POEMS Syndrome
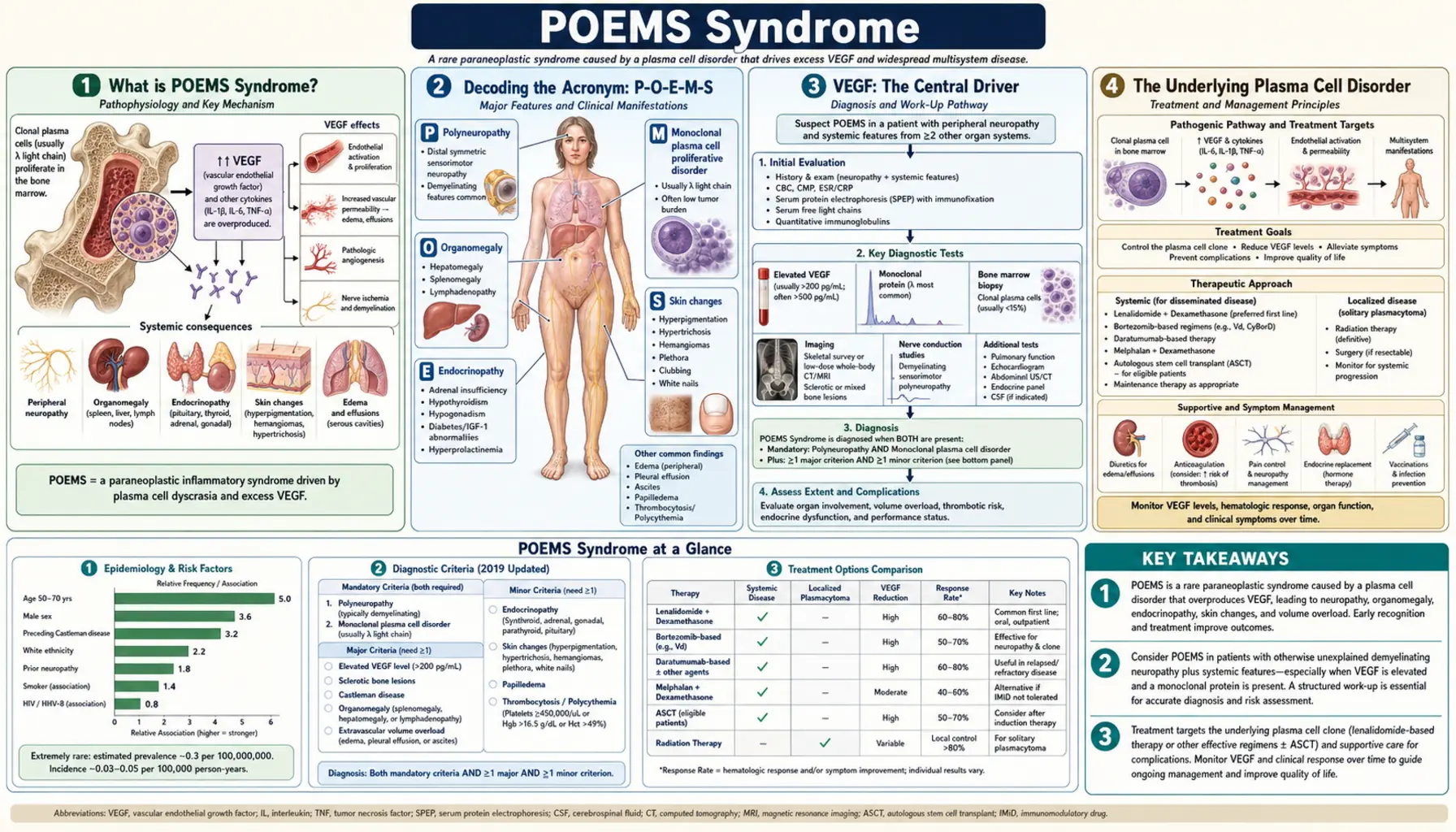
Table of Contents
- What is POEMS Syndrome?
- Decoding the Acronym: P-O-E-M-S
- VEGF: The Central Driver
- The Underlying Plasma Cell Disorder
- Polyneuropathy: The Defining Feature
- Endocrine and Skin Manifestations
- Other Clinical Features: Sclerotic Bone Lesions, Edema, Papilledema
- Diagnosis: Mayo Clinic Criteria
- Treatment Approaches
- Prognosis and Monitoring
- Key Research Papers
- Connections
- Featured Videos
What is POEMS Syndrome?
POEMS syndrome is one of medicine's rarest and most complex disorders — a paraneoplastic syndrome driven by an underlying plasma cell clone that secretes a pathological monoclonal antibody. The term "paraneoplastic" means that the disease manifestations are not caused directly by tumor invasion or mass, but by substances produced by the tumor cells affecting distant organs. In POEMS, the key pathological substance is VEGF (vascular endothelial growth factor), which is produced in vastly excessive amounts by the abnormal plasma cells and drives nearly all of the multi-organ disease. POEMS is estimated to affect approximately 0.3 per million people per year — making it rarer than multiple myeloma and far rarer than the more common plasma cell disorders. It predominantly affects middle-aged adults, with a median age at diagnosis in the 50s; it is slightly more common in men. Because POEMS is rare and its manifestations span many organ systems, patients often see multiple specialists over years before a correct diagnosis is made. The disease is serious but potentially treatable — early diagnosis can prevent irreversible organ damage, particularly to the peripheral nervous system.
Decoding the Acronym: P-O-E-M-S
The acronym POEMS was coined by Bardwick and colleagues in 1980 to capture the most recognizable clinical features of the syndrome. P stands for Polyneuropathy — a severe, progressive nerve disorder affecting the limbs, which is present in virtually every patient and is mandatory for diagnosis. O stands for Organomegaly — enlargement of the liver, spleen, or lymph nodes, found in approximately 40–50% of patients. E stands for Endocrinopathy — hormonal abnormalities affecting multiple glands, found in up to 80% of patients; the most common is hypogonadism (low sex hormones). M stands for Monoclonal protein — a single abnormal immunoglobulin produced by the clonal plasma cells; in POEMS, this is almost always an IgG or IgA with a lambda (λ) light chain, a highly specific finding. S stands for Skin changes — a variety of dermatological abnormalities including hyperpigmentation, hypertrichosis (excess hair growth), skin thickening, hemangiomata (small vascular growths), and white nails. However, the acronym is incomplete — several other features not in the acronym are equally important and commonly present, including sclerotic bone lesions, massive edema, papilledema, and elevated VEGF.
VEGF: The Central Driver
Vascular endothelial growth factor (VEGF) is the master mediator in POEMS syndrome. Serum VEGF levels in POEMS patients are typically dramatically elevated — often 10- to 100-fold above normal, frequently exceeding 1,000 pg/mL (normal less than 80–100 pg/mL). VEGF is a potent angiogenic (blood vessel-forming) and vascular permeability factor. Under normal conditions, it regulates wound healing and tissue oxygenation. In POEMS, the plasma cell clone appears to be an aberrantly high producer of VEGF, flooding the circulation with it. The consequences of massively elevated VEGF are far-reaching: markedly increased vascular permeability causes capillary leak — fluid leaks from blood vessels into tissues, producing the characteristic peripheral edema, ascites, and pleural effusions seen in POEMS. Elevated VEGF directly damages the blood-nerve barrier, contributing to polyneuropathy. It promotes new blood vessel growth in inappropriate locations. It causes papilledema by increasing permeability of cerebral blood vessels, leading to elevated intracranial pressure. VEGF also mediates the endocrine dysfunction, possibly through effects on pituitary and hypothalamic vasculature. The clinical importance of VEGF in POEMS cannot be overstated: serum VEGF level is the single most useful biomarker for diagnosis, monitoring treatment response, and detecting relapse. When POEMS treatment is effective, VEGF levels fall dramatically, often before clinical improvement.
The Underlying Plasma Cell Disorder
POEMS syndrome is driven by a clonal proliferation of plasma cells — the same type of cell responsible for multiple myeloma and monoclonal gammopathy of undetermined significance (MGUS). However, the plasma cell biology of POEMS is distinct from typical myeloma in several important ways. The monoclonal protein in POEMS is almost always lambda light chain (>95% of cases), whereas myeloma has roughly equal kappa/lambda distribution. The M-protein level in POEMS is often surprisingly low — frequently below the threshold that would trigger a myeloma diagnosis, sometimes even below the MGUS threshold. This counterintuitive feature — serious multi-organ disease driven by a small plasma cell clone — is explained by the extraordinary VEGF output of each individual plasma cell. The underlying bone lesion in POEMS is characteristically osteosclerotic (bone-hardening, producing dense bony plaques) rather than the lytic (bone-dissolving) lesions of multiple myeloma. POEMS-associated plasma cells form localized sclerotic bone lesions, often in the axial skeleton, pelvis, and proximal long bones. In a variant of POEMS, the disease is associated with Castleman disease — a rare lymph node disorder (especially multicentric Castleman disease of the HHV-8-negative type) — which adds to the lymphadenopathy and systemic inflammation.
Polyneuropathy: The Defining Feature
Polyneuropathy is the most prominent and disabling manifestation of POEMS syndrome and the one that most often brings patients to medical attention. Unlike the relatively mild, predominantly sensory neuropathy of MGUS, POEMS neuropathy is severe, progressive, and affects both sensory and motor functions. It is an ascending, symmetric neuropathy — starting in the feet and hands and progressing proximally over months to years. On nerve conduction studies and electromyography (EMG), it shows a mixed pattern: both demyelinating (slowed conduction, indicating damage to myelin sheath) and axonal (reduced amplitude, indicating nerve fiber loss) features. This combination distinguishes it from purely demyelinating neuropathies like CIDP. Clinically, patients experience severe numbness and tingling, but also profound motor weakness — difficulty walking, climbing stairs, rising from chairs — which can progress to the need for a cane, walker, or wheelchair. Pain may be significant. The neuropathy in POEMS is thought to be driven by VEGF-mediated damage to the blood-nerve barrier, combined with direct immunological damage from the monoclonal lambda protein. Treatment response in the neuropathy often lags behind VEGF normalization by 6–12 months; patients should understand that nerve healing is slow even when treatment is working. Maximum neuropathy response typically occurs 1–3 years after effective treatment.
Endocrine and Skin Manifestations
Endocrine abnormalities occur in up to 80% of POEMS patients and often involve multiple glands simultaneously — a pattern unusual in other diseases. Hypogonadism is the most common endocrine manifestation: low testosterone in men (causing decreased libido, erectile dysfunction, infertility, fatigue) and menstrual irregularities in women. Hypothyroidism (low thyroid function) is common and may be the presenting endocrine complaint. Adrenal insufficiency (low cortisol production) is found in a subset of patients and can cause profound fatigue, hypotension, and salt craving. Diabetes mellitus or impaired glucose tolerance occurs in 10–20% of patients. Hyperprolactinemia may cause galactorrhea in women. Multiple simultaneous endocrine deficiencies — affecting pituitary, thyroid, adrenal, and gonadal axes at once — is a characteristic finding that raises suspicion for POEMS. The mechanism is thought to involve VEGF-mediated vascular damage to endocrine glands, combined with immune-mediated effects. Skin changes in POEMS are numerous and clinically recognizable: hyperpigmentation (darkening of the skin, particularly sun-exposed areas) is common; hypertrichosis (excessive hair growth on face, limbs, or trunk) occurs in a minority; skin thickening and a scleroderma-like texture; cutaneous hemangiomata (small cherry-red vascular lesions on the skin surface); and white nails (leukonychia). The simultaneous presence of multiple unusual skin findings should prompt consideration of POEMS.
Other Clinical Features: Sclerotic Bone Lesions, Edema, Papilledema
Several features not captured in the POEMS acronym are important and clinically distinctive. Sclerotic bone lesions (osteosclerotic myeloma) are the characteristic bone finding in POEMS. Unlike the punched-out lytic lesions of multiple myeloma, POEMS lesions appear as dense, sclerotic (bone-hardening) plaques on plain radiography, CT, or PET-CT. They may be solitary or multiple, and are typically found in the vertebral bodies, pelvis, ribs, and proximal femur. A single sclerotic plasmacytoma (solitary bone lesion) may be the only evidence of plasma cell disease in POEMS and, when treated with radiation, may produce complete resolution of the syndrome. Edema and effusions are ubiquitous in POEMS, reflecting VEGF-driven capillary leak. Peripheral edema (ankle and leg swelling) is present in up to 80% of patients. Ascites (abdominal fluid accumulation), pleural effusions (fluid around the lungs), and pericardial effusions (fluid around the heart) occur in varying combinations. The fluid accumulation can be massive and may require periodic drainage. Papilledema — swelling of the optic disc from elevated intracranial pressure — is found in 25–35% of patients on fundoscopic examination. It can cause visual symptoms (blurred vision, visual field loss) and, if untreated, permanent visual loss. Thrombocytosis (elevated platelet count) and erythrocytosis (elevated red blood cell count) are paradoxical findings in POEMS, in contrast to the cytopenias of typical myeloma.
Diagnosis: Mayo Clinic Criteria
Diagnosing POEMS requires meeting specific criteria because no single test is pathognomonic and the disease mimics many other conditions. The Mayo Clinic diagnostic criteria (2019 revision) require: TWO mandatory major criteria (polyneuropathy AND monoclonal lambda plasma cell disorder) PLUS at least ONE of three other major criteria (osteosclerotic bone lesion, Castleman disease variant, or elevated VEGF levels ≥3× upper limit of normal) PLUS at least ONE of six minor criteria (organomegaly, volume overload/edema/effusions, endocrinopathy, skin changes, papilledema, or thrombocytosis/erythrocytosis). Mandatory diagnostic workup includes: nerve conduction studies/EMG to characterize neuropathy; serum and urine protein electrophoresis with immunofixation (specifically looking for lambda monoclonal protein); serum free light chains; bone marrow biopsy with immunohistochemistry; whole-body CT scan or PET-CT to identify sclerotic bone lesions (which can be subtle); serum VEGF level (the single most important biomarker — dramatically elevated in POEMS); endocrine panel (testosterone/estrogen, TSH, morning cortisol, prolactin, glucose); ophthalmological exam for papilledema; CBC (often shows thrombocytosis). VEGF is crucial: if VEGF is not significantly elevated, the diagnosis of POEMS should be questioned. Note that serum VEGF measured in EDTA plasma is the preferred specimen; serum measurements may be artifactually high due to platelet VEGF release during clotting.
Treatment Approaches
POEMS syndrome is a serious but treatable disease. Unlike many paraneoplastic syndromes, effective treatment of the underlying plasma cell disorder can produce profound improvement or even complete reversal of the POEMS manifestations — including partial or complete recovery of neuropathy in many patients. For localized disease (single or few isolated osteosclerotic lesions, limited marrow involvement), radiation therapy to the sclerotic bone lesion(s) is the treatment of choice and can produce long-term remission or cure in carefully selected patients. After radiation, VEGF levels often normalize and neuropathy improves over 1–3 years. For disseminated or widespread disease, systemic therapy is required. Autologous stem cell transplantation (ASCT) preceded by high-dose melphalan conditioning is the most effective treatment for eligible patients (typically younger, fit patients without severe neuropathy). ASCT produces deep and durable responses with significant rates of complete resolution of POEMS manifestations; it is considered the standard of care for transplant-eligible patients. Bortezomib-based regimens (bortezomib/dexamethasone/cyclophosphamide or bortezomib/melphalan/dexamethasone) are effective for transplant-ineligible patients or as induction before ASCT; bortezomib has activity against plasma cells and has favorable effects on neuropathy compared to thalidomide. Lenalidomide with dexamethasone is an effective and tolerable regimen; thalidomide-dexamethasone has been used historically but thalidomide itself can worsen neuropathy. Bevacizumab (an anti-VEGF antibody) has been studied but results are mixed; it is not a standard treatment but may be considered in selected patients. All patients with POEMS require comprehensive supportive care: physical and occupational therapy for neuropathy rehabilitation, endocrine replacement (testosterone, thyroid hormone, hydrocortisone as needed), management of edema and effusions, anticoagulation for thrombotic risk.
Prognosis and Monitoring
POEMS syndrome is a serious chronic disease, but outcomes have improved substantially with modern treatment. In published series, median overall survival for POEMS has ranged from 5 to 14 years, with the best outcomes in patients who achieve complete hematological remission (undetectable monoclonal protein). Patients who undergo ASCT and achieve a complete hematological response have 10-year survival rates exceeding 70% in some series — approaching the prognosis of indolent myeloma. Factors associated with worse prognosis include severe baseline neuropathy (especially with motor involvement and wheelchair dependence), respiratory compromise (impaired diaphragm function from neuropathy — a rare but dangerous complication), advanced age, and significant organ dysfunction at diagnosis. Early diagnosis before irreversible nerve damage has occurred offers the best chance for meaningful neuropathy recovery. VEGF level is the primary monitoring biomarker: it falls rapidly with effective treatment (often within weeks to months) and rises with relapse, often before clinical deterioration. Serial VEGF measurements every 3–6 months are standard. Serum free light chains and M-protein level also track treatment response. Nerve conduction studies track neurological improvement, though changes are slow. Patients should be monitored by a multidisciplinary team including hematology/oncology, neurology, endocrinology, and physical medicine and rehabilitation.
Key Research Papers
- Dispenzieri A, et al. (2007). POEMS syndrome: definitions and long-term outcome. Blood. — Search PubMed
- Dispenzieri A. (2016). POEMS syndrome: 2017 update on diagnosis, risk stratification, and management. Am J Hematol. — Search PubMed
- Kuwabara S, et al. (2001). Elevated plasma vascular endothelial growth factor is diagnostic for POEMS syndrome. J Neurol Neurosurg Psychiatry. — Search PubMed
- Kourelis TV, et al. (2016). Autologous stem cell transplantation for POEMS syndrome. Leukemia. PMID 22517908
- D'Souza A, et al. (2012). Effect of lenalidomide therapy on the function of regulatory T-cells and plasmacytes in patients with POEMS syndrome. Leukemia. — Search PubMed
- Royer B, et al. (2013). Bortezomib, cyclophosphamide, and dexamethasone for POEMS syndrome. Leuk Lymphoma. — Search PubMed
- Dispenzieri A, et al. (2009). Treatment of newly diagnosed POEMS syndrome with transplantation and bortezomib-based therapy. Br J Haematol. — Search PubMed
- Li J, et al. (2013). Newly diagnosed POEMS syndrome with high serum vascular endothelial growth factor. Ann Hematol. — Search PubMed
- Nasu S, et al. (2012). Endocrine manifestations of POEMS syndrome. QJM. — Search PubMed
- Karam C, et al. (2012). Neuropathy in POEMS syndrome: a clinical, electrophysiological, and histopathological analysis. Ann Neurol. — Search PubMed
- Keddie S, et al. (2018). POEMS syndrome — diagnosis and treatment. Pract Neurol. — Search PubMed
- Zagouri F, et al. (2017). Lenalidomide in patients with POEMS syndrome: a systematic review and pooled analysis. Leuk Lymphoma. — Search PubMed
Connections
- Oncology
- Multiple Myeloma
- Peripheral Neuropathy
- Waldenström's Macroglobulinemia
- Aplastic Anemia
- Myelodysplastic Syndrome
- Hypothyroidism
- Non-Hodgkin Lymphoma
- Anemia