Chronic Fatigue Syndrome (ME/CFS): History and Discovery
The history of myalgic encephalomyelitis / chronic fatigue syndrome (ME/CFS) is, more than almost any other illness, a history of names — and of the people behind them being believed or disbelieved. The same profound, exertion-worsened exhaustion has been called neurasthenia, benign myalgic encephalomyelitis, epidemic neuromyasthenia, chronic fatigue syndrome, and systemic exertion intolerance disease, and each label carried a verdict about whether sufferers were truly sick. This page traces that contested story honestly: from a nineteenth-century diagnosis of “tired nerves,” through the post-viral hospital outbreaks of the mid-twentieth century, to the trivialising 1988 coinage of “chronic fatigue syndrome,” the controversy over exercise therapy, and the modern recognition — affirmed by the 2015 U.S. Institute of Medicine report — that this is a serious, biological, multi-system disease. Where a claim about who named what, and when, is genuinely uncertain or disputed, it is flagged rather than smoothed over.
Table of Contents
- Neurasthenia and the Nineteenth-Century “Tired Nerves”
- The Twentieth-Century Outbreaks
- The 1955 Royal Free Hospital Outbreak
- Naming Myalgic Encephalomyelitis (1956) and Ramsay's Work
- Lake Tahoe and the 1988 CDC Coinage of “CFS”
- The Psychological-versus-Biological Battle
- The PACE Trial, Graded Exercise, and Post-Exertional Malaise
- The 2015 Institute of Medicine Report and SEID
- The Dismissal of Patients — An Honest Reckoning
- Research Papers and References
- Connections
- Featured Videos
Neurasthenia and the Nineteenth-Century “Tired Nerves”
Long before anyone spoke of ME or CFS, Western medicine had a fashionable diagnosis for unexplained, disabling exhaustion: neurasthenia, literally “weakness of the nerves.” The American neurologist George Miller Beard (1839–1883) is the name most associated with it; in an 1869 paper in the Boston Medical and Surgical Journal (the forerunner of the New England Journal of Medicine) he described neurasthenia as a condition of fatigue, headache, neuralgia, palpitations, and low mood, which he attributed to the nervous system running out of energy under the strain of modern civilisation. He went on to make it one of the best-known diagnoses of his era.
It is important to be precise here, because the history is often told loosely. Beard did not actually invent the word “neurasthenia” — the term had been used for a mechanical weakness of the nerves decades earlier (sources trace it to around 1829), and in the very same year of 1869 the Michigan asylum physician E. H. Van Deusen independently published on neurasthenia as a psychiatric concept. What Beard did was popularise and redefine it as a modern illness of overworked, urban life. The distinction matters: saying Beard “coined” the term overstates the record, whereas saying he launched it into a century of worldwide use is accurate. Neurasthenia became so identified with the United States that it acquired the nickname “Americanitis.”
Whether nineteenth-century neurasthenia was the “same” illness as today's ME/CFS is genuinely unknowable and should not be asserted; it was an enormous, elastic category that almost certainly swept together depression, anxiety, post-infectious fatigue, and much else. But the recurring suspicion that such patients were merely weak or “nervous” runs unbroken from Beard's clinic to the modern controversy. The label changed; the problem of being a chronically exhausted patient whom medicine could not explain did not.
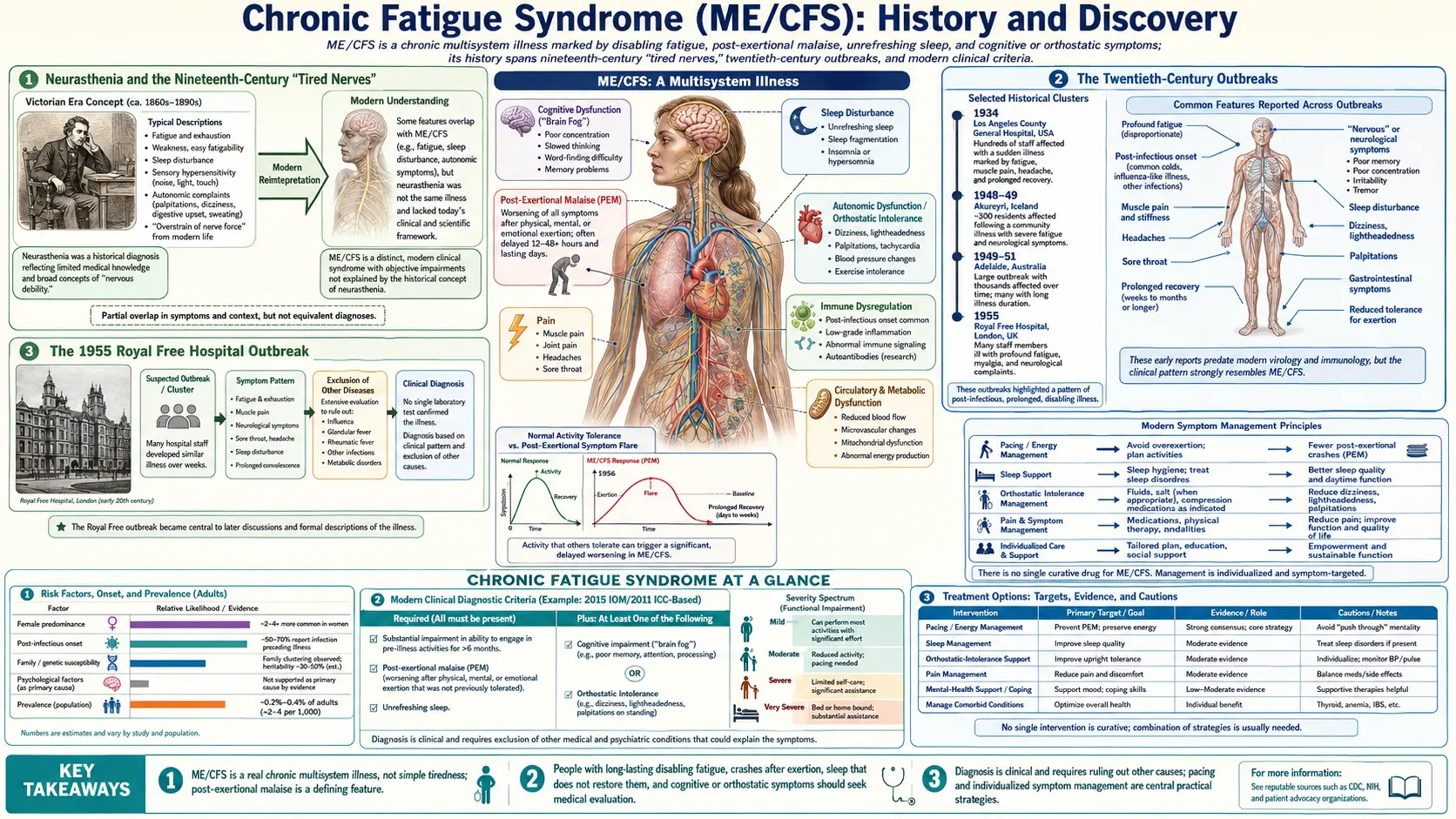
The Twentieth-Century Outbreaks
The modern story of ME/CFS turns on a striking twentieth-century phenomenon: cluster outbreaks of a fatiguing, often post-infectious illness, frequently striking groups of people in a single institution or town. Because these outbreaks affected many people at once, in a pattern resembling an infection, they were far harder to dismiss as individual nervousness — and they pushed clinicians to treat the illness as a real, possibly viral, neurological disease.
Several such episodes were documented across the mid-century. The 1934 outbreak among staff at the Los Angeles County General Hospital, during a polio epidemic, produced a lingering fatiguing illness in those affected. In 1948–1949 an outbreak in Akureyri, Iceland (sometimes called “Akureyri disease” or “Iceland disease”) affected over a thousand people with persistent muscle pain and exhaustion. Further clusters were later grouped by researchers under the umbrella term “epidemic neuromyasthenia.” These names — Iceland disease, epidemic neuromyasthenia, and later benign myalgic encephalomyelitis — were eventually treated as descriptions of one broad clinical syndrome.
What these outbreaks shared was a pattern that still defines the illness: a triggering infection, followed not by recovery but by months or years of disabling fatigue, muscle pain, cognitive difficulty, and a characteristic worsening after exertion. They are the empirical backbone of the argument that ME/CFS is a genuine post-viral, organic disease rather than a psychological state — and the most famous of them, at the Royal Free Hospital in London, gave the illness the name many patients still prefer.
The 1955 Royal Free Hospital Outbreak
In 1955, between July and November, a dramatic outbreak struck the staff of the Royal Free Hospital in London. Roughly 292 members of staff — doctors, nurses, and ancillary workers — fell ill, and about 255 were admitted to the hospital; the outbreak was severe enough that the hospital had to be closed to admissions for a period. Strikingly, it affected hospital staff far more than patients, and women more than men, a demographic pattern that has echoed through the illness's history ever since.
The Royal Free patients presented with a confusing mix of malaise, low-grade fever, headache, neck stiffness, muscle pain and weakness, and a range of neurological signs, followed in many by a long, relapsing course of exhaustion and emotional lability. No infectious agent was ever conclusively identified despite extensive investigation, which left the outbreak open to competing interpretations from the start. That ambiguity — a real, sometimes severe illness with no proven pathogen and no abnormal routine tests — set the template for decades of argument about whether ME/CFS is organic or psychological.
The interpretation of the Royal Free outbreak has itself become contested ground. A widely cited 1970 reappraisal by two psychiatrists, McEvedy and Beard (no relation to George Beard, despite the surname), controversially argued the outbreak was best explained as epidemic hysteria — a conclusion many clinicians and patients have since rejected as unsupported. Later analyses, including a 2020 paper modelling the epidemic as a transmissible infectious disease, push back in the opposite direction. The episode remains a genuine historical dispute, and is presented here as one rather than resolved in either camp.
Naming Myalgic Encephalomyelitis (1956) and Ramsay's Work
The name “myalgic encephalomyelitis” entered the medical literature in 1956, in an editorial in The Lancet prompted by the Royal Free and related outbreaks. The term joins myalgic (muscle pain) with encephalomyelitis (inflammation of the brain and spinal cord), reflecting the authors' belief that the illness was a real inflammatory disease of the nervous system. The editorial is widely attributed to Dr. (later Sir) Donald Acheson, who published it as an anonymous leading article — the standard form for Lancet editorials of the day — and who proposed the title “benign myalgic encephalomyelitis.” Acheson chose “benign” only because, unlike polio or other encephalitides, the outbreaks had not been fatal; the qualifier was later dropped because, for severely affected patients, the illness was anything but benign. Acheson went on to a distinguished career and later served as England's Chief Medical Officer.
The physician most identified with characterising ME clinically is Dr. A. Melvin Ramsay, an infectious-disease consultant at the Royal Free who investigated the 1955 outbreak and spent the rest of his career studying and advocating for the illness. Ramsay described the cardinal features that still anchor the ME concept — especially muscle fatigability, in which even minor exertion is followed by a prolonged, disproportionate loss of strength and a delayed recovery. This emphasis on exertion making patients worse is, in retrospect, an early clinical recognition of what is now called post-exertional malaise, and it is the feature that most clearly distinguishes ME/CFS from ordinary tiredness or deconditioning.
Ramsay's later diagnostic criteria (often called the Ramsay definition) and his insistence that ME was a distinct, organic, post-infectious disease made him a foundational figure for the patient community, and the name he championed — ME — remains the one many patients and advocacy organisations prefer to this day. The 1956 naming and Ramsay's clinical work together established ME as a recognised entity in British medicine well before the American “chronic fatigue syndrome” label appeared three decades later.
Lake Tahoe and the 1988 CDC Coinage of “CFS”
The American chapter of the story opens in the mid-1980s. In the winter of 1984 and through 1985, the resort communities of Incline Village and the Lake Tahoe / Truckee area of Nevada and California saw an outbreak of a persistent, flu-like, exhausting illness. Two local physicians, Daniel Peterson and Paul Cheney, documented scores of patients with severe fatigue, cognitive problems (“brain fog”), and prolonged disability, and called in the U.S. Centers for Disease Control and Prevention (CDC) to investigate. Because many patients showed elevated antibodies to the Epstein–Barr virus, the illness was at first widely discussed as “chronic Epstein–Barr virus” or “chronic mononucleosis.”
The CDC's investigators were unconvinced that Epstein–Barr virus was the cause, since not every patient had the same serology and the antibody findings were hard to interpret. In 1988, a CDC-led working group headed by Gary Holmes (with Jon Kaplan and colleagues) published a consensus case definition that gave the illness a deliberately neutral, symptom-based name: “chronic fatigue syndrome.” The stated logic was to avoid implying an unproven viral cause — but in choosing to foreground the single word “fatigue,” the CDC attached to a serious neuro-immune illness a name that sounded, to many patients and clinicians, like ordinary tiredness.
The consequences of that 1988 choice were enormous and are widely regarded as harmful. Patients felt the name trivialised their condition — reducing a disease that could leave people bedbound to a complaint of being “chronically tired” — and that it invited disbelief from doctors, employers, insurers, and family. The broad Holmes criteria also shaped a generation of research toward a heterogeneous “fatigue” population rather than the more specifically defined ME described in Britain. The mismatch between the British “ME” tradition and the American “CFS” label is the direct origin of the awkward combined term “ME/CFS” used today.
The Psychological-versus-Biological Battle
For much of the late twentieth century, the central conflict over ME/CFS was framed as a war between two explanations: was this a biological disease — post-viral, immunological, neurological — or a psychological / behavioural condition driven by mood, false illness beliefs, and physical deconditioning? The answer was never merely academic. It determined whether patients were offered medical investigation and accommodation, or told their problem was essentially in their minds and that they could think and exercise their way out of it.
An influential school of thought, especially among some British psychiatrists from the 1980s onward, advanced a “biopsychosocial” model. In its strongest form it proposed that whatever infection had originally triggered the illness, the ongoing disability was perpetuated by deconditioning and by patients' fear of activity — implying that the cure was to correct those beliefs (with cognitive behavioural therapy) and to rebuild fitness (with graded exercise therapy). To patients who experienced unmistakable physical crashes after exertion, this felt both wrong and insulting, and the resulting breakdown of trust between patients and parts of the medical establishment is one of the defining features of the illness's history.
Over the following decades the evidence shifted decisively toward the biological. Research has documented abnormalities in immune function, energy metabolism, autonomic regulation, and the response to exertion, and authoritative bodies have moved to classify ME/CFS as a physical disease. None of this means every mechanism is understood — ME/CFS still has no single confirmed cause and no diagnostic biomarker in routine use, and it is honest to say so — but the once-dominant idea that it is fundamentally a disorder of belief and deconditioning has been substantially abandoned. The turning point in that shift was the public collapse of the case for graded exercise therapy.
The PACE Trial, Graded Exercise, and Post-Exertional Malaise
The most consequential and bitterly contested episode in modern ME/CFS history is the PACE trial, a large, government-funded British study led by Peter White and colleagues, published in The Lancet in 2011. PACE compared cognitive behavioural therapy (CBT) and graded exercise therapy (GET) against other approaches and reported that CBT and GET led to improvement, even “recovery,” for many patients. On the strength of PACE, GET and CBT became the officially recommended treatments for ME/CFS in the UK and influenced practice internationally — a powerful endorsement of the deconditioning model.
PACE drew intense criticism from patients, advocates, and a number of independent scientists, who raised serious methodological objections: notably that the trial changed its definitions of “improvement” and “recovery” partway through in ways that made the results look better, and that its reliance on subjective endpoints in an unblinded trial was unsound. After a years-long campaign — including a legal fight to release the trial's data — independent reanalyses of the PACE data (around 2016–2018) found the recovery and improvement rates to be far smaller than originally claimed once the trial's own original definitions were applied. PACE is now widely regarded as a cautionary tale in clinical-trial methodology, although its original authors continue to defend it; that disagreement is itself part of the record.
The deeper scientific reason GET fell out of favour is the recognition of post-exertional malaise (PEM) as the central, defining feature of ME/CFS — a delayed, disproportionate worsening of all symptoms after even modest physical or cognitive exertion, the very crash that Ramsay had described decades earlier. If exertion itself triggers relapse, then a therapy built on steadily increasing exertion is not merely ineffective but can cause real harm. Reflecting this, the UK's National Institute for Health and Care Excellence (NICE), in its 2021 guideline, stopped recommending graded exercise therapy for ME/CFS, recast CBT as a supportive (not curative) option, and placed PEM at the heart of diagnosis — alongside a management approach of pacing, in which patients stay within their available “energy envelope” rather than pushing through.
The 2015 Institute of Medicine Report and SEID
A landmark in the legitimisation of ME/CFS came on February 10, 2015, when the U.S. Institute of Medicine (IOM) — now the National Academy of Medicine — published a comprehensive report commissioned by federal health agencies. After reviewing thousands of studies, the IOM committee reached a blunt and historically important conclusion: ME/CFS is a serious, chronic, complex, multi-system biological disease, not a psychological disorder and emphatically “not in the patient's head.” For a community long accused of imagining its illness, an official statement of that kind from a leading scientific body was a watershed.
The report made several concrete contributions. It proposed simplified diagnostic criteria centred on a small set of core features — a substantial reduction in activity, post-exertional malaise, unrefreshing sleep, and either cognitive impairment or orthostatic intolerance — designed to be usable by ordinary clinicians. Crucially, it identified post-exertional malaise as a hallmark of the disease, reinforcing exactly the feature that undermined the exercise-therapy model. And it proposed a new name intended to capture that central feature: “systemic exertion intolerance disease” (SEID).
The proposed name SEID has had a mixed reception and has not been widely adopted, which is itself part of the honest history. Supporters argued it described the core problem — that exertion of any kind makes patients systemically ill — far better than “chronic fatigue syndrome.” Critics, including many patients, felt it still omitted the disease's neurological and immune dimensions and worried it would simply add a fifth name to an already confusing pile; many continue to prefer “ME” or the combined “ME/CFS.” The lasting legacy of the 2015 report is therefore less its naming proposal than its authoritative insistence that this is a real, physical, disabling disease deserving serious medical attention and research funding.
The Dismissal of Patients — An Honest Reckoning
No history of ME/CFS is truthful if it omits how badly patients have been treated. For decades, people with this illness — who can be too sick to work, to leave the house, or in the most severe cases to sit up, tolerate light, or feed themselves — have been routinely told that nothing was physically wrong with them. They have been disbelieved by doctors, denied diagnoses and benefits, accused of malingering or of “false illness beliefs,” and pushed into exercise programmes that made them sicker. The trivialising name “chronic fatigue syndrome” actively contributed to this, by making a devastating disease sound like everyday tiredness.
This dismissal has fallen hardest on those least able to fight it. Women, who make up the majority of patients, have disproportionately had their symptoms attributed to anxiety or depression. People with severe and very severe ME — bedbound, often unable to advocate for themselves — have at times been failed catastrophically by services that did not believe their condition was real or serious. And historically, the illness has been chronically under-funded relative to its burden, a direct downstream consequence of not being taken seriously. The harm done has been real and, in some documented cases, life-threatening.
The arc of this history, while still incomplete, bends toward recognition. The 2015 IOM report, the 2021 NICE guideline's rejection of harmful exercise therapy, the growing biomedical literature, and renewed research interest — intensified by the appearance of Long COVID, a post-viral condition that strongly overlaps ME/CFS — have all helped. But the central lesson of this history is a human one: patients reporting a real, exertion-worsened, multi-system illness were right, and were disbelieved for far too long. Telling the story accurately means saying that plainly.
Research Papers and References
The references below combine peer-reviewed papers on the history, naming, and science of ME/CFS with curated PubMed topic-search links into the historical and clinical literature. Where a precise editorial or primary source is named in the text (for example the 1956 Lancet editorial, or Beard's 1869 paper), it is described historically; the links here open the corresponding modern literature at PubMed, journal sites, or authoritative public-health pages in a new tab. Several reflect ongoing scholarly disagreement — they are included precisely because the history is contested.
- Institute of Medicine (U.S.) Committee. Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness. Washington (DC): National Academies Press; 2015. — NCBI Bookshelf: full IOM report
- Holmes GP, Kaplan JE, Gantz NM, et al. Chronic fatigue syndrome: a working case definition. Annals of Internal Medicine. 1988;108(3):387-389. — doi:10.7326/0003-4819-108-3-387
- White PD, Goldsmith KA, Johnson AL, et al. (PACE trial management group). Comparison of adaptive pacing therapy, cognitive behaviour therapy, graded exercise therapy, and specialist medical care for chronic fatigue syndrome (PACE): a randomised trial. The Lancet. 2011;377(9768):823-836. — doi:10.1016/S0140-6736(11)60096-2
- Wilshire CE, Kindlon T, Courtney R, et al. Rethinking the treatment of chronic fatigue syndrome — a reanalysis and evaluation of findings from a recent major trial of graded exercise and CBT. BMC Psychology. 2018;6:6. — doi:10.1186/s40359-018-0218-3
- Underhill R, Baillod R. Myalgic Encephalomyelitis, Chronic Fatigue Syndrome, and Systemic Exertion Intolerance Disease: Three Distinct Clinical Entities. Challenges. 2018;9(1):19. — doi:10.3390/challe9010019
- Underwood J, et al. Myalgic encephalomyelitis (ME) outbreaks can be modelled as an infectious disease: a mathematical reconsideration of the Royal Free Epidemic of 1955. Fatigue: Biomedicine, Health & Behavior. 2020;8(2):63-78. — doi:10.1080/21641846.2020.1793058
- Acheson ED. The clinical syndrome variously called benign myalgic encephalomyelitis, Iceland disease and epidemic neuromyasthenia. The American Journal of Medicine. 1959;26(4):569-595. — PubMed: 13637100
- Royal Free Hospital outbreak (1955) — original reports and reappraisals — PubMed: Royal Free 1955 outbreak
- George Beard, neurasthenia, and the history of the chronic-fatigue concept — PubMed: neurasthenia history and Beard
- Goudsmit E, Shepherd C, et al. Ramsay's definition and the clinical characterisation of myalgic encephalomyelitis — PubMed: Ramsay ME definition
- Incline Village / Lake Tahoe outbreak and the origins of the CFS case definition — PubMed: Incline Village CFS outbreak
- Post-exertional malaise in ME/CFS — mechanisms and measurement — PubMed: post-exertional malaise in ME/CFS
- The PACE trial controversy and graded exercise therapy — critiques and reanalyses — PubMed: PACE trial and GET controversy
- Systemic exertion intolerance disease (SEID) — the IOM name and its reception — PubMed: SEID and the IOM criteria
External Authoritative Resources
- CDC — About ME/CFS
- NICE Guideline NG206 (2021) — ME/CFS: diagnosis and management
- National Academies / IOM (2015) — Redefining an Illness
Connections
- Neurology
- Myalgic Encephalomyelitis / Chronic Fatigue Syndrome (ME/CFS)
- Fibromyalgia
- Postural Orthostatic Tachycardia Syndrome (POTS)
- Mast Cell Activation Syndrome (MCAS)
- All Conditions