cicero’s De Senectute) arguing that decline could be resisted by an active, disciplined mind. What they did not do was carve out senile cognitive decline as a specific medical disease distinct from ordinary aging; that distinction lay far in the future.
So the ancient inheritance is twofold and somewhat contradictory: a word meaning generic madness or mindlessness, and a separate, widely shared observation that the aging brain commonly loses its powers. The history of dementia is, in large part, the slow work of bringing those two things together into a single, sharply defined idea — and then, much later, splitting that idea open to reveal the many diseases beneath it.
Centuries of Drift: Legal and Medical Meanings
Through the medieval and early-modern centuries the term continued in a wide, imprecise sense. The historian of psychiatry German E. Berrios, in his influential conceptual histories, showed that before the nineteenth century “dementia” carried two overlapping meanings: a legal one and a medical one. The legal meaning — concerning a person’s incapacity to manage their affairs, make contracts, or stand trial — sharpened during the seventeenth century, as courts needed language for unsound mind. The narrower medical meaning, an enduring impairment of the intellectual faculties, took clearer shape during the eighteenth century.
Crucially, in this older usage dementia was not tied to old age and not necessarily irreversible. It could describe intellectual weakness arising at any time of life and from many situations — including states we would now call delirium, intellectual disability, or the end stages of other mental illnesses. Eighteenth-century nosologists who tried to classify diseases of the mind placed “dementia” or its equivalents among the disorders of reason, but without the modern requirements of acquired, progressive, age-associated brain decline.
This long interval of drift is easy to underrate, yet it is the essential backdrop to what followed. By 1800 the word was centuries old, widely used in law, philosophy, and medicine, and meant something like “a settled loss of reason.” It was precisely this vague, capacious term that the French alienists inherited — and proceeded to discipline into a clinical concept.
The French Alienists: Pinel and Esquirol Define Démence
The turn of the nineteenth century brought the reforms and the systematic disease-classification that gave dementia its modern shape. Philippe Pinel (1745–1826), a central figure in the humane reform of the asylums and author of the Traité médico-philosophique sur l’aliénation mentale (1801), placed démence — which he associated with an “abolition of thought” — among his principal categories of mental alienation, alongside mania, melancholia, and idiocy. Pinel’s framework began to treat the loss of intellectual function as a definable clinical state rather than mere madness.
It was Pinel’s student Jean-Étienne Dominique Esquirol (1772–1840) who did the decisive work. In his contributions to the Dictionnaire des sciences médicales from around 1814 and, most fully, in his landmark treatise Des maladies mentales (1838), Esquirol defined démence as an acquired weakening of the intellectual faculties — a loss of reasoning, memory, and judgment in a mind that had once possessed them. With this single criterion, “acquired,” he separated dementia from two neighbors with which it had long been confused.
First, he distinguished it from amentia / idiocy (what he called idiotie): in idiocy the intellect never properly develops, whereas in dementia a fully formed intellect is lost. In his memorable formulation, the person with dementia is “deprived of advantages they once enjoyed,” a rich person become poor, while the person with idiocy was always in want. Second, he separated chronic dementia from delirium (and acute, reversible confusional states), distinguishing the lasting erosion of intellect from a transient clouding of consciousness. Esquirol further subdivided dementia into acute (potentially reversible), chronic, and senile forms — an early recognition that “dementia” covered more than one situation.
“Senile Dementia” and the Nineteenth-Century Brain
Esquirol’s category of senile dementia — the failure of mind occurring in old age — took firm hold over the nineteenth century, and the English phrase “senile dementia” entered medical usage by the 1820s. For the first time, the age-old observation that the elderly often lose their faculties was joined to a defined clinical term, and “senile dementia” became the standard name for the dementia of later life. Much of the century’s effort went into describing its course and, increasingly, into asking what in the body produced it.
The nineteenth century’s great contribution was to relocate the cause of dementia firmly inside the brain. As pathology and microscopy advanced, physicians sought the physical lesions underlying mental decline. A dominant nineteenth- and early-twentieth-century theory attributed much senile decline to hardening of the brain’s arteries — “arteriosclerotic” or cerebrovascular disease starving the brain of blood. The German psychiatrist Otto Binswanger described a form of vascular white-matter disease (later bearing his name) in the 1890s, and Emil Kraepelin, in his influential textbook, recognized “arteriosclerotic dementia” among the dementias of later life.
This vascular emphasis is historically important for a reason that goes beyond its own correctness: it was the first widely accepted attempt to assign a specific bodily cause to a dementia, and it implicitly opened the door to the modern idea that different dementias might have different causes in the brain. For decades, in fact, “hardening of the arteries” was the popular catch-all explanation for senility — a notion later revised as the central role of degenerative brain diseases like Alzheimer’s became clear, even as genuine vascular dementia remained a real and major cause in its own right.
From One Word to Many Causes
The early twentieth century shattered the assumption that “senile dementia” was one thing. In 1906, the German psychiatrist and neuropathologist Alois Alzheimer presented the case of Auguste Deter — a woman in her fifties with profound memory loss and confusion — at a conference in Tübingen, describing the plaques and neurofibrillary tangles he had found in her brain; the paper, Über eine eigenartige Erkrankung der Hirnrinde, appeared in 1907. Around 1910, Alzheimer’s chief Emil Kraepelin named the condition “Alzheimer’s disease” in the eighth edition of his textbook, initially as a striking presenile form. (Alzheimer’s disease has its own dedicated page on this site.)
Other distinct diseases that cause dementia were identified in the same era and after. Arnold Pick described, from 1892 onward, the focal frontal and temporal lobe atrophy underlying what became Pick’s disease — the historical root of today’s frontotemporal dementia. Friedrich (Frederic) Lewy, working in Alzheimer’s Munich laboratory, described the abnormal neuronal inclusions now called Lewy bodies in 1912; these would later be recognized as the hallmark of dementia with Lewy bodies and a key feature of Parkinson’s disease dementia. Alongside these degenerative diseases stood vascular (multi-infarct) dementia and many secondary causes — from chronic alcohol use and thyroid disease to vitamin B12 deficiency, infections, and normal-pressure hydrocephalus.
The cumulative lesson was transformative: the single nineteenth-century box labeled “senile dementia” in fact contained many different diseases, each with its own pathology, course, and (where it exists) treatment. “Dementia” was no longer the diagnosis — it was the description of a problem whose diagnosis still had to be made. It is also now understood that these pathologies frequently coexist in the same brain, especially in older people: “mixed dementia,” with both Alzheimer and vascular or Lewy-body changes together, is common rather than exceptional.
Dementia as a Syndrome, Not a Disease
The realization that dementia has many causes produced the single most important conceptual shift in this whole history: dementia is a syndrome, not a disease. A syndrome is a recognizable pattern of signs and symptoms that can arise from more than one underlying cause. The dementia syndrome is, in essence, an acquired, persistent decline in two or more domains of thinking — memory, language, attention, executive function, visuospatial skill, social cognition — severe enough to interfere with everyday independent living, and not explained by a temporary delirium.
Framing dementia this way clarifies much that earlier confusion obscured. It explains why dementia must be acquired (Esquirol’s old criterion, distinguishing it from lifelong intellectual disability); why it must be persistent and not a passing fog (distinguishing it from delirium); and why diagnosing “dementia” is only the first step, after which the clinician asks the truly important question: which disease is causing it? The answer determines prognosis, family counseling, and whether any cause is treatable or reversible.
This syndrome-and-causes model is the framework taught and used in medicine today. It rescues the term from its ancient vagueness by giving it precise clinical criteria, while honestly acknowledging that the criteria describe a final common pathway reached by many roads. Dementia, in the modern sense, is best understood as the shared destination of a family of brain diseases — not a single illness with a single cause or a single cure.
DSM-5 and “Major Neurocognitive Disorder”
The most recent chapter is a deliberate change of language. When the American Psychiatric Association published the fifth edition of its Diagnostic and Statistical Manual of Mental Disorders (DSM-5) in 2013, it retired “dementia” as a formal diagnostic heading and replaced it with “major neurocognitive disorder” (with a paired, milder category, “mild neurocognitive disorder,” corresponding roughly to what had been called mild cognitive impairment). The manual organized these as a single “neurocognitive disorders” group, further specified by the suspected cause — for example, “major neurocognitive disorder due to Alzheimer’s disease.”
Two motives drove the change. The first was stigma: because “dementia” translates roughly as “out of one’s mind” or “loss of mind,” many clinicians, patients, and advocates found it pejorative and frightening, and proposals to retire it had been published in the years before DSM-5. The second was structure: the “major / mild” pairing and the “due to…” specifier neatly express the modern syndrome-with-many-causes model and add an explicit milder tier for earlier-stage impairment. DSM-5 notably retained the word “dementia” as an acceptable alternative in settings where it is customary, rather than banning it outright.
In practice, usage today is mixed. “Dementia” remains the dominant everyday and clinical term worldwide — it is used by patients, families, the World Health Organization, and most national health services — while “major neurocognitive disorder” is the formal DSM-5 label and is gaining ground in research and documentation. Both names point to the same thing: the syndrome of acquired cognitive decline whose definition this two-century history slowly built.
Stigma, Language, and the Modern Picture
Looking back, the history of dementia is a story of a word being tamed and then a concept being opened up. An ancient term for generic madness — de + mens, “out of one’s mind” — was disciplined by Pinel and Esquirol into a clinical category of acquired intellectual decline; given a physical home in the brain by nineteenth-century pathology; and then revealed, through the work of Alzheimer, Pick, Lewy, and the students of cerebrovascular disease, to be not one illness but the shared face of many. The final move, from “dementia” toward “major neurocognitive disorder,” is an attempt to shed the old word’s sting while keeping the hard-won precision.
The shift away from the stigmatizing older usage is more than cosmetic. For centuries the word lumped the dignified frailty of an aging mind together with raving and foolishness; modern language tries instead to name a medical condition with an identifiable cause, a definable course, and — increasingly — specific care. Person-first language (“a person living with dementia”) and disease-specific naming both reflect the same impulse: to describe what is actually happening in the brain without reducing the person to a label.
For readers and families, the practical takeaways of this history are clear. “Dementia” is a description, not a diagnosis; behind it lies a specific cause that should be sought, because some causes are treatable or even reversible. It is not a normal, inevitable part of aging, however common it becomes with age. And the steady refinement of the concept — from an ancient insult to a syndrome with named, studied causes — is exactly what makes accurate diagnosis, honest information, and humane care possible today.
Research Papers and References
The references below combine peer-reviewed conceptual histories of dementia with curated PubMed topic-search links into the historical and biographical literature. Historical primary texts — Celsus’s De Medicina, Pinel’s Traité médico-philosophique (1801), Esquirol’s Des maladies mentales (1838), Kraepelin’s Psychiatrie, and Alzheimer’s 1907 case report — are named in the article as historical sources rather than as modern citations. Links open at the publisher, PubMed, or PMC (National Library of Medicine) in a new tab. Where a confident DOI or PMID was not established, a PubMed topic-search link is given instead.
- Berrios GE. Dementia during the seventeenth and eighteenth centuries: a conceptual history. Psychological Medicine. 1987;17(4):829–837. — doi:10.1017/S0033291700000623 (PMID: 3324141)
- Berchtold NC, Cotman CW. Evolution in the conceptualization of dementia and Alzheimer’s disease: Greco-Roman period to the 1960s. Neurobiology of Aging. 1998;19(3):173–189. — doi:10.1016/S0197-4580(98)00052-9 (PMID: 9661992)
- Roman GC. A historical review of the concept of vascular dementia: lessons from the past for the future. Alzheimer Disease & Associated Disorders. 1999. — PMID: 10609675
- Trachtenberg DI, Trojanowski JQ. Should the word ‘dementia’ be forgotten? Journal of Cellular and Molecular Medicine. 2010;14(11):2585–2588. — doi:10.1111/j.1582-4934.2010.01159.x (PMID: 20731751)
- Hippius H, Müller N. The discovery of Alzheimer’s disease. Dialogues in Clinical Neuroscience. 2003;5(1):101–108. — PMC3181715
- Yang HD, Kim DH, Lee SB, Young LD. History of Alzheimer’s disease. Dementia and Neurocognitive Disorders. — PubMed: history of Alzheimer’s disease (Auguste Deter, Kraepelin)
- Esquirol and dementia — biographical and conceptual review — PubMed: Esquirol and dementia (PMID 22586818)
- Pinel, Esquirol, and the birth of the French clinical concept of démence — PubMed: Pinel, Esquirol and the history of démence
- DSM-5 neurocognitive disorders — major and mild, replacing “dementia” — PubMed: DSM-5 major neurocognitive disorder terminology
- History and conceptual evolution of vascular and arteriosclerotic dementia (Binswanger, Kraepelin) — PubMed: history of vascular dementia
- Frederic Lewy, Lewy bodies, and the history of Lewy body dementia — PubMed: Frederic Lewy and the history of Lewy body dementia
- Arnold Pick, Pick’s disease, and the history of frontotemporal dementia — PubMed: Arnold Pick and the history of frontotemporal dementia
- Senile dementia in antiquity — Greco-Roman views of the aging mind — PubMed: senile dementia in antiquity
- Etymology and conceptual history of the term “dementia” (Celsus to modern usage) — PubMed: history of the term “dementia”
External Authoritative Resources
- National Institute on Aging (NIA) — Alzheimer’s and Dementia
- World Health Organization — Dementia fact sheet
- PubMed — Conceptual history of dementia
Connections
- Psychiatry
- Dementia (overview)
- All Conditions
- Alzheimer’s Disease
- Parkinson’s Disease
- Huntington’s Disease
- Depression