Tick-Borne Encephalitis
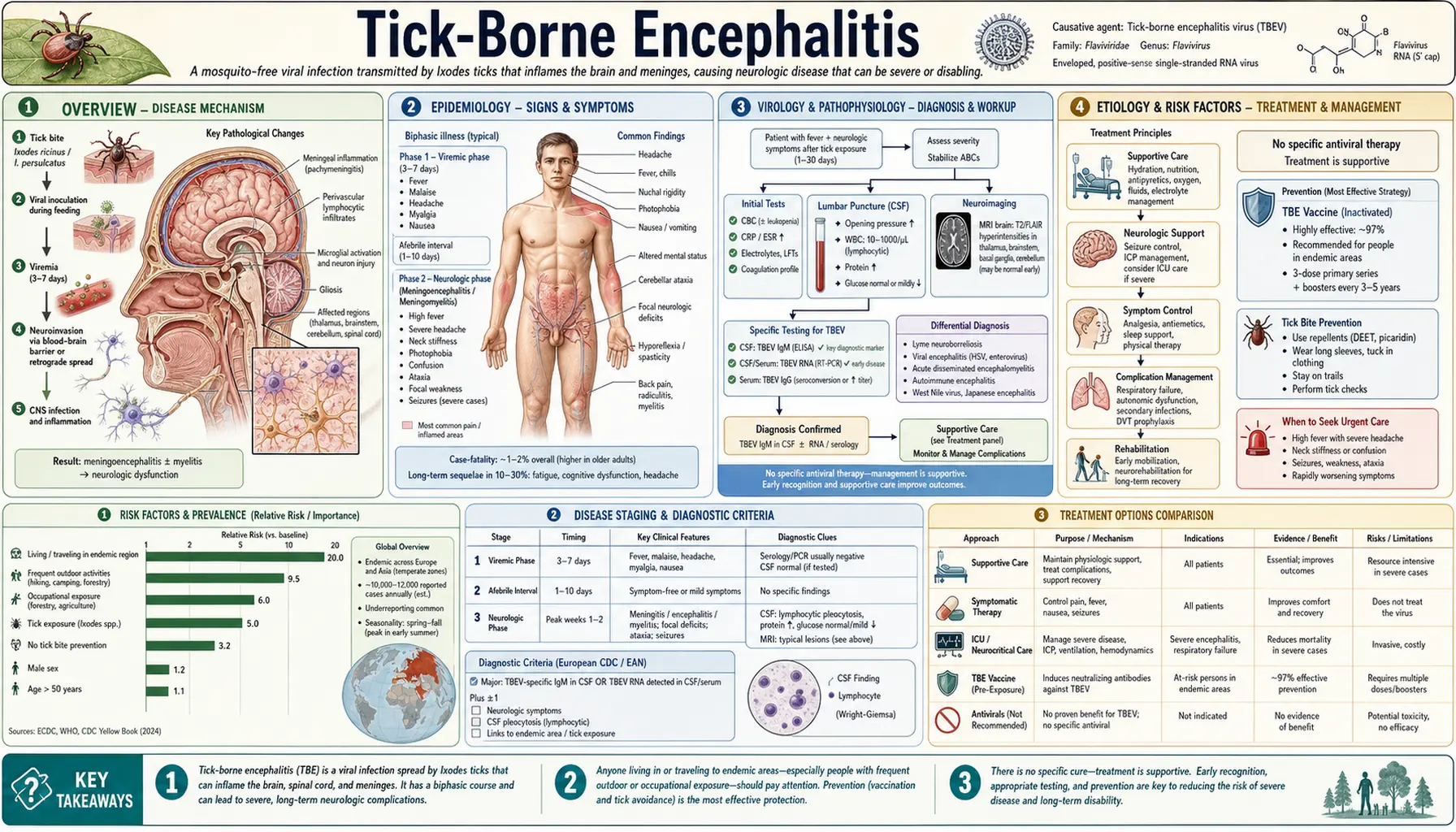
Table of Contents
- Overview
- Epidemiology
- Virology and Pathophysiology
- Etiology and Risk Factors
- Clinical Presentation
- TBE Subtypes by Virus Variant
- Diagnosis
- Treatment
- Vaccination
- Complications
- Prognosis
- Prevention
- References
- Research Papers
- Connections
- Featured Videos
1. Overview
Tick-Borne Encephalitis (TBE) is caused by the Tick-Borne Encephalitis Virus (TBEV), a flavivirus belonging to the family Flaviviridae and the genus Flavivirus. TBEV is a positive-sense single-stranded RNA virus and is closely related to West Nile virus, dengue, Zika, and yellow fever — all members of the Flaviviridae family. This close genetic relationship explains overlapping serological cross-reactivity that can complicate diagnosis.
TBEV is classified into three main subtypes, each with a distinct geographic range, tick vector, and clinical severity profile. The European subtype (TBEV-Eu) is transmitted by Ixodes ricinus (the castor bean tick) and circulates primarily in Central, Western, and Northern Europe; it causes the mildest disease of the three subtypes with a mortality rate of approximately 1–2%. The Siberian subtype (TBEV-Sib) is transmitted by Ixodes persulcatus (the taiga tick) across Russia and Siberia; it is more neuroinvasive than the European subtype, carries a 2–3% mortality rate, and is associated with chronic progressive encephalitis in some patients. The Far Eastern subtype (TBEV-FE), also transmitted by I. persulcatus across China, Japan, and Far Eastern Russia, is the most virulent; it follows a monophasic clinical course (in contrast to the characteristic biphasic pattern of the European subtype), presents as fulminant encephalitis, and carries a mortality rate of 5–35% in unvaccinated individuals — the highest of any tick-borne viral disease in Eurasia.
TBE represents a major public health problem across Eurasia. Approximately 10,000–12,000 clinical cases are reported annually across more than 35 countries in Europe and Asia, but significant underreporting is documented — true incidence is estimated to be 3–7 times higher than reported figures. Countries with the highest burden include Germany, Austria, the Czech Republic, Sweden, Finland, the Baltic states (Estonia, Latvia, Lithuania), and Russia. TBE is not currently endemic in the United States; the North American ecological equivalent is Powassan virus, a tick-borne flavivirus transmitted by Ixodes cookei and I. scapularis. American travelers to endemic regions of Europe and Asia are at risk and should be counseled accordingly.
One of the most clinically important distinguishing features of TBE compared with other major tick-borne diseases — Lyme disease, ehrlichiosis, anaplasmosis, Rocky Mountain spotted fever — is the existence of a highly effective licensed vaccine. TBE is a vaccine-preventable encephalitis. The WHO and European public health authorities recommend vaccination for endemic-area residents and for travelers planning extended or high-risk exposure in endemic regions. Despite vaccine availability, TBE remains underappreciated by travelers and some healthcare providers outside Europe, contributing to preventable cases.
2. Epidemiology
TBE is endemic across a broad swath of Eurasia, from Western Europe through Siberia and into East Asia. Approximately 10,000–12,000 cases are reported annually in Europe and Asia combined, with the true burden estimated at 3–7 times higher due to systematic underreporting, mild cases that never reach medical attention, and diagnostic gaps in lower-resource settings. The European subtype accounts for the majority of globally reported cases; the Siberian and Far Eastern subtypes predominate in Russia and Asia.
Countries with the highest incidence in Europe include the Baltic states (Estonia, Latvia, Lithuania), Slovenia, the Czech Republic, Austria, Sweden, Germany, and Finland. Within these countries, incidence is highest in forested, rural, and peri-urban areas where tick populations are dense and human outdoor activity is common. Russia and neighboring states (Belarus, Ukraine) carry a high burden of the Siberian subtype. The Far Eastern subtype is the dominant strain in Siberia, northeastern China, Japan, and the Korean Peninsula.
Seasonal pattern: TBE follows a bimodal seasonal distribution corresponding to tick activity — a primary peak in May–June (nymphal activity) and a secondary peak in September–October (adult tick activity). Cases are rare during winter months when ticks are dormant. Climate change is documented as expanding both the northern and higher-altitude distribution of I. ricinus, with TBE cases now reported in Scandinavia at latitudes and altitudes where the disease was historically absent.
Risk groups: Forestry workers, farmers, hunters, military personnel, and hikers in endemic areas bear the greatest occupational and recreational risk. Children and young adults in endemic countries are frequently exposed through outdoor play and summer activities. An often-overlooked transmission route is raw milk consumption — TBEV is secreted into the milk of infected ruminants (goats, sheep, and cattle) and can cause alimentary TBE through unpasteurized milk or dairy products; family and community clusters from this route have been documented in multiple countries.
Travel-acquired TBE is increasingly recognized, with cases reported in travelers returning from endemic regions of Europe and Asia to non-endemic countries including the United States, Canada, Australia, and the United Kingdom. The majority of travel-acquired TBE cases involve unvaccinated travelers who underestimated their risk.
Mortality by subtype: European subtype 1–2%; Siberian subtype 2–3%; Far Eastern subtype 5–35% (unvaccinated). Elderly individuals and those with significant neurological disease at presentation consistently have the highest mortality and most severe outcomes across all subtypes.
3. Virology and Pathophysiology
TBEV is a small (approximately 40–50 nm), enveloped, positive-sense single-stranded RNA virus with a genome of approximately 11 kilobases encoding three structural proteins (capsid C, pre-membrane prM, and envelope E) and seven non-structural proteins (NS1, NS2A, NS2B, NS3, NS4A, NS4B, NS5). The envelope E protein mediates viral attachment to host cell receptors and membrane fusion, and is the primary target of neutralizing antibodies — the basis of both natural immunity and vaccine-induced protection. The close structural similarity of E proteins across flaviviruses explains the serological cross-reactivity between TBEV and other flaviviruses such as West Nile virus and dengue.
Entry and early replication: After a tick bite, TBEV replicates at the skin inoculation site in Langerhans cells and local dendritic cells, followed by transport to regional lymph nodes and subsequent viremia. The viral envelope protein binds to glycosaminoglycans and potentially DC-SIGN on target cells, initiating receptor-mediated endocytosis and pH-dependent membrane fusion within endosomes, releasing the genome into the cytoplasm for replication.
CNS invasion: TBEV crosses the blood-brain barrier (BBB) through multiple mechanisms: direct infection of brain microvascular endothelial cells, transcytosis across the BBB, and possibly retrograde neuronal transport from peripheral olfactory neurons. Once in the CNS, the virus displays pronounced neurotropism, infecting neurons (the primary target), astrocytes, and microglia. Neuronal infection results in necrosis and inflammatory infiltrates most prominently in the cerebellum (producing the clinical ataxia and dysarthria characteristic of TBE), brainstem, spinal cord anterior horn cells (producing poliomyelitis-like flaccid paralysis), thalamus, and cortex. The distribution of pathology directly predicts the clinical syndrome.
The biphasic illness pattern — the hallmark of European subtype TBE — results from the temporal separation of the viremic and neuroinvasive phases. During Phase 1, virus circulates freely in blood and replicates in lymphoid tissues and peripheral organs, producing systemic flu-like symptoms. Approximately 70% of infected individuals clear the virus at this stage without CNS involvement and recover completely. In the remaining ~30%, after an asymptomatic interval of 7–10 days, the virus invades the CNS while circulating antibodies are rising but insufficient to prevent neuroinvasion. This accounts for the paradox that Phase 2 neurological disease worsens despite the presence of detectable antibodies in serum.
Immune evasion: TBEV employs several strategies to evade innate immune responses. The NS5 protein inhibits interferon (IFN) signaling by blocking STAT1/STAT2 phosphorylation, impairing type I interferon-mediated antiviral defense. NS3, NS4A, and NS4B proteins collectively suppress innate immune activation through multiple mechanisms. This robust immune evasion strategy contributes to the ability of the virus to establish viremia and CNS invasion despite an active immune response.
Immunopathology contributes significantly to CNS injury in TBE. The inflammatory infiltrate — predominantly CD8+ T lymphocytes and activated macrophages/microglia — while targeting virus-infected neurons, causes collateral neuronal damage. Bystander T-cell activation and cytokine-mediated injury (TNF-α, IFN-γ) amplify tissue destruction beyond directly virus-infected cells, explaining the severity of neurological deficits that can persist well beyond viral clearance from the CNS.
4. Etiology and Risk Factors
Tick vectors: Ixodes ricinus (the European castor bean tick) is the primary vector for the European subtype (TBEV-Eu) and is responsible for the vast majority of TBE cases in Central, Western, and Northern Europe. Ixodes persulcatus (the taiga tick) transmits both the Siberian and Far Eastern subtypes across Russia, Siberia, northeastern China, and Japan. All life stages of both tick species — larvae, nymphs, and adults — are capable of transmitting TBEV after feeding on an infected vertebrate host. Nymphs are most commonly responsible for human infection due to their small size (1–2 mm), which makes them difficult to detect during tick checks.
Critical transmission difference from Lyme disease and ehrlichiosis: Unlike Borrelia burgdorferi (Lyme disease) and Ehrlichia/Anaplasma species, which require 24–36 hours of tick attachment before transmission occurs, TBEV can be transmitted within minutes of tick attachment. This is because TBEV, unlike Lyme spirochetes, does not need to migrate from the tick midgut to salivary glands during feeding — it is already present in tick saliva at the beginning of the blood meal. This fundamentally alters the prevention calculus: while prompt tick removal is still valuable and should always be performed, it cannot be relied upon to reliably prevent TBE as it can for Lyme disease. Vaccination is therefore the most effective prevention strategy for individuals with ongoing endemic-area exposure.
Alimentary (oral) transmission: TBEV is secreted into the milk of infected goats, sheep, and cattle during viremia. Consumption of unpasteurized (raw) milk or cheese from these animals can result in alimentary TBE. This route accounts for documented family and community clusters — often involving multiple members of a household consuming the same raw dairy product. Pasteurization reliably eliminates TBEV; boiling milk is also sufficient to inactivate the virus. Travelers and residents in endemic areas who consume local artisanal or farmstead dairy should be counseled specifically about this risk.
Risk factors for acquiring TBE:
- Residence in or travel to TBE-endemic areas in Europe or Asia, particularly forested, rural, or peri-urban environments with high tick density.
- Outdoor occupational exposure: forestry workers, farmers, hunters, military personnel, wildlife biologists, and agricultural workers in endemic regions.
- Recreational outdoor activities: hiking, camping, orienteering, mountain biking, and berry/mushroom picking in forested endemic areas.
- Consumption of unpasteurized milk or dairy products from goats, sheep, or cattle in endemic areas.
- Unvaccinated status — the single most important modifiable risk factor.
- Age over 50 years is associated with more severe neurological disease and worse outcomes, though all age groups can acquire infection.
Risk factors for severe disease:
- Advancing age (>60 years) — consistently the strongest predictor of severe neurological outcome and death across all subtypes and geographic regions.
- Immunosuppression: HIV/AIDS, hematological malignancies, solid organ or stem cell transplantation, high-dose corticosteroid therapy, biologic immunomodulatory agents (anti-TNF therapy, rituximab). Chronic progressive TBE is specifically documented in patients with agammaglobulinemia and other primary antibody deficiencies.
- Infection with the Siberian or Far Eastern subtype rather than the European subtype.
- Delayed diagnosis or presentation with meningoencephalomyelitis rather than meningitis-only form.
5. Clinical Presentation
The incubation period for TBE is typically 7–14 days (range 2–28 days) after a tick bite. Alimentary (raw milk) transmission has a shorter incubation of approximately 3–4 days. A history of a recognized tick bite or raw dairy consumption in an endemic area is important to elicit, but many patients do not recall a tick bite.
The most characteristic feature of European subtype TBE is a biphasic illness, which develops in approximately 30% of those infected (the remaining 70% experience either asymptomatic infection or a subclinical Phase 1 febrile illness without progression to neurological disease). The biphasic pattern is less consistent with the Siberian subtype and often absent with the Far Eastern subtype, which typically presents as a monophasic fulminant encephalitis.
Phase 1 — Viremic Phase
Duration: 3–7 days. Onset after 7–14 days incubation. This phase represents systemic viral replication and viremia. Symptoms are nonspecific and resemble influenza or other viral illnesses: fever (38–39°C), malaise, profound fatigue, myalgia, arthralgia, and headache. Nausea, loss of appetite, and conjunctival injection may also occur. Laboratory findings may include leukopenia, thrombocytopenia, and mildly elevated C-reactive protein (CRP), though these are inconsistent.
TBEV is detectable by PCR in blood during this phase. The majority of infected individuals (approximately 70%) recover fully from Phase 1 without progressing to neurological disease. Those who do progress to Phase 2 experience an asymptomatic interval of typically 7–10 days (range 1–21 days) during which symptoms abate and patients may believe they are recovering.
Phase 2 — Neurological Phase
Phase 2 begins with the abrupt recurrence of fever — typically higher than Phase 1 (39–41°C) — accompanied by severe headache, neck stiffness (meningismus), nausea, and vomiting. At this point the virus has crossed the blood-brain barrier and CSF pleocytosis is present. The severity of neurological involvement determines the clinical form:
- Meningitis form (approximately 50% of neurological TBE cases): Fever, severe headache, photophobia, phonophobia, and meningismus without encephalitic features. CSF shows lymphocytic pleocytosis. This is the most benign form; full recovery within 1–4 weeks is the rule, and permanent sequelae are uncommon.
- Meningoencephalitis (approximately 40% of neurological cases): Meningitis features plus encephalitic involvement — impaired consciousness ranging from drowsiness and disorientation to stupor or coma, cognitive dysfunction (confusion, memory impairment), psychiatric features (agitation, anxiety, depression), tremor, cerebellar ataxia (unsteady gait, dysarthria, nystagmus), and cranial nerve palsies. Ataxia and tremor are particularly prominent in TBE compared with other viral encephalitides, reflecting the predilection of TBEV for the cerebellum. This form carries significant risk of prolonged post-encephalitic syndrome.
- Meningoencephalomyelitis (approximately 10% of neurological cases; most severe form): Meningoencephalitis plus involvement of the spinal cord and/or anterior horn cells, producing the most feared complication of TBE — flaccid paralysis with a poliomyelitis-like distribution. This paralysis is typically asymmetric, involves the upper limbs and shoulder girdle preferentially (the so-called "floppy arm syndrome" or TBE myelopathy), and results from destruction of anterior horn motor neurons. Bulbar palsy (dysphagia, dysphonia, dysarthria) from brainstem motor nucleus involvement can cause aspiration and respiratory compromise. Respiratory muscle paralysis is a medical emergency requiring mechanical ventilation. This form has the worst prognosis for full neurological recovery, with permanent flaccid paralysis in a significant proportion of survivors.
- Polyradiculoneuritis (rare): A peripheral neuropathy pattern with radicular pain, weakness, and sensory changes; may occur in isolation or accompany central neurological findings.
Cerebellar involvement — ataxia, dysmetria, dysarthria, nystagmus — is a particularly characteristic and frequently prominent feature of TBE that helps distinguish it from other viral encephalitides. Tremors of the hands, lips, and tongue are also common.
6. TBE Subtypes by Virus Variant
European subtype (TBEV-Eu): The most geographically widespread and extensively studied subtype. Vector: Ixodes ricinus. Distribution: Central, Western, and Northern Europe, including Austria, Germany, Czech Republic, Slovenia, Switzerland, the Baltic states, Sweden, Finland, Norway, and parts of France and Italy. The biphasic clinical pattern is most clearly expressed with this subtype, occurring in approximately one-third of those with neurological disease. Overall case fatality rate 1–2% (higher in elderly). Permanent neurological sequelae occur in 30–50% of those with meningoencephalitis or meningoencephalomyelitis. The European subtype is the most amenable to vaccine prevention, and the commercially available TBE vaccines were developed primarily against this variant.
Siberian subtype (TBEV-Sib): Vector: Ixodes persulcatus. Distribution: Russia (western Siberia, Urals, European Russia), Kazakhstan, Baltic states (where both TBEV-Eu and TBEV-Sib overlap), and parts of Finland. This subtype is more neuroinvasive than TBEV-Eu and carries a case fatality rate of 2–3%. A distinctive feature of TBEV-Sib is its capacity to cause chronic progressive TBE — a slowly progressive encephalopathy resembling subacute sclerosing panencephalitis — particularly in immunocompromised patients with impaired antibody responses (agammaglobulinemia, hypogammaglobulinemia). The biphasic pattern may be less distinctly expressed, and the asymptomatic interval may be shorter or absent.
Far Eastern subtype / Russian Spring-Summer Encephalitis (TBEV-FE): Vector: Ixodes persulcatus. Distribution: Far Eastern Russia, northeastern China, Japan, and the Korean Peninsula. This is the most virulent of the three subtypes and the cause of the classical "Russian spring-summer encephalitis" described in Soviet-era literature from the 1930s and 1940s. TBEV-FE typically causes a monophasic illness — the biphasic pattern of the European subtype is usually absent, and encephalitis develops from the outset without a preceding asymptomatic interval. The clinical course is often fulminant, with rapid progression to deep coma, severe flaccid paralysis, and respiratory failure. Case fatality rate in unvaccinated individuals is 5–35%, the highest of any tick-borne viral disease in Eurasia. Survivors frequently have severe permanent neurological deficits.
Louping Ill Virus: A related but phylogenetically distinct tick-borne flavivirus found in the United Kingdom and Ireland, transmitted by I. ricinus. Primarily a disease of sheep and red grouse; human cases are rare and occur almost exclusively in occupationally exposed individuals (veterinarians, farmers, slaughterhouse workers, and laboratory workers). Human clinical disease resembles European TBE with meningitis or meningoencephalitis. Cross-protective capacity of TBE vaccines against louping ill virus is partial; TBE vaccination is not a reliable substitute for occupational precautions in louping ill-endemic areas.
Powassan virus (North American equivalent): While not a subtype of TBEV, Powassan virus is a closely related tick-borne flavivirus and the primary tick-borne neuroinvasive flavivirus endemic to North America. Transmitted by I. cookei (the groundhog tick) and I. scapularis (the black-legged tick) in the northeastern and north-central United States and Canada. Powassan encephalitis is severe, with mortality of approximately 10–15% and permanent neurological deficits in 50% of survivors. Unlike TBE, there is no licensed human vaccine against Powassan virus, and TBE vaccines do not reliably cross-protect against it.
7. Diagnosis
The diagnosis of TBE requires clinical suspicion based on the combination of: (1) exposure history — tick bite, time spent in a TBE-endemic area, or consumption of unpasteurized dairy; (2) characteristic clinical presentation — biphasic febrile illness or encephalitis with cerebellar features; and (3) laboratory confirmation. As with many tick-borne and viral diseases, empiric management while awaiting confirmatory results is appropriate in the right clinical context.
Serology (Primary Diagnostic Method)
Detection of TBEV-specific IgM and IgG antibodies is the diagnostic standard for TBE. TBEV-specific IgM typically appears 1–2 weeks after symptom onset; IgG develops 2–4 weeks after onset. The preferred method is ELISA for initial screening, with plaque reduction neutralization test (PRNT) used for confirmation when cross-reactivity with other flaviviruses (dengue, West Nile virus, yellow fever vaccine-induced antibodies) must be excluded. PRNT is the gold standard for serological specificity.
Both serum AND CSF should be submitted for antibody testing in patients with neurological disease. Demonstration of intrathecal TBEV antibody production (elevated CSF:serum IgG antibody ratio, or the presence of TBEV IgM in CSF) provides strong evidence of active CNS infection and distinguishes TBE from incidental seropositivity due to past vaccination or prior infection.
Cross-reactivity with dengue, yellow fever vaccine, and West Nile virus antibodies must be considered, particularly in travelers who may have received flavivirus vaccines. PRNT is essential in these cases.
PCR
Reverse-transcription PCR (RT-PCR) for TBEV RNA in blood is positive during Phase 1 (viremic phase) but becomes negative as viremia clears before Phase 2 neurological symptoms. This is a critical limitation: PCR is usually negative when the patient presents with encephalitis. RT-PCR on blood is most useful if a patient presents during Phase 1 fever, which is rarely the case in practice. PCR on CSF has very low sensitivity in Phase 2 and is not a reliable diagnostic tool at the time of neurological presentation.
CSF Analysis
Lumbar puncture is essential for patients with neurological TBE. Typical findings: lymphocytic pleocytosis (100–1,000 cells/μL; predominantly mononuclear), elevated protein (0.5–1.5 g/L), and normal glucose (unless bacterial superinfection is suspected). TBEV-specific IgM in CSF is a highly specific marker of neuroinvasive disease. Culture is uniformly negative.
MRI and EEG
Brain MRI shows T2/FLAIR hyperintensities in the thalami, basal ganglia, cerebellum, cortex, and brainstem in severe cases — findings that correlate with areas of neuronal necrosis and inflammation. MRI is normal in the meningitis-only form. Spinal cord MRI in meningoencephalomyelitis may show T2 signal changes in the anterior horn regions. EEG demonstrates diffuse slowing and, in some cases, spike-wave complexes consistent with encephalopathy.
Differential Diagnosis
Key entities to consider and exclude: Herpes simplex encephalitis (HSV-1/2) — requires empiric acyclovir while awaiting HSV PCR on CSF (treatment is time-sensitive and entirely different from TBE management); bacterial meningitis (CSF glucose low, neutrophilic pleocytosis, positive bacterial culture); other viral encephalitides (West Nile virus, enterovirus, mumps, measles); Lyme neuroborreliosis (different geographic exposure, CSF intrathecal Lyme antibody production); rickettsial disease (RMSF, ehrlichiosis — rash, thrombocytopenia, responds to doxycycline); autoimmune encephalitis (anti-NMDAR and other antibody-mediated encephalitides — no infectious exposure history, serum/CSF autoantibody panel).
8. Treatment
No specific antiviral treatment for TBE is currently available. Unlike many other serious infectious diseases, there is no drug analogous to acyclovir for herpes encephalitis or doxycycline for tick-borne bacterial diseases. Management is entirely supportive and symptomatic, with the primary goals of controlling systemic and cerebral complications, preventing secondary infections, and maximizing neurological recovery through rehabilitation.
Hospitalization and Monitoring
All patients with neurological TBE (meningitis, meningoencephalitis, or meningoencephalomyelitis) require inpatient care. Patients with meningoencephalomyelitis, altered consciousness, or any evidence of respiratory compromise require intensive care unit (ICU) admission. Neurological status, fever, and respiratory function should be monitored closely, with particular attention to bulbar function (swallowing, phonation, cough reflex) and oxygen saturation as indicators of imminent respiratory failure.
Fever and Pain Management
Paracetamol (acetaminophen) is the preferred antipyretic and analgesic. NSAIDs may be used with caution but are generally avoided in severe or complicated TBE due to concerns about platelet function and gastrointestinal effects in systemically unwell patients.
Corticosteroids
Corticosteroids are not routinely recommended for TBE. Unlike bacterial meningitis, where dexamethasone has demonstrated benefit in reducing inflammation and hearing loss, there is no robust evidence that corticosteroids improve outcomes in viral encephalitis including TBE. Some expert opinion supports a limited, closely monitored trial of corticosteroids (e.g., dexamethasone) exclusively for life-threatening cerebral edema with clinical deterioration, but this must be individualized with specialist consultation and should not become routine practice.
Seizure Management
Acute seizures should be treated with benzodiazepines (lorazepam or diazepam IV). For ongoing seizure management or EEG-confirmed subclinical seizures, levetiracetam or valproate are preferred. Post-encephalitic epilepsy may require long-term antiepileptic therapy.
Respiratory Support
Respiratory compromise is the primary life-threatening complication of meningoencephalomyelitis with bulbar or respiratory muscle involvement. Early respiratory assessment — including regular monitoring of forced vital capacity in patients with any bulbar symptoms — is critical. Progressive respiratory insufficiency requires non-invasive ventilation (BiPAP/CPAP) transitioning to endotracheal intubation and mechanical ventilation as needed. Some patients require prolonged ventilatory support, and tracheostomy may be necessary.
Passive Immunization — TBE Immunoglobulin (TBEIg)
Human TBE-specific immunoglobulin (TBEIg) was previously used in Central Europe (particularly Austria and Germany) for post-exposure prophylaxis in unvaccinated individuals after a tick bite in an endemic area. This practice has been largely withdrawn following evidence — most prominently from Austrian pediatric and adult case series — that TBEIg administered after symptoms develop may paradoxically worsen neurological outcome, possibly through an antibody-dependent enhancement mechanism similar to that seen with dengue. The current consensus is that TBEIg is appropriate only if administered within 96 hours of tick bite and before any symptom onset; it is contraindicated once symptoms have developed. The practical utility of TBEIg is therefore very limited, and it is no longer routinely stocked or recommended in most European countries. Vaccination before exposure remains the only reliable preventive strategy.
Rehabilitation
Intensive physical therapy, occupational therapy, and speech-language pathology are central to management of patients with flaccid paralysis, ataxia, tremor, dysarthria, or cognitive impairment. Rehabilitation should begin as early as the patient's condition permits and may need to continue for many months. Recovery from TBE myelopathy (flaccid paralysis) is often partial and prolonged; some patients plateau with permanent deficits, while others achieve meaningful functional improvement over 12–24 months with sustained rehabilitation.
9. Vaccination
TBE is one of the very few tick-borne diseases — and one of the few encephalitides — for which a highly effective licensed vaccine exists. Vaccination is the cornerstone of TBE prevention for endemic-area residents and a critical recommendation for travelers planning exposure in high-risk regions. The availability of effective vaccination makes TBE prevention fundamentally different from the situation with most other tick-borne diseases.
Available Vaccines
Multiple TBE vaccines are licensed globally. All currently licensed products are based on formalin-inactivated TBEV antigen (whole virus) grown in chick embryo fibroblast cell culture, adsorbed onto aluminum hydroxide adjuvant.
- FSME-IMMUN (Pfizer; marketed as TICOVAC in the US and Canada) and ENCEPUR (Bavarian Nordic/CSL): The two primary vaccines licensed in Europe and North America, both derived from European subtype TBEV strains. FSME-IMMUN has a pediatric formulation (0.25 mL) for children aged 1–15 years; the adult formulation (0.5 mL) is used from age 16.
- Tick-E-Vac / TBE-Moscow (Russia): Russian-manufactured vaccines licensed in Russia and neighboring countries; derived from the Siberian/Far Eastern subtype strains; used primarily in Russia for subtype-appropriate protection.
- ENCEVIR (Russia): Another Russian-licensed product based on Far Eastern subtype antigen.
Vaccination Schedules
Standard (conventional) schedule (FSME-IMMUN / ENCEPUR): Three doses — dose 1 at day 0, dose 2 at 1–3 months, dose 3 at 5–12 months after dose 2. The first two doses provide initial protection (approximately 90% after 2 doses); the third dose extends and consolidates immunity. Full protection is not achieved until after dose 3.
Rapid schedule: For travelers with insufficient time for the conventional schedule — dose 1 at day 0, dose 2 at day 7, dose 3 at day 21. This accelerated schedule achieves protective antibody levels more quickly but requires a booster at 12–18 months to maintain long-term immunity.
Booster doses: First booster at 3 years after primary series completion; subsequent boosters every 3–5 years for continuing exposure (some guidelines recommend every 5 years in those under 60, every 3 years in those over 60 given waning immunity with age).
Efficacy and Cross-Protection
TBE vaccines based on the European subtype are 95–99% effective against TBE after primary series completion — an exceptionally high efficacy for an encephalitis vaccine. Cross-neutralization between the European, Siberian, and Far Eastern subtypes is substantial but not complete; vaccines developed against the European subtype provide significant but potentially reduced protection against the Far Eastern subtype. For individuals traveling to Far Eastern Russia, China, or Japan, TBE vaccination is still strongly recommended as providing meaningful protection, though specific data on Far Eastern subtype protection efficacy from European-strain vaccines are limited. The Russian Far Eastern-strain vaccines may offer somewhat better subtype-matched protection for travelers in those regions where they are available.
Safety
TBE vaccines are generally well tolerated. Local injection site reactions (redness, swelling, pain) occur in 50–70% of recipients. Systemic reactions (fever, myalgia, fatigue, headache) are more common in children (10–30%) than adults. Fever after the first dose in children is the most commonly reported adverse event and is self-limited. Serious adverse events (severe allergic reactions, neurological events) are rare. The vaccines are contraindicated in individuals with known severe allergic reactions to egg protein, as they are produced in chick embryo cell cultures (cell-culture derived alternatives may be available in some markets). Consult current prescribing information for up-to-date contraindications and precautions.
Indications for Vaccination
- Residents of TBE-endemic areas in Europe and Asia — especially those with outdoor occupational or recreational exposure.
- Travelers to high-risk endemic regions who will have outdoor exposure in forested or rural areas; consult a travel medicine specialist at least 4–8 weeks before departure to allow completion of at least two doses before travel.
- Laboratory workers handling TBEV or working with infected materials.
- Military personnel deployed to endemic areas.
- TBE vaccination is not currently recommended in the United States for the general population given the absence of endemic TBEV transmission; it is available through travel medicine clinics for travelers to endemic regions.
- Note: TBE vaccination does NOT protect against Powassan virus (the North American tick-borne flavivirus) or other non-TBE flaviviruses. Cross-protection is uncertain and should not be assumed.
10. Complications
- Post-encephalitic syndrome: The most common complication overall. Cognitive impairment (memory deficits, concentration difficulties, executive dysfunction), fatigue, depression, anxiety, emotional lability, sleep disturbances, and headaches persist in 40–50% of patients with meningoencephalitis or meningoencephalomyelitis for months to years after the acute illness. This post-TBE syndrome significantly impairs quality of life and work capacity; recovery continues slowly over 12–24 months but some deficits may be permanent.
- Flaccid paralysis (TBE myelopathy): The most feared neurological complication of meningoencephalomyelitis. Results from destruction of anterior horn motor neurons in the cervical and thoracic spinal cord. Characteristically asymmetric; the shoulder-arm girdle is the predominant distribution (distinguishing it from other causes of flaccid paralysis). Paralysis is permanent in 10–20% of those who develop myelitis; partial recovery occurs in others over months to years of intensive rehabilitation. Permanent disability requiring adapted living may result.
- Chronic progressive TBE: A slowly progressive neurological deterioration resembling subacute sclerosing panencephalitis, documented primarily with the Siberian subtype in immunocompromised patients — particularly those with primary or secondary agammaglobulinemia who cannot mount a protective antibody response. This rare but devastating complication may develop months or years after the initial infection.
- Post-encephalitic epilepsy: Seizure disorder developing after TBE encephalitis in a small proportion of patients; may require long-term antiepileptic medication.
- Psychiatric sequelae: Anxiety disorders, depression, post-traumatic stress disorder (PTSD), and personality changes are documented in survivors of severe TBE and may persist independently of cognitive deficits. Psychological support and mental health follow-up should be integrated into post-TBE care.
- Respiratory failure: Bulbar and respiratory muscle weakness from brainstem and spinal cord involvement can necessitate prolonged mechanical ventilation. Tracheostomy may be required. Aspiration pneumonia is a frequent complication of bulbar palsy.
- Death: Mortality varies by subtype — European 1–2%, Siberian 2–3%, Far Eastern 5–35% — and is highest in elderly patients, those with meningoencephalomyelitis, and the immunocompromised. The majority of deaths occur from respiratory failure, brainstem herniation in severe cerebral edema, or secondary infections in the ICU.
11. Prognosis
Meningitis-only form: Excellent prognosis. Patients with TBE presenting as aseptic meningitis without encephalitic features typically recover fully within 1–4 weeks. Permanent neurological sequelae are uncommon. This form does not require ICU-level care in the majority of cases.
Meningoencephalitis: Intermediate prognosis. The majority of patients survive the acute illness, but 40–50% experience significant post-encephalitic symptoms — cognitive impairment, fatigue, headaches, depression — that persist for months to years. Recovery is often gradual and incomplete. Some patients achieve near-complete functional recovery over 12–24 months with sustained rehabilitation; others plateau with permanent cognitive or functional deficits. Return to full work capacity may be delayed or impossible for some patients.
Meningoencephalomyelitis: Poorest prognosis of the three neurological forms. Flaccid paralysis of the shoulder-arm girdle is the defining sequela and is permanent in approximately 10–20% of those who develop myelitis. Bulbar complications drive mortality risk. Extended ICU stays are common. Recovery of arm and shoulder function is often partial at best; some patients require ongoing supportive care and adapted living arrangements.
Predictors of poor neurological outcome: Age over 60 years (the single strongest predictor); infection with Far Eastern or Siberian subtype rather than European; clinical presentation with meningoencephalomyelitis rather than meningitis; presence of bulbar symptoms or respiratory compromise; immunosuppression; delayed hospital presentation; initial severity of encephalopathy (GCS score). Age over 60 and meningoencephalomyelitis form are additive risk factors for both mortality and permanent disability.
Recovery timeline: The acute illness phase typically lasts 2–4 weeks. Post-encephalitic symptoms may persist for 12–24 months. Improvement in cognitive function and fatigue continues slowly; some deficits plateau and some patients recover remarkably given time. Early and sustained engagement with physiotherapy, occupational therapy, speech therapy, and neuropsychological rehabilitation is associated with better functional outcomes. Regular neurological follow-up at 3, 6, and 12 months post-discharge is recommended for patients with meningoencephalitis or meningoencephalomyelitis.
12. Prevention
Vaccination (see Section 9) is the most effective prevention strategy for TBE and should be the primary recommendation for endemic-area residents and travelers planning exposure in high-risk forested or rural areas of Europe and Asia. Vaccination is particularly important given that TBEV can be transmitted within minutes of tick attachment, making tick removal an unreliable prevention measure for TBE (unlike Lyme disease, where prompt tick removal within 24–36 hours is highly protective).
Non-Vaccine Tick Bite Prevention
Personal protection measures remain valuable for reducing overall tick exposure and preventing co-transmitted pathogens, even if they cannot reliably prevent TBE from a single tick bite:
- Apply DEET (20–30%) or picaridin to exposed skin; apply permethrin to clothing, boots, and gear (not directly to skin). Permethrin-treated clothing retains acaricidal activity through multiple washings.
- Wear light-colored clothing with long sleeves and pants tucked into socks in tick-endemic areas; light colors facilitate tick detection.
- Conduct regular, thorough tick checks (scalp, behind ears, axillae, groin, popliteal fossa, umbilicus) after time in wooded or grassy areas. Pay particular attention to finding and removing I. ricinus nymphs, which are 1–2 mm and easily overlooked.
- Remove attached ticks promptly with fine-tipped tweezers — grasp as close to the skin surface as possible and pull upward with steady, even pressure. Do not twist, squeeze the tick body, or apply substances (petroleum jelly, heat). Clean the bite site with alcohol or soap and water. While early tick removal cannot reliably prevent TBE transmission (given the rapidity of TBEV transmission), prompt removal reduces co-infection risk from Lyme disease and other pathogens and should always be performed.
- Shower promptly after outdoor activities in endemic areas.
Dietary Prevention in Endemic Areas
Avoid consuming unpasteurized (raw) milk and raw dairy products (cheese, yogurt, butter) from goats, sheep, or cattle in TBE-endemic areas. TBEV is reliably inactivated by pasteurization. Boiling milk is also sufficient to inactivate the virus if pasteurization is unavailable. Travelers to endemic regions who seek out local artisanal or farmstead dairy should be specifically counseled about this risk, which is often overlooked.
Travel Medicine Preparation
Travelers planning outdoor activities in TBE-endemic areas of Europe or Asia should:
- Consult a travel medicine clinic at least 4–8 weeks before departure to allow time for at least two doses of TBE vaccine before travel (ideally completing the primary series).
- Check current CDC Traveler's Health destination pages and the ECDC (European Centre for Disease Prevention and Control) TBE maps for up-to-date risk areas within each country — risk is highly focal within endemic countries, concentrated in forested regions, and varies by season.
- Discuss the need for rapid-schedule vaccination if departure is imminent.
Occupational Prevention
Forestry workers, military personnel, farmers, agricultural workers, and outdoor laboratory researchers in endemic areas should be covered by formal occupational TBE vaccination programs, regular tick surveillance, provision of DEET/permethrin-treated personal protective equipment, and education about tick bite recognition and prompt removal. Many European countries with high endemic TBE burden have national occupational vaccination guidelines.
13. References
- Lindquist L, Vapalahti O. Tick-borne encephalitis. Lancet. 2008;371:1861–1871. PMID: 18514730. https://doi.org/10.1016/S0140-6736(08)60800-4
- Bogovic P, Strle F. Tick-borne encephalitis: a review of epidemiology, clinical characteristics, and management. World J Clin Cases. 2015;3:430–441. PMID: 26000308. https://doi.org/10.12998/wjcc.v3.i5.430
- Mansfield KL, Johnson N, Phipps LP, Stephenson JR, Fooks AR, Solomon T. Tick-borne encephalitis virus — a review of an emerging zoonosis. J Gen Virol. 2009;90:1781–1794. PMID: 19420159. https://doi.org/10.1099/vir.0.011437-0
- Gritsun TS, Lashkevich VA, Gould EA. Tick-borne encephalitis. Antiviral Res. 2003;57:129–146. PMID: 12615309. https://doi.org/10.1016/s0166-3542(02)00206-1
- Kaiser R. Tick-borne encephalitis. Infect Dis Clin North Am. 2008;22:561–575. PMID: 18755393. https://doi.org/10.1016/j.idc.2008.03.013
- Heinz FX, Stiasny K. Tick-borne encephalitis. Antiviral Res. 2012;93:1–15. PMID: 22100386. https://doi.org/10.1016/j.antiviral.2011.10.002
- Dumpis U, Crook D, Oksi J. Tick-borne encephalitis. Clin Infect Dis. 1999;28:882–890. PMID: 10825054. https://doi.org/10.1086/515195
- Bogovic P, Lotric-Furlan S, Strle F. What tick-borne encephalitis may look like: clinical signs and symptoms. Travel Med Infect Dis. 2010;8:246–250. PMID: 20637426. https://doi.org/10.1016/j.tmaid.2010.05.011
- Amicizia D, Domnich A, Panatto D, et al. Epidemiology of tick-borne encephalitis (TBE) in Europe and its prevention by available vaccines. Hum Vaccin Immunother. 2013;9:1163–1171. PMID: 23377671. https://doi.org/10.4161/hv.23802
- Suss J. Tick-borne encephalitis 2010: epidemiology, risk areas, and virus strains in Europe and Asia — an overview. Ticks Tick Borne Dis. 2011;2:2–15. PMID: 21771528. https://doi.org/10.1016/j.ttbdis.2010.10.007
- Erra EO, Askling HH, Deshpande A, et al. Cross-protective capacity of tick-borne encephalitis (TBE) vaccines against louping ill virus and tick-borne flaviviruses. J Travel Med. 2011;18:244–252. PMID: 21722237. https://doi.org/10.1111/j.1708-8305.2011.00528.x
- Rendi-Wagner P. Risk and prevention of tick-borne encephalitis in travelers. J Travel Med. 2004;11:307–312. PMID: 15544702. https://doi.org/10.2310/7060.2004.19001
Research Papers
The following PubMed topic searches retrieve current peer-reviewed literature on Tick-Borne Encephalitis.
- Tick-borne encephalitis TBEV flavivirus
- Tick-borne encephalitis vaccine efficacy
- TBEV neuropathology encephalitis treatment
- Tick-borne encephalitis epidemiology Europe
- Tick-borne encephalitis biphasic fever diagnosis
- TBEV Far Eastern subtype Russian spring summer encephalitis
- Tick-borne encephalitis cerebellar ataxia flaccid paralysis
- TBEV Ixodes ricinus transmission
- Tick-borne encephalitis raw milk alimentary transmission
- TBEV immunoglobulin post-exposure prophylaxis
- Tick-borne encephalitis Powassan virus flavivirus
- Tick-borne encephalitis post-encephalitic syndrome sequelae
Connections
- Infectious Disease
- Lyme Disease
- Powassan Virus
- West Nile Virus
- Dengue Fever
- Rocky Mountain Spotted Fever
- Ehrlichiosis
- Meningitis
- Encephalitis — TBE is one of the few vaccine-preventable encephalitides; the general page covers all causes of brain inflammation.
- Viral Hemorrhagic Fevers
- Malaria
- Yellow Fever
- Zika Virus