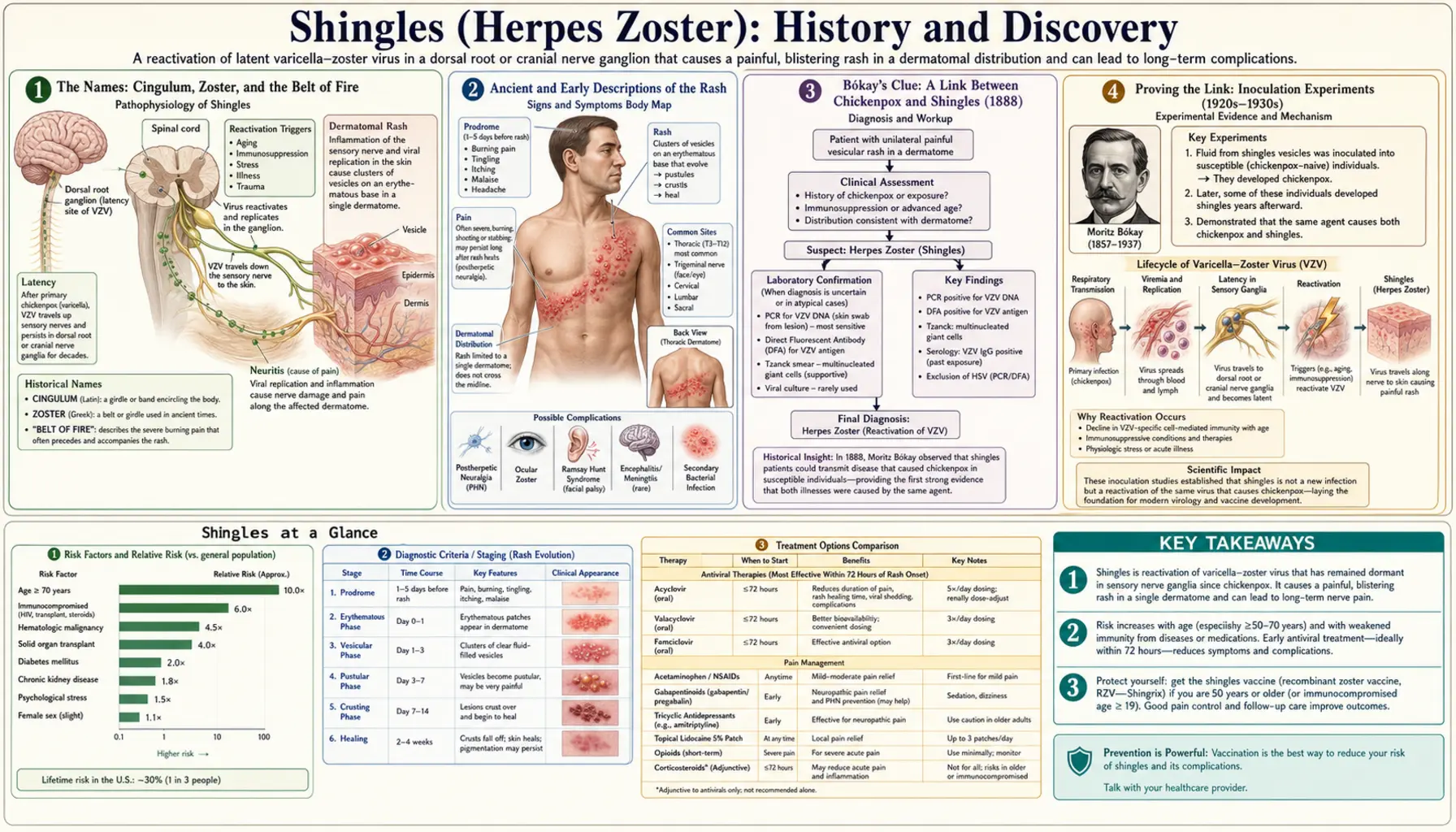
Shingles (Herpes Zoster): History and Discovery
The story of shingles is really two stories that took nearly two thousand years to join together. For most of recorded history, the painful band of blisters that wraps around one side of the body was named for its shape — the English word shingles comes from the Latin cingulum, a girdle or belt, while the medical name herpes zoster joins the Greek herpein, “to creep,” to zōstēr, again a girdle. The great discovery came much later: that shingles and childhood chickenpox are not separate diseases at all but two faces of a single virus, the varicella-zoster virus (VZV). The first clue was an epidemiological one, noticed by the Hungarian pediatrician János von Bókay around 1888; the mechanism — lifelong latency in the nerves and reactivation decades later — was proposed by R. Edgar Hope-Simpson in 1965 and finally confirmed by laboratory virology in the twentieth century. This page traces that arc, from a name on a rash to a vaccine that can prevent it.
Table of Contents
- The Names: Cingulum, Zoster, and the Belt of Fire
- Ancient and Early Descriptions of the Rash
- Bókay’s Clue: A Link Between Chickenpox and Shingles (1888)
- Proving the Link: Inoculation Experiments (1920s–1930s)
- Weller Grows the Virus: One Agent, Two Diseases (1950s)
- Hope-Simpson and the Latency Hypothesis (1965)
- Confirming Latency in the Nerve Ganglia
- From Takahashi’s Vaccine to Shingrix
- Postherpetic Neuralgia: The Complication That Drove the Search
- Research Papers and References
- Connections
- Featured Videos
The Names: Cingulum, Zoster, and the Belt of Fire
Both names that English speakers use for this disease describe the same striking feature: a rash that runs in a band along one side of the trunk, as if a belt had been drawn across the skin. The everyday word shingles descends, by way of Medieval Latin cingulus, from the classical Latin cingulum — a girdle or belt — from the verb cingere, “to gird” or “to encircle.” The name was applied precisely because the inflammation so often extends around the waist or flank like a girdle. (The roofing “shingle” is an unrelated word; the coincidence is purely English.)
The formal medical term herpes zoster reaches the same image through Greek. Herpes comes from herpein, “to creep,” the root shared by the whole family of herpesviruses and a nod to the way these infections creep along and recur. Zoster is the Greek zōstēr, a warrior’s belt or girdle — once more, the band-like rash. So “herpes zoster” means, almost literally, “the creeping girdle.” The virus’s own name, varicella-zoster, then pairs the Latin varicella (“little pox,” for chickenpox) with the Greek zoster, embedding both diseases in a single label once they were known to share a cause.
This shared imagery survives in folk names across Europe, where shingles has long been called something like a “belt of fire” or “ring of fire” — in modern Spanish it is culebrilla (“little snake”) and in French zona, itself from zoster. The vocabulary, in other words, was settled long before anyone understood what the disease actually was. For centuries the name pointed only at the shape on the skin; the cause lay hidden for nearly two more millennia.
Ancient and Early Descriptions of the Rash
A painful, blistering, band-like eruption is hard to miss, and physicians described something resembling shingles from antiquity onward. Greek and Roman medical writers recorded creeping, encircling skin lesions, and the term zoster was used in the classical world for a girdling rash. For accessibility these ancient observations are named here as historical descriptions rather than as modern clinical citations; it is genuinely difficult to know across two thousand years which descriptions correspond to herpes zoster as we define it today and which to other blistering conditions such as erysipelas or impetigo.
What the historical record shows clearly is a long-standing recognition that this rash was distinctive, painful, often confined to one side, and prone to leaving lasting discomfort. Pre-modern medicine, lacking any concept of viruses, could classify shingles only by its appearance, and it was generally treated as a disorder of the skin and the “humors,” with topical remedies and the band-like distribution noted as its defining sign. The persistent association with the girdle shape is why the Latin and Greek belt-words attached so firmly to it.
Crucially, throughout this long period chickenpox and shingles were regarded as entirely separate illnesses — one a mild rash of childhood, the other a painful affliction more common in older adults. There was no reason, on appearance alone, to connect a child’s widespread itchy spots with an adult’s searing one-sided band. The idea that the same agent could cause both would have seemed counterintuitive, and it took a careful clinical observer working in the late nineteenth century to notice the thread that tied them together.
Bókay’s Clue: A Link Between Chickenpox and Shingles (1888)
The pivotal observation came from János von Bókay (also written James or Johann von Bókay), a Hungarian pediatrician working in Budapest. Around 1888 — and revisited in his later writings, including work published in 1909 — Bókay noticed a pattern that did not fit the prevailing view of two unrelated diseases: susceptible children who had never had chickenpox sometimes came down with it a couple of weeks after close household contact with an adult who had shingles. In other words, exposure to a case of herpes zoster could seemingly trigger an outbreak of varicella in children who caught it from that person.
This was a profound and counterintuitive clue. If chickenpox could be “caught” from a case of shingles, then the two diseases must share something fundamental — most plausibly, the same infectious agent. Bókay’s contribution was epidemiological and observational rather than experimental: he saw a recurring real-world link and drew the cautious, correct inference that varicella and herpes zoster were related. He did not, and at the time could not, identify a virus or prove the mechanism; viruses themselves were only beginning to be conceived of as filterable agents distinct from bacteria.
It is worth being precise about what Bókay did and did not establish, because accuracy matters here. He proposed a relationship on the basis of contact patterns; he did not isolate VZV (which would have been impossible with the tools of his day) and he did not describe latency or reactivation. His clinical insight set the agenda for the next seventy years of investigation, but the proof would come from later experiments and, ultimately, from the laboratory. Bókay’s 1888 observation is best remembered as the first solid evidence pointing toward a single cause behind two very different-looking diseases.
Proving the Link: Inoculation Experiments (1920s–1930s)
Bókay’s clue invited a direct test, and in the decades that followed, several investigators set out to confirm experimentally that the fluid from shingles blisters could cause chickenpox. In the early 1920s, the Austrian physician Karl Kundratitz reported that inoculating susceptible children with vesicle fluid taken from patients with herpes zoster produced varicella-like illness. Work along similar lines was extended in the 1930s by investigators including Bruusgaard, who likewise found that material from zoster lesions could transmit chickenpox to non-immune individuals.
These experiments — carried out in an era with very different research ethics than today’s, and which would not be permissible by modern standards — provided strong support for Bókay’s hypothesis. They demonstrated that whatever infectious agent sat inside a shingles blister was capable of producing chickenpox in someone who had never had it. The clinical link Bókay had merely observed in households was now reproduced deliberately, strengthening the case that one agent underlay both diseases.
Still, a gap remained. Transmission experiments could show that the two diseases shared an agent without isolating that agent or pinning down its identity at the level of the virus particle itself. Demonstrating that the very same virus — not merely a similar one — caused both varicella and herpes zoster required the ability to grow the virus in the laboratory and compare strains directly. That capability did not arrive until the middle of the twentieth century, with the advent of practical cell culture.
Weller Grows the Virus: One Agent, Two Diseases (1950s)
The decisive laboratory work was done by the American virologist Thomas Huckle Weller. Weller first succeeded in propagating the varicella-zoster virus in tissue culture in 1953, isolating the agent from cases of both chickenpox and shingles. He and his colleagues then characterized it in detail in a landmark 1958 paper in the Journal of Experimental Medicine, “The Etiologic Agents of Varicella and Herpes Zoster,” which reported that the virus strains recovered from patients with varicella and from patients with herpes zoster could not be distinguished by their behavior in culture.
This was the missing proof, supplied at the level of the virus itself. By growing the agent from both diseases and showing the strains were indistinguishable, Weller’s work established that chickenpox and shingles are caused by one and the same virus — vindicating, in the laboratory, the link Bókay had inferred from a Budapest household sixty-five years earlier. It is the reason the virus carries a hyphenated name honoring both diseases: varicella-zoster virus.
A point of accuracy worth flagging: Thomas Weller shared the 1954 Nobel Prize in Physiology or Medicine — with John Enders and Frederick Robbins — for cultivating poliovirus in non-neural tissue culture, not for his VZV work. The cell-culture techniques recognized by that prize, however, were exactly what made the varicella-zoster isolation possible, and Weller himself regarded his VZV studies as among his proudest achievements. The Nobel and the VZV discovery are thus closely related in method but are distinct accomplishments, and this page is careful not to conflate them.
Hope-Simpson and the Latency Hypothesis (1965)
Knowing that one virus caused both diseases still left a deep puzzle: how could a virus that gave a child chickenpox come roaring back as a one-sided rash in the same person decades later? The most influential answer was proposed by R. Edgar Hope-Simpson, an English general practitioner who spent years meticulously recording every case of zoster in his rural Gloucestershire practice. In his classic 1965 paper, “The Nature of Herpes Zoster: A Long-Term Study and a New Hypothesis” (Proceedings of the Royal Society of Medicine), he set out the model that still anchors our understanding.
Hope-Simpson proposed that after a bout of chickenpox the virus does not leave the body but retreats into the sensory nerve cells — the dorsal root ganglia alongside the spinal cord — where it lies latent, silent and dormant, often for the rest of a person’s life. Years or decades later, when the immune system’s grip on the virus weakens, the latent virus can reactivate, travel back down a single sensory nerve, and erupt as shingles in the strip of skin (the dermatome) that nerve supplies. This elegantly explained both the one-sided, band-like rash and why shingles tends to strike older adults and people whose immunity is reduced.
From his careful records, Hope-Simpson also noticed that the dermatomes most often hit by shingles matched the regions where chickenpox lesions had been densest, and he reasoned that immunity to the virus could be topped up by exposure to circulating chickenpox — ideas that remain debated and studied today. It is important to be clear that in 1965 this was advanced as a hypothesis, an inference from epidemiology and clinical pattern, not yet a demonstrated molecular fact. Its power was that it was both testable and, ultimately, largely correct.
Confirming Latency in the Nerve Ganglia
Hope-Simpson’s latency-and-reactivation model was a hypothesis when he wrote it, and turning it into established fact required showing that the virus really does hide inside the nerve ganglia between episodes. Through the later twentieth century, advances in virology and molecular biology made this possible. Investigators were eventually able to detect varicella-zoster viral DNA in human sensory ganglia — in the trigeminal and dorsal root ganglia — obtained from people who had had chickenpox but were not currently suffering shingles, demonstrating that the virus persists silently in exactly the location Hope-Simpson had predicted.
These findings confirmed the core of the hypothesis: the virus establishes lifelong latency in the neurons of the sensory ganglia after primary infection, and shingles is the result of its reactivation along a single nerve. The discovery also clarified why anything that weakens cell-mediated immunity — advancing age, certain illnesses, immunosuppressive medication — raises the risk of an outbreak, since it is that arm of the immune system that keeps the latent virus in check. The mechanism Hope-Simpson sketched from a country doctor’s case ledger was now visible in the molecular record.
This convergence — a clinical observation (Bókay), confirmatory transmission experiments (Kundratitz, Bruusgaard), laboratory isolation of a single shared virus (Weller), an epidemiological hypothesis of latency and reactivation (Hope-Simpson), and finally molecular confirmation of viral DNA in the ganglia — is a textbook example of how a disease comes to be understood in layers, each generation building on the last. By the close of the twentieth century, shingles had been transformed from a mysterious girdle-shaped rash into one of the best-understood reactivating viral infections in medicine.
From Takahashi’s Vaccine to Shingrix
Understanding the virus opened the door to preventing it. The foundational step was the development of a live attenuated varicella vaccine by the Japanese virologist Michiaki Takahashi. Takahashi isolated the virus from the blister fluid of a child with chickenpox — the boy’s family name, Oka, gave the strain its enduring name — and weakened it through repeated passage in cell cultures. His results were reported in 1974, and the Oka strain became the basis of the chickenpox vaccines used worldwide, the same attenuated virus that underlies the later shingles vaccines as well.
Because shingles is a reactivation of the very virus the Oka vaccine targets, a logical next step was a vaccine aimed at older adults to boost waning immunity and head off reactivation. Zostavax, made by Merck, was a high-dose live attenuated zoster vaccine; the U.S. Food and Drug Administration approved it in May 2006 for adults aged 60 and over (later extended to those 50 and over). It reduced the risk of shingles and of its painful aftermath, though its protection was only partial and waned with time, and being a live vaccine it was not suitable for people with weakened immune systems.
The current standard arrived with Shingrix, a recombinant subunit zoster vaccine from GlaxoSmithKline, FDA-approved in October 2017. Rather than a live virus, Shingrix combines a single VZV surface protein (glycoprotein E) with a potent adjuvant, producing markedly higher and more durable protection against shingles and postherpetic neuralgia — and, because it contains no live virus, it can be given to many people for whom Zostavax was unsafe. Shingrix became the preferred shingles vaccine, and Zostavax was withdrawn from the U.S. market in 2020. In two human generations, shingles had gone from an unexplained rash to a largely preventable one.
Postherpetic Neuralgia: The Complication That Drove the Search
Much of the long medical interest in shingles — and much of the urgency behind vaccinating against it — comes not from the rash itself but from its most feared complication, postherpetic neuralgia (PHN). PHN is persistent nerve pain that lingers in the affected area for months or even years after the blisters have healed, the consequence of damage and ongoing irritation to the sensory nerve through which the virus reactivated. It can be severe, burning, and stubbornly resistant to treatment, and it becomes markedly more common with advancing age.
PHN explains why shingles has always been regarded as more than a passing skin disease and why the latency model matters so directly to patients: because shingles travels along a single sensory nerve, the lasting pain follows that same nerve’s territory. The risk of PHN rising sharply in older adults is precisely the reason the zoster vaccines were targeted at exactly that group, and the fact that Shingrix substantially reduces PHN — not just the rash — is central to why it is recommended. Other recognized complications, including involvement of the eye in ophthalmic zoster, similarly trace back to which nerve the virus reactivates along.
Seen as a whole, the history of shingles is a chain of insights that turned a frightening, poorly understood affliction into a disease we can name precisely, explain mechanistically, and increasingly prevent. From the girdle-words of antiquity, through Bókay’s 1888 clue and Weller’s isolation of a single shared virus, to Hope-Simpson’s latency hypothesis and the vaccines that followed, each step reduced human suffering — with the prevention of postherpetic neuralgia standing as the clearest measure of how far that understanding has come. For the clinical picture, risk factors, and current treatment, see the main Shingles page.
Research Papers and References
The references below combine the key primary papers in the discovery of varicella-zoster virus and its latency with curated PubMed topic-search links into the historical and clinical literature. Where a definitive primary paper is cited, a real DOI or PMID is given; broader historical themes link to PubMed topic searches. Each external link opens in a new tab.
- Hope-Simpson RE. The Nature of Herpes Zoster: A Long-Term Study and a New Hypothesis. Proceedings of the Royal Society of Medicine. 1965;58(1):9-20. — doi:10.1177/003591576505800106 (PMID: 14267505)
- Weller TH, Witton HM, Bell EJ. The Etiologic Agents of Varicella and Herpes Zoster: Isolation, Propagation, and Cultural Characteristics In Vitro. Journal of Experimental Medicine. 1958;108(6):843-868. — doi:10.1084/jem.108.6.843 (PMID: 13598816)
- Gilden DH, Kleinschmidt-DeMasters BK, LaGuardia JJ, et al. Latent varicella-zoster viral DNA in human trigeminal and thoracic ganglia. New England Journal of Medicine. 1990;323(10):627-631. — doi:10.1056/NEJM199009063231002 (PMID: 2166911)
- Takahashi M, Otsuka T, Okuno Y, Asano Y, Yazaki T. Live vaccine used to prevent the spread of varicella in children in hospital. The Lancet. 1974;304(7892):1288-1290. — doi:10.1016/S0140-6736(74)90144-5 (PMID: 4139526)
- Weller TH. Varicella and herpes zoster: a perspective and overview. Journal of Infectious Diseases. 1992;166(Suppl 1):S1-S6. — PubMed: Weller perspective on varicella and herpes zoster
- János von Bókay and the historical link between varicella and herpes zoster — PubMed: Bókay, varicella and herpes zoster history
- Kundratitz / Bruusgaard inoculation experiments transmitting varicella from zoster vesicle fluid — PubMed: zoster vesicle-fluid inoculation history
- History of varicella-zoster virus — discovery, isolation, and milestones — PubMed: history of varicella-zoster virus
- Varicella-zoster virus latency in sensory ganglia — mechanism and reactivation — PubMed: VZV latency and reactivation
- The Oka strain and development of the live attenuated varicella vaccine — PubMed: Oka strain varicella vaccine development
- Zoster vaccine (Zostavax) live attenuated — efficacy and history — PubMed: live zoster vaccine (Zostavax)
- Recombinant subunit zoster vaccine (Shingrix) — glycoprotein E with adjuvant — PubMed: recombinant zoster vaccine (Shingrix)
- Postherpetic neuralgia — pathophysiology, risk factors, and prevention — PubMed: postherpetic neuralgia
- Etymology and terminology of herpes zoster (shingles) — PubMed: herpes zoster etymology and terminology
External Authoritative Resources
- CDC — Shingles (Herpes Zoster)
- StatPearls (NCBI Bookshelf) — Varicella-Zoster Virus
- PubMed — Herpes zoster and VZV history
Connections
- Infectious Disease
- Shingles (Herpes Zoster)
- All Conditions
- Peripheral Neuropathy
- Chronic Pain
- Central Sensitization and Nociplastic Pain
- Complex Regional Pain Syndrome
- Meningitis