ADHD: History and Discovery
Attention-deficit/hyperactivity disorder is often described in the press as a recent or even invented condition, but careful physicians have been recording its core features — restless inattention, impulsivity, and difficulty with self-regulation in otherwise capable children — for more than two hundred years. This page traces that documented history honestly: from Sir Alexander Crichton's 1798 account of a "mental restlessness," through Sir George Frederic Still's influential 1902 lectures, to Charles Bradley's accidental 1937 discovery that a stimulant could calm and focus difficult children, and on through the long evolution of the diagnostic name from "minimal brain dysfunction" to today's "ADHD." Where the record is uncertain or has been re-interpreted by later scholars, this page says so plainly, and it uses non-stigmatizing language throughout.
Table of Contents
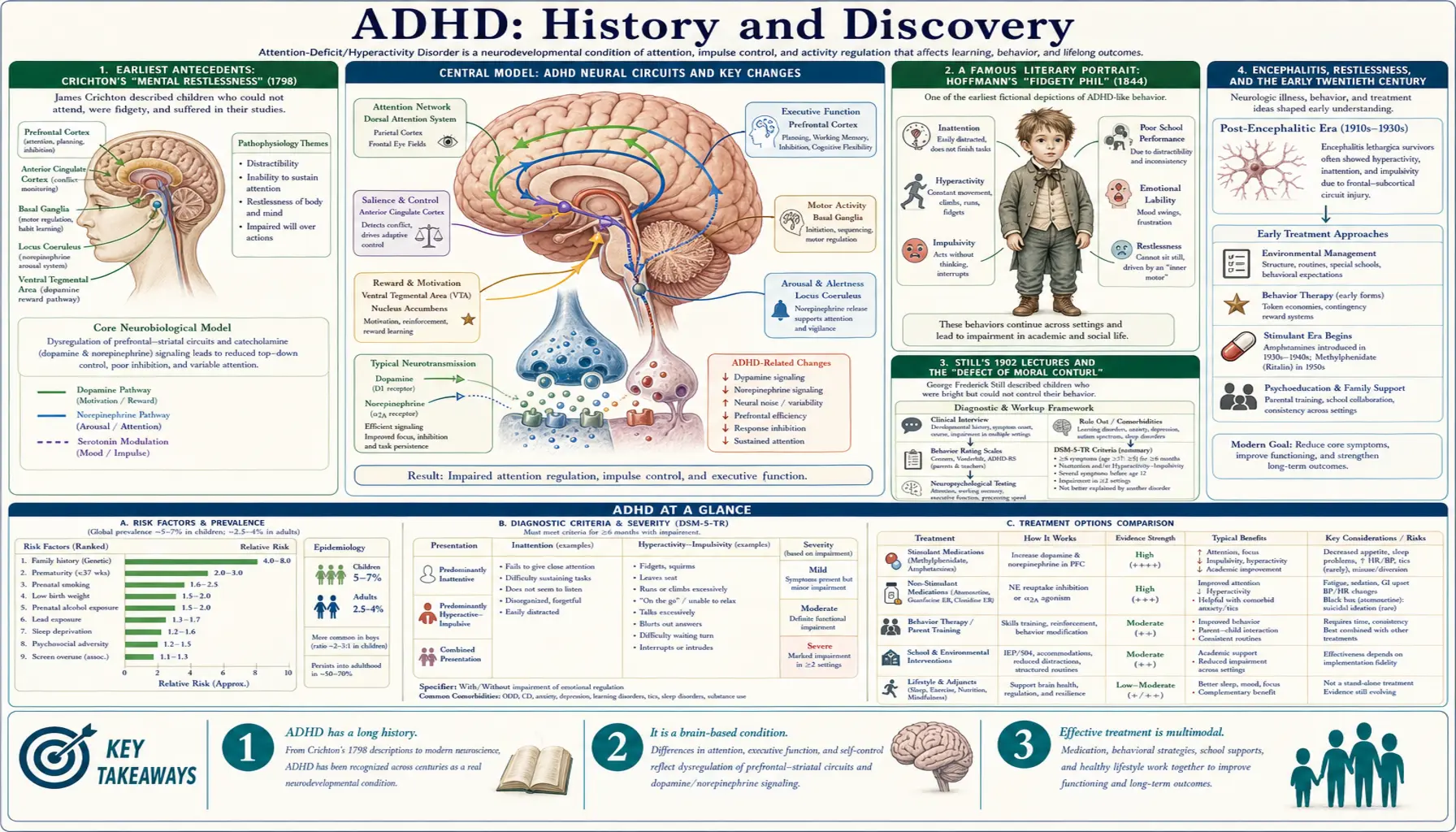
- Earliest Antecedents: Crichton's "Mental Restlessness" (1798)
- A Famous Literary Portrait: Hoffmann's "Fidgety Phil" (1844)
- Still's 1902 Lectures and the "Defect of Moral Control"
- Encephalitis, Restlessness, and the Early Twentieth Century
- Bradley's Accidental Discovery: Stimulants (1937)
- The Evolving Name: From MBD to ADHD
- Methylphenidate, the Modern Era, and Lifelong ADHD
- How the Understanding of ADHD Changed
- Research Papers and References
- Connections
- Featured Videos
Earliest Antecedents: Crichton's "Mental Restlessness" (1798)
The earliest detailed medical description that modern scholars connect to ADHD comes from the Scottish-born physician Sir Alexander Crichton (1763–1856). In 1798 he published a two-volume work, An Inquiry into the Nature and Origin of Mental Derangement, which included a chapter on attention and its disorders. There Crichton described people in whom "every impression seems to agitate the person, and gives him or her an unnatural degree of mental restlessness," leaving them unable to hold their attention steadily on any one object.
What makes Crichton's account striking to later readers is how many of the features now associated with the inattentive picture of ADHD he gathered together: distractibility, fidgety restlessness, an onset early in life, and a recognition that the difficulty interfered with schooling. He also noted, with unusual compassion for his era, that such children "require a great deal of attention," and that the restlessness sometimes lessened with age. Crucially, he framed this as a difficulty of attention rather than as a moral or character failing — a tone the field would not fully recover for nearly two centuries.
Crichton's primary text is named here as a historical source rather than a modern citation. Although he did not use any term resembling "ADHD" and was describing what he saw clinically rather than defining a discrete disorder, the 1798 chapter is now widely cited as the first clear, sympathetic medical antecedent of the condition, predating the more famous twentieth-century accounts by more than a hundred years.
A Famous Literary Portrait: Hoffmann's "Fidgety Phil" (1844)
One of the most frequently reproduced images in the popular history of ADHD is not a medical document at all but a children's picture book. The German physician Heinrich Hoffmann (1809–1894) wrote and illustrated a collection of cautionary rhymes, Der Struwwelpeter, which he created as a Christmas gift for his young son in 1844 and published in 1845. One of its tales, "Die Geschichte vom Zappel-Philipp" ("The Story of Fidgety Philip"), describes a boy who cannot sit still at the dinner table, rocks on his chair, and finally pulls the tablecloth, dishes, and dinner crashing down with him.
Because the verse captures the restless, impulsive squirming so familiar to parents and teachers, "Fidgety Phil" is often invoked as an early depiction of hyperactivity — and in Germany ADHD is still sometimes called Zappelphilipp-Syndrom colloquially. It is important to be accurate about what this is and is not. Hoffmann was indeed a physician who later worked in psychiatry, but the poem was written as a humorous moral tale about a child misbehaving at the table, not as a clinical description or a medical "first." The reading of Fidgety Phil as an ADHD case study is a modern, retrospective interpretation laid onto a nineteenth-century children's rhyme.
The story endures in the ADHD narrative for a simpler reason: it shows that the behaviour pattern itself — a bright, lively child who genuinely cannot keep still — was recognizable and commonplace long before there was any diagnosis for it. As a piece of cultural history it is genuine and charming; as evidence of how ADHD was once understood medically, it should be read with care.
Still's 1902 Lectures and the "Defect of Moral Control"
The account most often cited as the foundational clinical description of ADHD belongs to the English paediatrician Sir George Frederic Still (1868–1941), frequently called the father of British paediatrics. In March 1902 Still delivered the Goulstonian Lectures to the Royal College of Physicians in London, published the same year in The Lancet under the title "Some Abnormal Psychical Conditions in Children." Drawing on a series of roughly forty-three children he had seen in practice, he described youngsters of apparently normal intellect who nonetheless showed a striking inability to sustain attention, were impulsive, over-emotional, and could not seem to learn from the consequences of their behaviour.
Still grouped these traits under what he called a "defect of moral control." By "moral control" he meant something closer to the capacity to regulate one's own conduct in line with the good of others — in modern terms, self-regulation and inhibition — rather than a judgement that the children were wicked. He explicitly observed "a quite abnormal incapacity for sustained attention" in many of these cases, and he suspected a biological rather than purely environmental basis, noting that the pattern sometimes ran in families and could follow illness or injury.
Modern historians treat Still's lectures as a genuine landmark while also reappraising exactly what he described. His sample was a clinically mixed group that, by today's standards, would likely include children with ADHD alongside others with conduct disorder, the aftermath of brain injury, and various developmental conditions; it was not a clean description of ADHD as currently defined. The phrase "defect of moral control," however well intentioned, also helped seed a long and damaging tendency to frame these children as morally deficient. Still's lasting contribution was to insist that such difficulties were real, often constitutional, and deserving of medical study — not simply the products of bad parenting or bad character.
Encephalitis, Restlessness, and the Early Twentieth Century
In the decades after Still's lectures, a dramatic public-health event reinforced the idea that restless, inattentive, impulsive behaviour could have a physical cause. The worldwide epidemic of encephalitis lethargica ("sleeping sickness") that followed the First World War left many surviving children with marked changes in behaviour — restlessness, impulsivity, irritability, and difficulty concentrating — in the absence of obvious intellectual loss. Clinicians began describing a "post-encephalitic behaviour disorder," and the resemblance to the children Still had portrayed was hard to miss.
This experience encouraged a broader and influential assumption: that a similar behavioural picture in children who had not had a documented brain infection might still reflect some subtle, perhaps undetectable, brain abnormality. Through the 1930s, 1940s, and 1950s this reasoning gave rise to labels such as "organic drivenness," "minimal brain damage," and eventually "minimal brain dysfunction," discussed in the naming section below. The intuition that the disorder was biological was, in broad strokes, on the right track; the specific theory — that every such child must have suffered actual brain damage — was an over-reach that later evidence did not support.
It was against this backdrop of intense interest in childhood behaviour and its possible neurological roots that the single most consequential observation in the history of ADHD treatment was about to be made — and, characteristically for this field, it would happen entirely by accident.
Bradley's Accidental Discovery: Stimulants (1937)
In 1937 the American psychiatrist Charles Bradley (1902–1979) made the discovery that would eventually transform the treatment of ADHD. Bradley was medical director of the Emma Pendleton Bradley Home in Providence, Rhode Island, a residential centre for children with neurological and behavioural problems. Many of these children were undergoing pneumoencephalography — a then-common but punishing diagnostic procedure in which spinal fluid was replaced with air so the brain could be X-rayed — and they suffered severe headaches afterward as a result.
Hoping to relieve those headaches, Bradley gave the children Benzedrine, a brand of amphetamine. It did little for the headaches. What it did do astonished the staff: a substantial number of the children became noticeably calmer, better behaved, and far more able to concentrate, with what Bradley described as a striking improvement in their school work and a new "drive to accomplish." He reported the findings that year in a paper titled "The Behavior of Children Receiving Benzedrine" in the American Journal of Psychiatry.
The result seemed paradoxical — a stimulant making over-active children calmer — and that apparent paradox is part of why Bradley's work was admired but largely set aside for roughly two decades before child psychiatry returned to it in earnest. Modern neuroscience no longer regards the effect as paradoxical at all: stimulant medications increase the availability of the neurotransmitters dopamine and noradrenaline in brain networks that govern attention and impulse control, improving focus in people with and without ADHD alike. Bradley himself was notably cautious and humane, stressing that medication was only one part of a child's care. His 1937 observation remains the direct ancestor of every stimulant prescribed for ADHD today.
The Evolving Name: From MBD to ADHD
Perhaps nothing illustrates the changing understanding of this condition better than the long series of names it has carried. None of these were arbitrary rebrandings; each shift reflected a real change in what clinicians believed lay at the heart of the disorder. In the middle of the twentieth century the favoured label was "minimal brain dysfunction" (MBD). This term was a deliberate retreat from the earlier "minimal brain damage": as it became clear that most affected children had no demonstrable brain injury, researchers softened "damage" to "dysfunction" to describe a presumed subtle disturbance of function rather than visible harm.
The condition entered the official American diagnostic system in stages. The second edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-II, 1968) listed it as "hyperkinetic reaction of childhood," a name that put over-activity — hyperkinesis — at the centre of the picture. The next major revision changed the emphasis decisively. DSM-III (1980) introduced the term "attention deficit disorder" (ADD), explicitly recognizing that the attention problem, not just the physical restlessness, was the core feature; it allowed the diagnosis to be made "with or without hyperactivity," acknowledging that some children struggled to focus without being visibly over-active.
The revised third edition, DSM-III-R (1987), merged these into a single category and gave the disorder the name still in use today: attention-deficit/hyperactivity disorder (ADHD). DSM-IV (1994) kept the name but defined three presentations — predominantly inattentive, predominantly hyperactive-impulsive, and combined — reflecting the recognition that the condition looks quite different from one person to the next. The current DSM-5 (2013) retained ADHD and its presentations but moved it into the "neurodevelopmental disorders" chapter, raised the age-of-onset threshold from before age 7 to before age 12, and adjusted the criteria so that the diagnosis could be applied appropriately to adolescents and adults rather than children alone.
Methylphenidate, the Modern Era, and Lifelong ADHD
After Bradley's 1937 report, the pharmacological side of the story advanced through a new generation of stimulants. The compound methylphenidate was first synthesized in 1944 by the chemist Leandro Panizzon and was marketed from the mid-1950s under the brand name Ritalin. Over the 1960s and 1970s, as controlled trials accumulated and the diagnosis was formalized in the DSM, methylphenidate and amphetamine-based medicines became the mainstay of treatment for what was then called hyperkinetic reaction and later ADD/ADHD, used alongside behavioural and educational support rather than in place of it.
Two larger conceptual shifts shaped the modern era. The first was the gradual realization, from the 1970s onward, that ADHD frequently does not disappear at adulthood. For much of the twentieth century it was regarded as a childhood condition that children grew out of; long-term follow-up studies showed instead that, while overt hyperactivity often fades, problems with attention, organization, and impulse control commonly persist into adult life. This understanding is reflected in the DSM-5 criteria and in the now-routine diagnosis and treatment of adults. The second shift was the steady accumulation of evidence — from genetics, family studies, and brain imaging — that ADHD is a highly heritable neurodevelopmental condition involving differences in the brain's dopamine and noradrenaline systems and in networks supporting attention and executive function.
This page describes that history rather than offering medical advice. ADHD is a real, well-studied, and treatable condition, and decisions about diagnosis or medication belong with a qualified clinician who knows the individual. The companion ADHD overview covers current symptoms, evaluation, and management in more detail.
How the Understanding of ADHD Changed
Seen as a whole, the two-century arc of this history is a story of an idea slowly being clarified and, importantly, de-moralized. Crichton in 1798 described a difficulty of attention with sympathy. Still in 1902 made it a subject of serious medical study but framed it, unfortunately, as a "defect of moral control" — a phrase that helped fasten a long-lasting and unfair stigma onto children who were, in fact, struggling with their neurology rather than their character. The early-twentieth-century encephalitis experience and the "minimal brain" era pushed the explanation back toward biology, sometimes over-confidently.
The modern view, built on Bradley's pharmacological clue and decades of subsequent research, holds ADHD to be a neurodevelopmental condition: a difference in how attention-, motivation-, and impulse-regulating brain systems develop and function, strongly influenced by genetics, present from early life, and frequently lasting into adulthood. Just as importantly, the language has shifted away from blame. Where earlier eras spoke of moral defect or brain damage, current clinical and advocacy communities emphasize that ADHD describes a real pattern of difficulty — and, for many people, of distinctive strengths — that responds to understanding, accommodation, and appropriate treatment.
That change in framing is not merely cosmetic. How a condition is named and explained shapes how the people who have it are treated by schools, workplaces, families, and the health system. The history of ADHD is, in the end, as much a history of attitudes as of medicine: a gradual movement from judging children for what they could not help, toward understanding and supporting them.
Research Papers and References
The references below combine key peer-reviewed historical reviews with curated PubMed topic-search links into the literature on the history and diagnosis of ADHD. Historical primary texts — Crichton's An Inquiry into the Nature and Origin of Mental Derangement (1798), Hoffmann's Der Struwwelpeter (1845), and Still's 1902 Goulstonian Lectures — are named in the article as historical sources. Each link opens at its source (PubMed, PMC, or the publisher) in a new tab.
- Bradley C. The behavior of children receiving Benzedrine. American Journal of Psychiatry. 1937;94(3):577–585. — doi:10.1176/ajp.94.3.577
- Strohl MP. Bradley's Benzedrine studies on children with behavioral disorders. Yale Journal of Biology and Medicine. 2011;84(1):27–33. — PMC3064242 (PMID 21451781)
- Palmer ED, Finger S. An early description of ADHD (inattentive subtype): Dr Alexander Crichton and "mental restlessness" (1798). Child Psychology and Psychiatry Review. 2001;6(2):66–73. — doi:10.1111/1475-3588.00324
- Lange KW, Reichl S, Lange KM, Tucha L, Tucha O. The history of attention deficit hyperactivity disorder. ADHD Attention Deficit and Hyperactivity Disorders. 2010;2(4):241–255. — doi:10.1007/s12402-010-0045-8
- Still GF. Some abnormal psychical conditions in children: the Goulstonian Lectures. The Lancet. 1902;159(4102):1008–1012. — PubMed: Still 1902 Goulstonian Lectures
- Sir George Frederic Still and the history of ADHD — PubMed: Still, moral control, and ADHD history
- Crichton and the early history of attention disorders — PubMed: Crichton 1798 and attention disorders
- Evolution of the ADHD diagnosis across DSM editions — PubMed: ADHD and the history of DSM criteria
- Encephalitis lethargica and post-encephalitic behaviour disorder in children — PubMed: encephalitis lethargica and childhood behaviour
- History of stimulant treatment for ADHD (amphetamine and methylphenidate) — PubMed: history of stimulant treatment for ADHD
- Heritability and neurodevelopmental basis of ADHD — PubMed: heritability and neurobiology of ADHD
- Persistence of ADHD into adulthood: long-term follow-up — PubMed: ADHD persistence into adulthood
- Stigma, language, and changing conceptions of ADHD — PubMed: stigma and the changing conception of ADHD
- Hoffmann's "Fidgety Philip" (Zappelphilipp) in the cultural history of ADHD — PubMed: Fidgety Philip and ADHD history
External Authoritative Resources
- National Institute of Mental Health (NIMH) — ADHD
- CHADD — About ADHD (Children and Adults with ADHD)
- Overview: History of ADHD (encyclopedic summary)