Hip Fracture
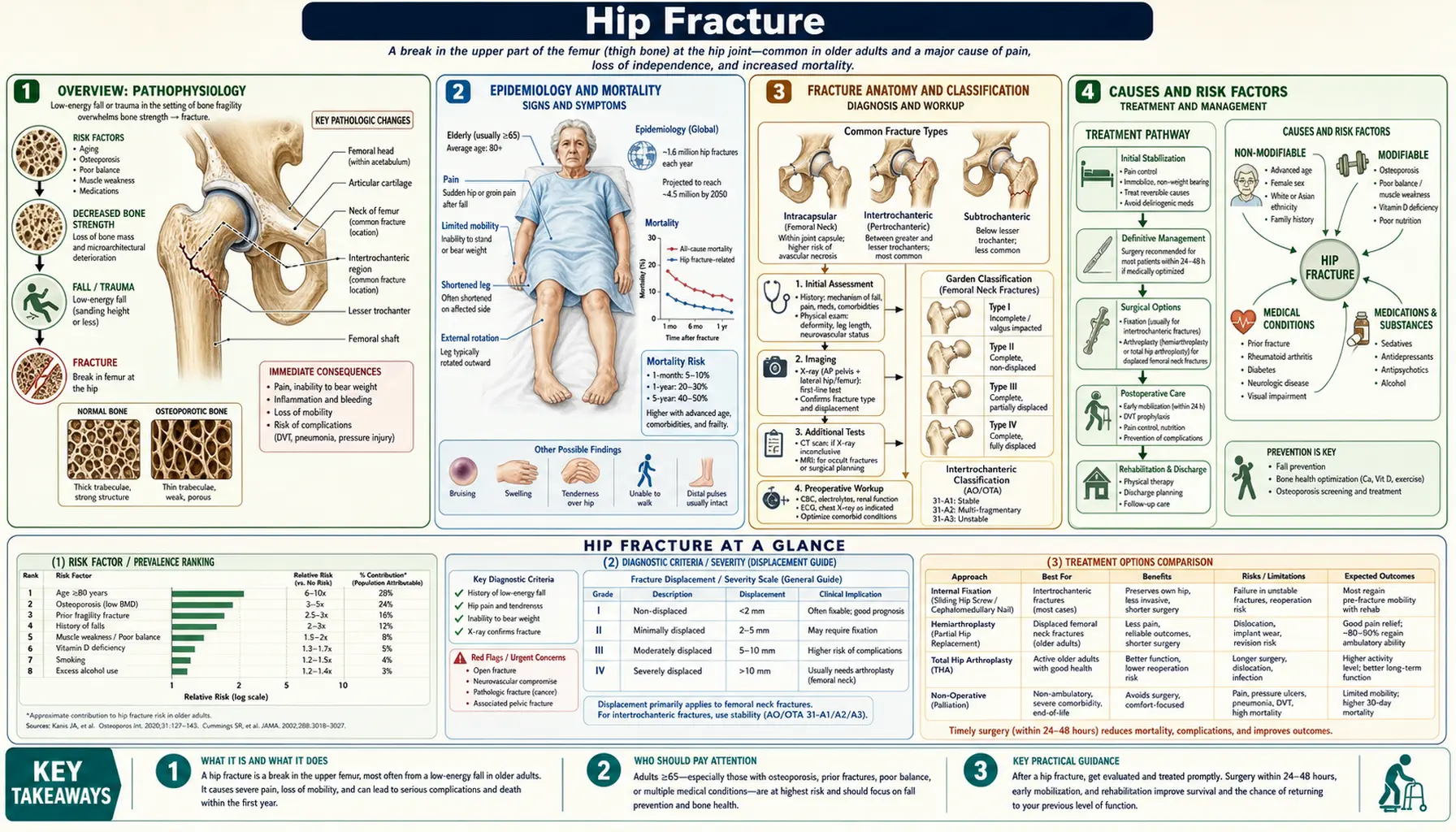
Table of Contents
- Overview
- Epidemiology and Mortality
- Fracture Anatomy and Classification
- Causes and Risk Factors
- Clinical Presentation
- Diagnosis
- Surgical Management
- Perioperative and Medical Care
- Secondary Fracture Prevention
- References & Research
- Research Papers
- Connections
- Featured Videos
1. Overview
A hip fracture is one of the most consequential injuries in older adults — a sentinel event that can permanently change a person's ability to live independently, and which carries a mortality risk that rivals many cancers. In the United States, approximately 300,000 hip fractures occur each year, nearly all in people over 65, and the downstream costs in hospitalization, rehabilitation, and long-term care exceed $6 billion annually. The sobering one-year mortality of 25–30% makes hip fracture a genuine life-threatening emergency, not merely a painful orthopedic inconvenience.
The term "hip fracture" is a clinical shorthand for a fracture of the proximal femur — the uppermost portion of the thigh bone — in the area of the femoral neck or the region around the two bony prominences (trochanters) just below the neck. These two zones differ in crucial ways: their blood supply, their implications for the femoral head, and the surgical strategies required to fix or replace them. Understanding that distinction is the foundation of hip fracture management.
The good news, and it is real: surgical treatment within 24–48 hours of admission, combined with aggressive early mobilization, dramatically reduces mortality and complications compared with delayed or non-operative management. For most patients, the goal is to be walking — even with assistance — within a day or two of surgery. The challenge is getting the whole multidisciplinary machine moving fast enough and coordinated enough to make that happen.
2. Epidemiology and Mortality
Hip fracture epidemiology is dominated by age and osteoporosis. The incidence rises exponentially with age: a woman aged 80–84 is roughly 30 times more likely to sustain a hip fracture than a woman aged 60–64. Women account for approximately 75% of hip fractures in the US, reflecting both their longer lifespan (more exposure to aging) and their substantially higher rates of osteoporosis. White and Asian women have higher fracture rates than Black or Hispanic women, partly because of differences in peak bone mass and body habitus.
The mortality statistics are strikingly high and widely underappreciated by patients and families. Within 30 days of a hip fracture, approximately 8–12% of patients die. By one year, mortality reaches 25–30% in most large cohort studies — a figure that has improved modestly but remains high despite advances in surgical technique and perioperative care. Multiple factors drive this mortality: the patients are old and medically fragile before the fracture; the fracture itself is a physiologic stress (blood loss, pain, immobility, surgery); immobility rapidly worsens existing comorbidities including cardiac disease, renal failure, and thromboembolism; and post-operative delirium, pneumonia, and pressure ulcers add additional mortality burden.
Even survivors face major functional decline: approximately 50% of patients who were independent in walking before their fracture do not recover the ability to walk independently afterward, and 30% are permanently institutionalized.
3. Fracture Anatomy and Classification
The location of a hip fracture relative to the joint capsule is the most clinically important anatomical distinction:
Femoral neck fractures (intracapsular)
The femoral neck is the segment of bone between the spherical femoral head and the wider trochanteric region. It lies almost entirely inside the hip joint capsule. The blood supply to the femoral head is precarious: the primary intraosseous vessels run along the femoral neck (the retinacular vessels, branches of the medial circumflex femoral artery), and a femoral neck fracture can disrupt or destroy these vessels. The result is avascular necrosis (AVN) of the femoral head — the femoral head loses its blood supply and progressively collapses over months to years, causing severe pain and arthritis.
The Garden classification grades femoral neck fractures I–IV by displacement: Grade I–II are non-displaced (valgus impacted or incomplete), and AVN risk is relatively low. Grade III–IV are displaced fractures, with AVN risk of 15–33%, which drives the treatment choice toward arthroplasty rather than internal fixation in elderly patients.
Intertrochanteric fractures (extracapsular)
Intertrochanteric fractures occur in the cancellous (spongy) bone between the greater and lesser trochanters, outside the joint capsule. Because they are extracapsular, the femoral head's blood supply is generally intact and AVN is not a significant concern. These fractures occur in bone that is heavily cancellous and highly vascular, which means they heal reliably with fixation. The trade-off is that they tend to occur in the very oldest, most osteoporotic patients, because the cancellous bone of the trochanteric region is lost earlier in osteoporosis than cortical bone of the femoral neck.
Intertrochanteric fractures are classified as stable (the posteromedial cortex is intact, which provides rotational stability) or unstable (the posteromedial cortex is comminuted or reversed oblique pattern). Stability determines which fixation device is preferred.
Subtrochanteric fractures
Fractures in the 5 cm of femur below the lesser trochanter are classified separately. They are mechanically challenging to fix because of high bending and rotational forces in this region. They are less common than the above two types in osteoporotic patients but can occur in younger patients with high-energy trauma or in older patients on long-term bisphosphonate therapy (atypical femoral fractures).
4. Causes and Risk Factors
The overwhelming majority of hip fractures in older adults result from a low-energy fall from standing height onto an osteoporotic proximal femur. The fracture is ultimately a consequence of two converging processes: the fall event and the underlying bone fragility.
Key risk factors for hip fracture can be grouped into those that affect bone quality and those that affect fall risk:
- Osteoporosis — by far the dominant bone-quality risk factor; BMD below −2.5 T-score at the hip multiplies fracture risk dramatically relative to normal bone density.
- Female sex and postmenopause — estrogen withdrawal accelerates bone loss; hip fracture rates in women are 2–3 times those in men at the same age.
- Prior fragility fracture — any previous low-energy fracture is an independent risk factor for subsequent fracture, including hip fracture, independent of bone density.
- Advanced age — both bone quality and muscle strength decline with age; patients over 80 are at highest absolute risk.
- Low body weight / undernutrition — low BMI is independently associated with hip fracture risk; body fat provides some impact attenuation during falls.
- Fall risk factors: impaired balance and gait (Parkinson's disease, stroke, vestibular disorders), muscle weakness (sarcopenia), polypharmacy (especially sedatives, antihypertensives causing orthostatic hypotension), impaired vision, home hazards.
5. Clinical Presentation
The classic presentation of a displaced hip fracture after a fall is straightforward and almost diagnostic on history and inspection alone:
- Hip or groin pain that is severe enough to prevent weight-bearing.
- Inability to stand or walk — the patient is found on the floor or immediately falls again on attempting to stand.
- Shortened, externally rotated leg — the affected leg appears shorter than the opposite leg and the foot is rotated outward. This is caused by unopposed pull of the iliopsoas and other hip flexors/rotators on the proximal fragment once the fracture disrupts normal bony architecture.
- Pain with any passive motion of the hip, including the log-roll test (external/internal rotation of the extended leg).
Non-displaced or impacted femoral neck fractures (Garden I–II) can present more subtly: the patient may be able to partially weight-bear, groin pain may be mild, and the leg may not appear shortened or rotated. These fractures are commonly missed on initial presentation and must be sought with MRI when plain films are unremarkable and clinical suspicion is present.
The clinician must also assess the cause of the fall, not just the fracture. A hip fracture after a syncopal episode from a cardiac arrhythmia requires ECG monitoring; one after a mechanical trip requires a very different workup. Missed medical triggers (PE, MI, subdural hematoma from the fall) contribute substantially to hip fracture mortality.
6. Diagnosis
Plain radiographs are the first-line imaging study: AP pelvis (both hips in view for comparison) and a lateral view of the affected hip. The vast majority of displaced fractures are visible on these views. The AP pelvis view also provides important information about the contralateral hip (bilateral hip fractures occur in 2–4% of patients) and about pre-existing joint disease that influences arthroplasty planning.
When clinical suspicion is high but plain films are negative or equivocal (the most common scenario for non-displaced femoral neck fractures or impacted valgus fractures), MRI is the gold standard next step. MRI identifies occult fractures, bone marrow edema (bone contusion without complete fracture), and concurrent soft-tissue injuries, with sensitivity approaching 100% and specificity >98%. CT can detect fractures missed on plain film but is less sensitive than MRI for non-displaced injuries and exposes the patient to radiation. If MRI is unavailable, bone scan (scintigraphy) can detect fractures within 72 hours of injury but is slower and less specific.
Pre-operative laboratory workup (CBC, BMP, coagulation studies, type and screen) and ECG are obtained simultaneously with imaging, as the goal is to have the patient in the operating room within 24–48 hours of admission.
7. Surgical Management
Surgery is the definitive treatment for virtually all displaced hip fractures in medically operable patients. The rare exceptions (moribund patients in whom the risks of anesthesia are prohibitive, or patients who were non-ambulatory before the fracture) are managed with non-operative pain management. For everyone else, the evidence is clear: surgery within 24–48 hours reduces mortality, complications, pain, and length of stay compared with delayed surgery beyond 48 hours. Each 24-hour delay is associated with increased in-hospital mortality in observational studies.
Femoral neck fractures
- Non-displaced (Garden I–II) — ORIF with cancellous screws or sliding hip screw. Internal fixation preserves the native femoral head. Healing rates are high and AVN risk is low (<10%) for these non-displaced fractures. Preferred in younger patients regardless of displacement because preserving native bone avoids the need for eventual revision arthroplasty.
- Displaced (Garden III–IV) in elderly patients (>65–70) — arthroplasty. The high AVN risk after ORIF of displaced femoral neck fractures in older adults shifts the balance strongly toward arthroplasty.
- Hemiarthroplasty replaces only the femoral head with a prosthetic component; the native acetabulum is retained. Faster surgery, less blood loss, lower dislocation risk than total hip replacement. Appropriate for lower-demand elderly patients with healthy pre-fracture acetabular cartilage.
- Total hip arthroplasty (THA) replaces both the femoral head and acetabulum. A Cochrane review and subsequent RCTs (HEALTH, HIP-ATTACK) show THA provides better long-term function and lower rates of joint pain/re-operation than hemiarthroplasty in cognitively intact, ambulatory patients with active pre-fracture lifestyles — at the cost of a modestly higher dislocation rate.
Intertrochanteric fractures
- Intramedullary nail (IMN) — a nail inserted down the femoral canal with a lag screw into the femoral head/neck. The IMN is the preferred device for most intertrochanteric fractures, particularly unstable patterns, because it provides better rotational control, allows earlier mobilization, and spans the entire proximal femur to protect against peri-implant fracture.
- Dynamic hip screw (DHS) — a sliding lag screw and plate construct fixed to the lateral femoral shaft. Appropriate for stable intertrochanteric patterns with an intact posteromedial cortex. Less complex to insert than an IMN in simple patterns, but biomechanically inferior for unstable fractures.
8. Perioperative and Medical Care
Hip fracture management is inherently multidisciplinary. The orthopedic surgery is only one component of a care bundle that must address multiple concurrent medical concerns:
Anesthesia
Both general and regional (spinal or epidural) anesthesia are used. A large RCT (REGAIN trial, PMID 32359177) found no significant difference in 60-day mortality or delirium between spinal and general anesthesia, though spinal anesthesia is associated with lower rates of intra-operative hypotension and slightly faster post-anesthesia recovery in observational studies.
VTE prophylaxis
Hip fracture patients are at very high risk for deep vein thrombosis and pulmonary embolism. Pharmacologic prophylaxis (low-molecular-weight heparin, fondaparinux, or a direct oral anticoagulant) should be started as soon as feasible after surgery and continued for 28–35 days. Mechanical prophylaxis (pneumatic compression devices) is used pre-operatively and for patients in whom anticoagulation is contraindicated.
Post-operative delirium
Post-operative delirium occurs in 35–65% of hip fracture patients and is an independent predictor of prolonged hospitalization, institutionalization, cognitive decline, and mortality. Prevention strategies include early mobilization, adequate pain control (reducing opioid burden with multimodal analgesia), avoiding anticholinergic and sedating medications, minimizing urinary catheterization duration, ensuring adequate hydration and nutrition, and providing orienting cues. A dedicated geriatric co-management service (orthogeriatric co-management) reduces delirium incidence, length of stay, and complications in RCT evidence.
Early mobilization
Physical therapy should begin on post-operative day one whenever possible. The goal is weight-bearing ambulation with assistance within 24 hours of surgery. Early mobilization reduces pneumonia, pressure ulcers, VTE, muscle atrophy, and delirium. It is a non-negotiable component of hip fracture care rather than a nice-to-have.
9. Secondary Fracture Prevention
A hip fracture is both a consequence and a warning signal of severe underlying bone fragility. Without intervention, the risk of a second hip fracture or other fragility fracture within 5 years is 5–10 times higher than in the general age-matched population. Yet rates of post-hip-fracture osteoporosis treatment remain dismally low — fewer than 20% of patients discharged after a hip fracture receive appropriate bone-protective therapy in most systems.
Every hip fracture patient who survives to discharge should have:
- DXA bone density measurement (if not performed recently).
- FRAX fracture risk assessment using clinical risk factors ± BMD.
- Calcium and vitamin D supplementation (1200 mg calcium daily from diet + supplement; vitamin D3 800–2000 IU daily).
- Pharmacologic bone protection in appropriate candidates:
- Bisphosphonates (alendronate, zoledronic acid) — first-line; zoledronic acid once yearly IV is particularly convenient and has Level 1 evidence for reducing mortality after hip fracture (PMID 17474134).
- Denosumab — preferred when renal function is impaired (GFR <35 mL/min) or bisphosphonates are not tolerated.
- Teriparatide/abaloparatide (anabolic agents) — for patients with very low BMD or prior bisphosphonate failure; stimulate new bone formation rather than merely preventing resorption.
- Fall prevention program: exercise (balance and strength training), vision assessment, medication review (deprescribing sedatives, antihypertensives if clinically feasible), home safety assessment, and hip protector pads for high-risk patients.
10. References & Research
Key Research Papers
- Search PubMed — HORIZON-RFT: zoledronic acid after hip fracture reduced new clinical fractures by 35% and all-cause mortality by 28%.
- REGAIN trial, 2020 — PMID: 32359177 — Spinal vs. general anesthesia for hip fracture surgery: no significant difference in 60-day mortality or delirium.
- Search PubMed — THA vs. hemiarthroplasty for displaced femoral neck fractures; THA showed better functional outcomes, lower re-operation rates at 24 months in active patients.
- Search PubMed — Meta-analysis: hip fracture surgery delay >48 hours associated with increased 30-day and 1-year mortality.
- Search PubMed — Intramedullary nail vs. sliding hip screw for intertrochanteric fractures: systematic review showing IMN advantage for unstable patterns.
- Search PubMed — Orthogeriatric co-management model: systematic review showing reduced length of stay, mortality, and complication rates.
- Search PubMed — Occult hip fractures: MRI as gold standard compared with CT and bone scan.
- Search PubMed — 1-year mortality after hip fracture: population-based study showing 30% mortality, driven largely by comorbidities.
- Search PubMed — USPSTF: interventions to prevent falls in community-dwelling older adults; graded exercise and multifactorial programs.
- Search PubMed — Post-hip-fracture treatment gap: systematic review showing <25% of patients received bone-protective therapy after hip fracture.
- Search PubMed — Denosumab vs. placebo in post-menopausal osteoporosis; hip fracture risk reduction 40%.
- Search PubMed — FRAX tool validation for hip fracture prediction; integration with BMD in clinical risk stratification.
Research Papers
The links below run live searches on PubMed, the U.S. National Library of Medicine's database of biomedical literature.
- Hip fracture mortality outcomes
- Hip fracture surgical timing delay
- Femoral neck fracture arthroplasty vs ORIF
- Intertrochanteric fracture intramedullary nail
- Hip fracture osteoporosis bisphosphonate
- Hip fracture delirium prevention
- Hip fracture early mobilization rehabilitation
- Hip fracture VTE prophylaxis
- Occult hip fracture MRI diagnosis
- Hip fracture secondary prevention
- Orthogeriatric co-management
- Hip fracture epidemiology USA
Connections
- Orthopedics
- Stress Fracture — both conditions result from bone failing under load; shared osteoporosis substrate in older women.
- Rotator Cuff Tear — another major surgical orthopedic condition in older adults; shared perioperative care principles.
- Osteoporosis — primary underlying cause of hip fracture; bisphosphonate/denosumab treatment addresses the root cause.
- Osteoarthritis — pre-existing hip OA alters arthroplasty planning; both conditions are common co-morbidities in older adults.
- Carpal Tunnel Syndrome — another common orthopedic condition in older adults; shared fall-risk context (wrist fractures are the most common fall-related fracture).
- Calcium — adequate calcium intake is a cornerstone of hip fracture prevention and post-fracture bone-building.
- Vitamin D3 — vitamin D3 supplementation reduces falls and hip fracture risk; co-prescribed with all bone-protective agents.
- All Conditions — complete disease index.