Rotator Cuff Tear
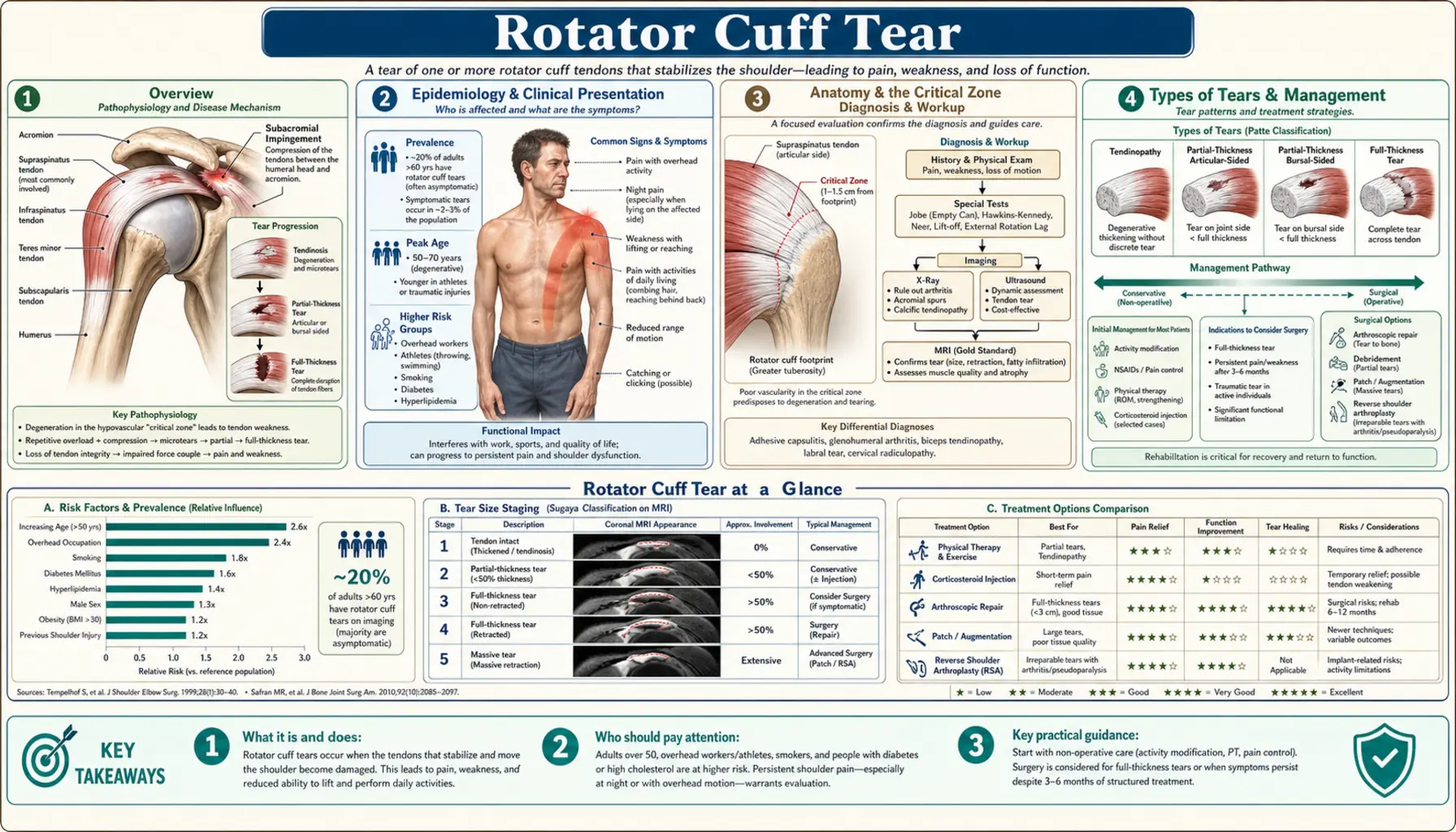
Table of Contents
- Overview
- Epidemiology
- Anatomy and Tendon Anatomy
- Types of Tears
- Clinical Presentation and Special Tests
- Diagnosis
- Treatment Options
- Surgical Management
- Complications and Outcomes
- References & Research
- Research Papers
- Connections
- Featured Videos
1. Overview
The rotator cuff is the workhorse of the shoulder — a group of four muscles and their tendons that wrap around the humeral head, keeping the ball pressed firmly into the socket while allowing the arm to move in nearly every direction. When one or more of those tendons tears, the shoulder loses both its stability and its strength. A rotator cuff tear is one of the most common soft-tissue injuries in adults, affecting an estimated one in five people over age 60, and it is the leading cause of shoulder pain and disability in the working-age population.
What makes rotator cuff tears complicated is that they exist on a wide spectrum — from a small fraying of fibers that causes only mild aching to a complete rupture of one or more tendons that leaves the arm nearly unable to lift overhead. Many tears, particularly partial-thickness ones, can be managed successfully without surgery through targeted physical therapy and judicious use of injections. Full-thickness tears in active patients, especially those that are symptomatic and progressive, usually require arthroscopic repair to restore durable function. Understanding where a specific tear falls on that spectrum is the first and most important step in choosing the right treatment path.
2. Epidemiology
Rotator cuff pathology is extraordinarily common. Cadaveric studies consistently find full-thickness tears in roughly 20–30% of the general population, with rates climbing sharply with age — from under 10% in people under 50 to more than 50% in those over 80. Importantly, many of these anatomic tears are asymptomatic; the mere presence of a tear on imaging does not mean it is causing the patient's pain or functional limitation.
Among symptomatic tears, several epidemiologic patterns stand out:
- Age is the dominant risk factor. Degenerative tears caused by cumulative micro-damage to the tendon's watershed zone dominate after age 60. The supraspinatus tendon, which passes through the narrowest part of the subacromial space, is by far the most frequently torn.
- Overhead workers and athletes at elevated risk. Painters, carpenters, swimmers, baseball pitchers, and tennis players sustain high repetitive loads on the rotator cuff tendons and develop symptomatic tears at higher rates than the general population.
- Traumatic tears in younger patients. An acute fall on an outstretched arm or a sudden eccentric force — catching a heavy load, bracing against a fall — can tear an otherwise healthy tendon in a patient under 50. These traumatic tears are less common but tend to be larger and more disabling than their degenerative counterparts.
3. Anatomy and the Critical Zone
Four muscles form the rotator cuff, each contributing a distinct mechanical role:
- Supraspinatus initiates and assists shoulder abduction (lifting the arm away from the body) and is the most commonly torn tendon. It passes beneath the acromion and the coracoacromial ligament through the subacromial space. Its distal tendon has a region of relative avascularity — the so-called "critical zone" — approximately 1 cm from its insertion on the greater tuberosity. Blood supply in this zone is tenuous because terminal vessels from both proximal and distal directions converge poorly here, making it the site most vulnerable to degenerative change and tear initiation.
- Infraspinatus is the primary external rotator of the shoulder, accounting for roughly 60% of total external rotation strength. It is the second most commonly torn tendon and is frequently involved when the supraspinatus tear extends posteriorly.
- Subscapularis is the only anterior muscle of the cuff, serving as the primary internal rotator and a critical stabilizer against anterior humeral head translation. Subscapularis tears were historically under-recognized because they are not seen on standard posterior MRI views and require specific examination and imaging attention.
- Teres minor assists with external rotation and humeral head depression. Isolated teres minor tears are rare.
The four tendons blend together near their insertions on the humeral tuberosities to form a nearly continuous "cuff" of tendinous tissue. A tear in the supraspinatus can propagate in any direction — anteriorly into the subscapularis, posteriorly into the infraspinatus — which is why large and massive tears frequently involve multiple tendons.
4. Types of Tears
Partial versus full-thickness tears
Partial-thickness tears affect only part of the tendon's cross-sectional area. They are further classified by location:
- Articular-surface partial tears (most common) — on the undersurface of the tendon, facing the joint.
- Bursal-surface partial tears — on the upper surface, facing the subacromial bursa.
- Intrasubstance tears — within the body of the tendon, not extending to either surface.
Partial tears are graded by depth: Grade I (<3 mm), Grade II (3–6 mm), Grade III (>6 mm, more than half the tendon thickness). Grade III partial tears behave more like full-thickness tears in terms of symptoms and often require the same surgical decision-making.
Full-thickness tears extend completely through the tendon, creating a defect that allows fluid communication between the glenohumeral joint and the subacromial bursa. They are sized by craniocaudal and anteroposterior dimensions: small (<1 cm), medium (1–3 cm), large (3–5 cm), and massive (>5 cm or involving two or more tendons). Massive tears are frequently accompanied by significant tendon retraction and fatty infiltration of the muscle belly, both of which diminish the likelihood of successful surgical repair.
Traumatic versus degenerative
Traumatic tears occur acutely from a single injury event — a fall, a sudden eccentric load — in a tendon that was previously intact or only minimally degenerate. They tend to occur in younger patients, are often large and symptomatic from onset, and generally respond well to surgical repair because the remaining tendon tissue is healthier and more repairable.
Degenerative tears develop silently over years of repetitive micro-damage in the critical zone. The patient may be unaware of a tear until a relatively minor incident (reaching overhead, a small fall) suddenly worsens preexisting tendon damage enough to produce symptoms. The underlying tendon tissue shows pathologic changes — loss of organized collagen architecture, calcium deposits, failed repair attempts — that make healing more challenging than in traumatic tears.
5. Clinical Presentation and Special Tests
The hallmark presentation of a symptomatic rotator cuff tear is pain with overhead activity, often with an arc of pain between approximately 60 and 120 degrees of abduction (the painful arc), combined with weakness in specific movement patterns that correspond to the torn tendon. Night pain — particularly pain that wakes the patient when rolling onto the affected shoulder — is common and often disproportionately disabling relative to daytime symptoms.
Special physical examination tests by tendon
Several provocation tests help identify which tendon is involved:
- Neer impingement sign. The examiner passively raises the patient's forward-flexed arm while stabilizing the scapula and depressing the shoulder. Pain at approximately 70–90 degrees suggests impingement of the supraspinatus under the acromion. Sensitivity approximately 72%, specificity 66%.
- Hawkins-Kennedy test. The examiner forward-flexes the shoulder to 90 degrees and then passively internally rotates it. Pain reproduces subacromial impingement. Sensitivity approximately 79%, specificity 59%.
- Empty can test (Jobe test) — supraspinatus. The arm is elevated to 90 degrees in the scapular plane with the thumb pointing downward (as though emptying a can). The examiner applies downward force while the patient resists. Pain or weakness is positive for supraspinatus pathology. Sensitivity approximately 69%, specificity 66% for full-thickness tears.
- External rotation resistance — infraspinatus. With the elbow at 90 degrees and the arm at the side, the patient resists the examiner's attempt to internally rotate the forearm. Marked weakness in this position strongly suggests an infraspinatus tear.
- Gerber lift-off test — subscapularis. The patient places the dorsum of their hand against their low back and attempts to push it away from the back against resistance. Inability to do so indicates subscapularis dysfunction. The belly press test (pressing the hand against the abdomen with the elbow forward) is an alternative when the patient cannot internally rotate enough to perform the lift-off.
- Drop arm sign — massive tear. The examiner passively raises the arm to 90 degrees and asks the patient to slowly lower it. Inability to control the descent — the arm drops suddenly — is highly specific for a massive rotator cuff tear or significant deltoid dysfunction.
6. Diagnosis
Clinical examination narrows the differential diagnosis and guides imaging selection, but imaging is required for definitive diagnosis and surgical planning.
Plain radiographs are obtained first. Standard views (AP in internal and external rotation, axillary lateral, outlet view) may reveal superior migration of the humeral head (indicating a massive chronic tear that has allowed the deltoid to pull the humerus upward), acromial morphology (a hooked type III acromion is associated with subacromial impingement), calcific deposits in the tendon, and glenohumeral arthritis.
MRI is the gold standard for rotator cuff tear diagnosis, with sensitivity exceeding 90% for full-thickness tears and approximately 67–77% for partial-thickness tears. MRI identifies tear size, tendon retraction, the number of tendons involved, the degree of fatty infiltration of the muscle belly (Goutallier classification, grades 0–4), and concurrent pathology including labral tears and glenohumeral arthritis. Fatty infiltration of grade III or higher (more fat than muscle) on MRI is a significant predictor of poor functional recovery even after repair.
Ultrasound is an increasingly used, cost-effective alternative that allows dynamic assessment and has good sensitivity for full-thickness supraspinatus tears (approximately 87%) in the hands of an experienced sonographer. It cannot assess the articular surface as completely as MRI and has limitations for infraspinatus and subscapularis assessment. Its advantage is real-time guided injection capability during the same examination visit.
7. Conservative Treatment
Not every rotator cuff tear requires surgery. For partial-thickness tears, small full-thickness tears (<1 cm), and full-thickness tears in patients with low functional demands or significant surgical risk, a well-structured conservative program is the appropriate first approach — and for many patients, it is all that is ultimately needed.
Physical therapy
The cornerstone of conservative management is a structured rehabilitation program targeting:
- Rotator cuff strengthening — progressive resistance exercises for the supraspinatus, infraspinatus, and subscapularis, with emphasis on pain-free range and proper scapular positioning.
- Periscapular stabilization — strengthening the serratus anterior, middle and lower trapezius, and rhomboids to optimize scapular position and reduce subacromial impingement during arm elevation.
- Posterior capsule stretching — tightness of the posterior glenohumeral capsule shifts the humeral head anterosuperiorly during arm elevation, worsening impingement. Cross-body stretching and sleeper stretches address this.
A systematic review by Kukkonen and colleagues (PMID 25784736) found no significant difference in outcomes between conservative treatment and surgical repair for small to medium full-thickness supraspinatus tears in patients over 55 at one year, providing strong support for an initial conservative trial in this population.
Subacromial corticosteroid injection
Subacromial injection of a corticosteroid (typically triamcinolone or methylprednisolone combined with a local anesthetic) provides meaningful short-term pain relief in 60–70% of patients, facilitating participation in rehabilitation. The effect typically lasts 6–12 weeks. Most guidelines recommend limiting injections to three or fewer per year in the same shoulder, as repeated high-dose corticosteroid exposure may impair tendon healing biology.
Biologics: PRP and platelet-rich plasma
Platelet-rich plasma injections have attracted considerable interest as an adjunct to conservative management or as an augmentation to surgical repair, based on the theoretical benefit of delivering growth factors to a poorly vascularized tendon. However, the current evidence is mixed. A meta-analysis by Hurley and colleagues (PMID 31972398) found no consistent benefit of PRP over placebo for chronic rotator cuff tendinopathy. Its role as an augment to surgical repair remains under investigation.
8. Surgical Management
Surgical repair is recommended for:
- Full-thickness symptomatic tears that have failed 3–6 months of structured conservative management.
- Acute traumatic full-thickness tears in active patients under 65, where earlier repair before significant muscle atrophy and fatty infiltration develop improves outcomes.
- Large or massive tears with significant functional deficit.
- Grade III partial-thickness tears with equivalent functional impairment to full-thickness tears.
Arthroscopic rotator cuff repair
Modern rotator cuff surgery is performed almost exclusively arthroscopically, using small portals and suture anchors to reattach the torn tendon edge back to its footprint on the greater (or lesser) tuberosity. Two main fixation techniques are used:
- Single-row repair — one line of anchors placed medially at the articular margin, with sutures passed through the tendon. Simpler, faster, and sufficient for most small to medium tears.
- Double-row repair — a medial row of anchors captures the articular margin and a lateral row restores the broader tendon footprint. Biomechanically superior load distribution; meta-analyses suggest lower re-tear rates for large tears but equivalent functional outcomes for small to medium tears.
Massive and irreparable tears
When a tear is deemed irreparable — due to severe retraction, severe fatty infiltration (Goutallier grade III–IV), or tissue quality too poor for primary repair — several salvage options exist:
- Superior capsule reconstruction (SCR) — a dermal allograft or fascia lata autograft is used to reconstruct the superior capsule, restoring humeral head centering and reducing superior migration. Short- to medium-term outcomes are encouraging in appropriately selected patients.
- Reverse total shoulder arthroplasty (RTSA) — reverses the glenohumeral anatomy so the deltoid, not the rotator cuff, powers elevation. RTSA has revolutionized the treatment of massive irreparable cuff tears with pseudoparalysis (inability to raise the arm against gravity) in patients over 60. It reliably restores meaningful function when the cuff cannot be reconstructed.
- Tendon transfer — in younger patients with irreparable posterior-superior tears and intact subscapularis, lower trapezius or latissimus dorsi transfer can restore external rotation strength.
9. Complications and Outcomes
The most important complication after rotator cuff repair is re-tear. Re-tear rates vary considerably with tear size, patient age, and tissue quality — ranging from approximately 13% for small tears to over 40% for large tears and 60–94% for massive tears. Importantly, many re-tears are not clinically symptomatic; even a structurally failed repair often produces better functional outcomes than the pre-operative state, possibly because the scar tissue provides some mechanical benefit.
A landmark study by Galatz and colleagues (PMID 15284285) found a 94% structural failure rate at two years after repair of massive tears — yet most patients had substantial pain relief and improved function. This dissociation between structural integrity and clinical outcome is a defining feature of rotator cuff biology and a reason why patient-reported outcomes are increasingly emphasized over purely structural endpoints.
Other important considerations include:
- Stiffness (frozen shoulder/adhesive capsulitis) can develop post-operatively, particularly in patients with pre-existing stiffness or those who are under-rehabilitated.
- Infection risk is low (<1%) for arthroscopic procedures.
- Nerve injury — the axillary nerve is at risk during portal placement and anchor insertion; rates are very low in experienced hands.
- Long-term osteoarthritis develops more commonly in shoulders with long-standing massive tears due to altered joint mechanics and superior humeral head migration causing acetabularization of the acromion.
10. References & Research
Key Research Papers
- Search PubMed — 94% re-tear rate at 2 years after massive rotator cuff repair; clinical outcomes improved despite structural failure.
- Search PubMed — RCT: conservative management vs. repair for full-thickness supraspinatus tears; equivalent outcomes at 1 year for patients >55.
- Search PubMed — Meta-analysis of PRP for rotator cuff tendinopathy; no consistent benefit over placebo.
- Search PubMed — RCT comparing early repair with rehabilitation-first strategy; establishes evidence base for conservative-first approach.
- Search PubMed — Natural history of asymptomatic rotator cuff tears; bilateral ultrasound study showing tear progression over time.
- Search PubMed — RCT of surgery vs. physiotherapy for small and medium rotator cuff tears; 5-year outcomes favored surgery for medium tears.
- Search PubMed — Fatty infiltration grading (Goutallier classification) as predictor of rotator cuff repair outcomes.
- Search PubMed — Superior capsule reconstruction for massive irreparable tears; 2-year outcomes and indications.
- Search PubMed — Evidence-based review of subacromial corticosteroid injection; short-term efficacy confirmed, long-term equivalent to conservative care.
- Search PubMed — Single-row vs. double-row repair: meta-analysis showing equivalent clinical outcomes with lower re-tear for large tears with double-row.
- Search PubMed — Reverse total shoulder arthroplasty for massive irreparable rotator cuff tears; long-term functional outcomes.
- Search PubMed — Natural history of asymptomatic full-thickness rotator cuff tears; rate of progression and risk of becoming symptomatic.
Research Papers
The links below run live searches on PubMed, the U.S. National Library of Medicine's database of biomedical literature.
- Rotator cuff repair outcomes
- Conservative rotator cuff treatment
- Supraspinatus tear MRI diagnosis
- Rotator cuff re-tear rates arthroscopic
- Rotator cuff fatty infiltration outcomes
- Superior capsule reconstruction
- Reverse shoulder arthroplasty massive tear
- Subacromial corticosteroid injection
- Rotator cuff PRP treatment
- Rotator cuff rehabilitation physical therapy
- Subscapularis tear diagnosis
- Asymptomatic rotator cuff tear natural history
Connections
- Orthopedics
- ACL Tear — another common soft-tissue tear in active adults; shares principles of conservative vs. surgical decision-making.
- Tendinitis — supraspinatus tendinopathy and rotator cuff impingement exist on a continuum leading to tear.
- Carpal Tunnel Syndrome — another upper-extremity entrapment/mechanical condition affecting the working-age population.
- Osteoarthritis — massive chronic rotator cuff tears cause cuff-tear arthropathy; glenohumeral OA alters treatment planning.
- Stress Fracture — both conditions illustrate how cumulative mechanical loading exceeds tissue repair capacity.
- Hip Fracture — shared osteoporosis/bone-health substrate in older patients; both require multidisciplinary perioperative management.
- All Conditions — complete disease index.