Mucormycosis
- Overview
- Epidemiology
- Pathophysiology
- Risk Factors
- Clinical Forms
- Rhinocerebral Mucormycosis
- Pulmonary Mucormycosis
- Diagnosis
- Treatment
- Complications
- Prognosis
- Prevention
- References
Overview
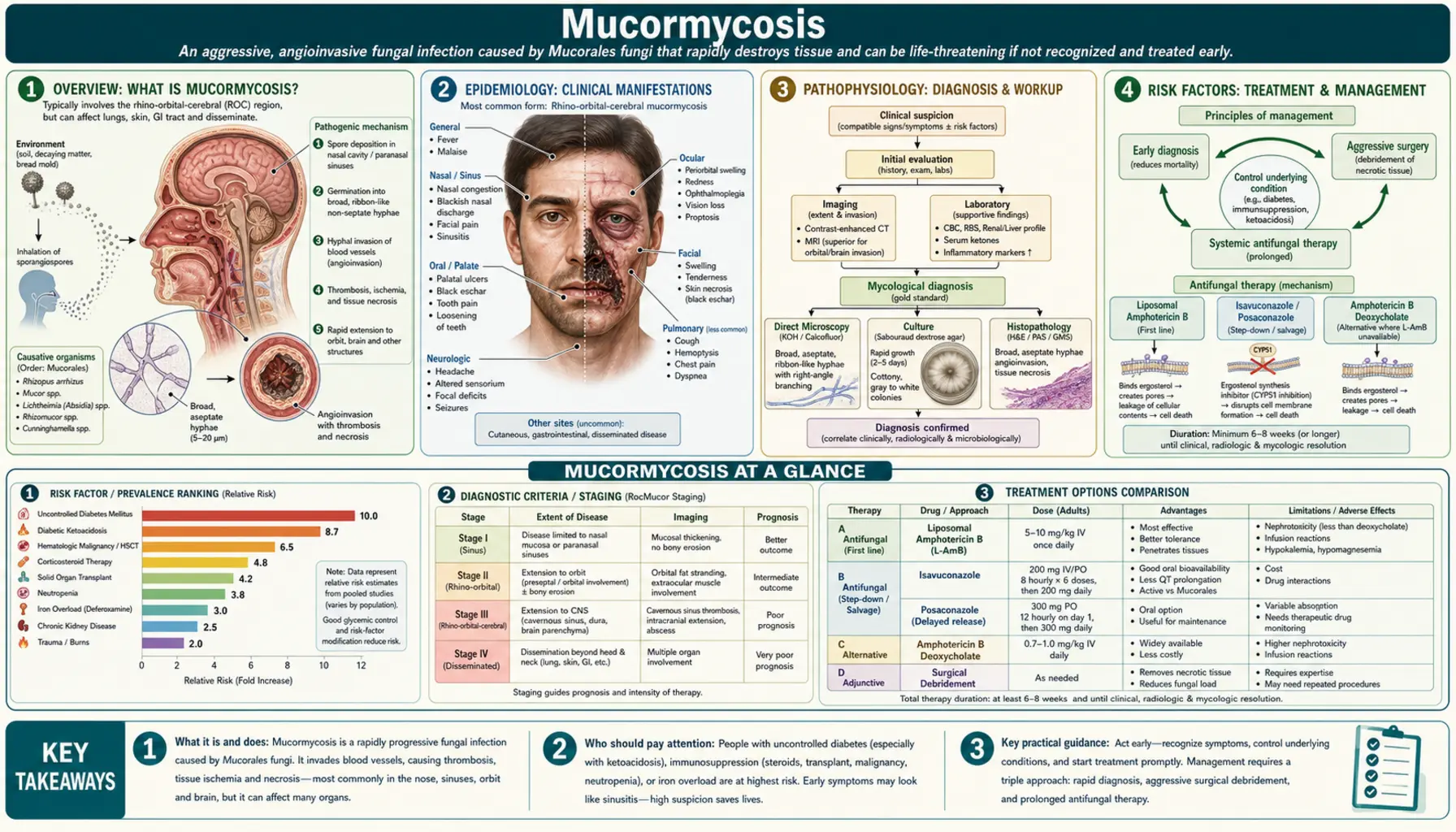
Mucormycosis (formerly zygomycosis) is an angioinvasive mold infection caused by fungi of the order Mucorales, class Zygomycetes. The key causative genera include Rhizopus (the most common, with R. arrhizus — also called R. oryzae — being the predominant species), Mucor, Lichtheimia (formerly Absidia), and Cunninghamella, which is particularly virulent in profoundly immunocompromised hosts. These ubiquitous environmental molds are found in soil, decaying organic matter, and in the air everywhere on earth; healthy individuals inhale spores constantly without becoming infected, because intact immunity clears them efficiently.
Three critical hallmarks define mucormycosis and explain its clinical behavior. First is rapid progression: the infection can spread from the sinuses to the brain in as little as 24 to 48 hours, making it one of the fastest-moving life-threatening infections in clinical medicine. Second is angioinvasion: the hyphae actively penetrate blood vessel walls, causing thrombosis and tissue infarction. This explains the pathognomonic black necrotic eschar, but also something clinically critical — ischemic tissue receives no blood supply, meaning IV antifungals cannot penetrate to the site of infection, and surgery is therefore always required. Third is the principle that the infection is reversed by correcting the underlying risk factor: normalizing blood glucose and stopping corticosteroids are as important as any antifungal drug.
Mucormycosis is widely regarded as one of the most feared fungal infections in medicine. Mortality ranges from 40 to 80 percent even with aggressive treatment combining surgery, high-dose antifungal therapy, and reversal of the predisposing condition. The infection gained renewed global attention during the 2021 COVID-associated mucormycosis (CAM) outbreak in India, which illustrated how rapidly a confluence of risk factors can amplify a rare disease into a public health emergency.
Epidemiology
Mucormycosis is rare but rising in incidence globally. Estimates suggest approximately 8,000 to 10,000 cases per year worldwide, with rising numbers closely linked to expanding diabetic and immunosuppressed populations. In the United States, the incidence is approximately 1.7 cases per million people per year. In continental Europe, hematologic malignancy and hematopoietic stem cell transplantation (HSCT) account for the dominant risk factor demographics, reflecting those regions' patterns of diabetes management and transplant medicine volumes.
The 2021 COVID-associated mucormycosis outbreak in India stands as the defining epidemiologic event of modern mucormycology. An estimated 40,000 or more cases occurred in a matter of months, representing a convergence of four concurrent risk amplifiers: COVID-19 itself (causing immune dysregulation, lymphopenia, and endothelial inflammation), corticosteroid treatment for severe COVID (dexamethasone induces hyperglycemia and impairs phagocyte function simultaneously), pre-existing poorly controlled or undiagnosed diabetes at extremely high national prevalence, and possible contamination of supplemental oxygen humidification systems. India's disproportionate burden reflects not only diabetes prevalence but also delayed diagnosis in resource-limited settings, where patients present later in the disease course with more extensive tissue destruction.
Case fatality rates vary significantly by site and extent of disease. Rhinocerebral mucormycosis (the most common form in diabetic patients) carries 40 to 60 percent mortality with aggressive combined treatment and can approach 80 to 100 percent with intracranial extension. Pulmonary mucormycosis, predominantly affecting hematologic malignancy patients, carries 65 to 90 percent mortality. Disseminated mucormycosis, defined as involvement of two or more non-contiguous sites, approaches 100 percent mortality even with maximal therapy.
Pathophysiology
Infection begins when sporangiospores are inhaled into the airways (or directly inoculated into wounds or GI mucosa in cutaneous and gastrointestinal forms). In immunocompetent individuals, alveolar macrophages and recruited neutrophils kill spores efficiently through oxidative burst mechanisms and phagolysosmal acidification. Two principal arms of innate immunity — neutrophil-mediated killing and macrophage-mediated clearance — must both be impaired before mucormycosis can establish itself, which is why the infection almost exclusively affects patients with specific immunologic vulnerabilities.
Neutropenia and neutrophil dysfunction are the primary vulnerability in hematologic malignancy patients. Neutrophils are the central defense against Mucorales; their near-absence in profound neutropenia essentially removes the host's ability to contain germinating spores. Corticosteroids impair both macrophage phagosomal acidification and neutrophil chemotaxis and oxidative burst, explaining their importance as a risk factor even in otherwise immunologically intact patients.
Acidosis, hyperglycemia, and iron availability form the metabolic axis that drives diabetes-associated mucormycosis, particularly in diabetic ketoacidosis. In acidic environments (pH below 7.4), iron is released from transferrin, leaving free iron available in the circulation. Mucorales are exquisitely dependent on iron for growth — they express high-affinity iron acquisition systems including dedicated siderophores and direct reductive iron assimilation. Free iron in the acidotic, hyperglycemic environment of DKA essentially provides a growth medium for the fungus. This mechanism also explains one of clinical medicine's most important drug contraindications: deferoxamine, the older iron chelator used in hemochromatosis and transfusional iron overload, forms a deferoxamine-iron complex that is taken up directly by the Mucorales siderophore system and used as an iron source. Deferoxamine treatment in at-risk patients does not protect against mucormycosis — it actively promotes it. This is an absolute contraindication.
Angioinvasion and tissue infarction are the defining pathologic events once infection is established. Mucorales hyphae express surface proteins (CotH spore coat proteins, for example) that interact with host endothelial cell receptors, facilitating active penetration of vessel walls. Once hyphae invade the vascular endothelium, they trigger thrombosis, occluding blood flow to downstream tissue. The resulting ischemic infarction produces the characteristic black necrotic eschar — tissue that has literally died from lack of blood supply. This creates two compounding clinical problems: the necrotic tissue supports ongoing fungal growth as a nutrient-rich anaerobic substrate, and the absence of vascularity means systemic antifungal drugs administered intravenously cannot reach the infected site. No amount of amphotericin B can cure a patient if the infected, necrotic tissue is not surgically removed.
Hyphae morphology on microscopy is distinctive and important for diagnosis: broad (6 to 16 micrometers in diameter), aseptate or pauci-septate (essentially ribbon-like, with rare cross-walls), and branching at approximately 90-degree right angles. This sharply contrasts with Aspergillus species, which produce narrow (2 to 4 micrometers), regularly septate hyphae branching at 45-degree angles. The distinction matters because these two molds cause clinically similar syndromes but require different antifungal treatment — and critically, the primary first-line treatment for invasive aspergillosis (voriconazole) has no activity against Mucorales.
Risk Factors
Diabetes mellitus and diabetic ketoacidosis represent the single most common risk factor for rhinocerebral mucormycosis, accounting for 70 to 80 percent of rhinocerebral cases. Even well-controlled diabetes increases susceptibility through subtle defects in neutrophil chemotaxis and phagocytic function; DKA dramatically amplifies risk through acidosis-mediated iron liberation, hyperglycemia-impaired immune cell function, and the concurrent endocrine stress response. In many parts of the world, rhinocerebral mucormycosis presenting in a patient with undiagnosed or poorly controlled diabetes and DKA is the most common clinical scenario.
Hematologic malignancy and prolonged neutropenia are the dominant risk factors in developed countries' epidemiology. Acute myeloid leukemia, myelodysplastic syndrome, and lymphoma patients undergoing induction chemotherapy develop neutrophil counts near zero for weeks to months. Prolonged neutropenia (absolute neutrophil count below 500 cells/mm³ for more than two weeks) is the critical determinant — this is when pulmonary mucormycosis risk peaks.
Hematopoietic stem cell transplantation, especially allogeneic HSCT, creates multiple converging risk windows: conditioning-regimen neutropenia, graft-versus-host disease (GVHD) requiring high-dose corticosteroid treatment, prolonged immunosuppression with calcineurin inhibitors, and mucositis breaching mucosal barriers. HSCT patients receiving voriconazole prophylaxis for aspergillosis prevention may face a particularly dangerous scenario — breakthrough mucormycosis in patients "protected" by azole prophylaxis.
Solid organ transplantation confers sustained risk from calcineurin inhibitors (tacrolimus, cyclosporine), which impair T-cell and NK-cell function. Kidney and liver transplant recipients have the highest mucormycosis incidence among solid organ transplant types. Early post-transplant period carries the highest risk.
Corticosteroid therapy, whether for autoimmune disease, organ transplantation, or acute illness including COVID-19, impairs multiple arms of antifungal immunity simultaneously. The 2021 India outbreak demonstrated that dexamethasone at doses used for severe COVID — entirely appropriate for preventing death from inflammatory lung injury — can create sufficient immunosuppression to permit mucormycosis in patients with pre-existing diabetes.
Deferoxamine use in patients with iron overload states (hereditary hemochromatosis, thalassemia major, transfusional siderosis from repeated red cell transfusions) represents an absolute contraindication in immunosuppressed or diabetic patients. The mechanism is direct: deferoxamine chelates iron into a complex that Mucorales species take up via their siderophore systems and metabolize as a direct iron source. This contraindication is often underappreciated.
Trauma, burns, and natural disasters can inoculate Mucorales spores directly into wounds or through contaminated dressings, producing cutaneous or wound mucormycosis without any systemic immunosuppression. Mass casualty events — the 2004 Indian Ocean tsunami, military combat injuries — have produced clusters of cutaneous mucormycosis in previously healthy individuals.
COVID-19 independently creates risk through coagulopathy, endothelial inflammation, lymphopenia, and possibly direct impairment of alveolar macrophage function. Even without corticosteroid treatment, severe COVID-19 patients have developed mucormycosis, though the risk is dramatically amplified by concurrent dexamethasone use.
Clinical Forms
Mucormycosis presents in six major clinical syndromes, each reflecting the anatomic site of initial invasion and the underlying host risk factor that permitted it. Rhinocerebral mucormycosis is the most widely recognized and highest-profile form, primarily occurring in diabetic patients with DKA, and is described in detail in its own section. Pulmonary mucormycosis is the second most common form, predominantly affecting hematologic malignancy and HSCT patients, and is also addressed separately.
Cutaneous mucormycosis results from direct traumatic inoculation at a wound, surgical site, or IV catheter site. It begins as a localized area of cellulitis that rapidly develops central necrosis and a black eschar as angioinvasion destroys local vascularity. Without early surgical debridement, it can progress to underlying fascia, muscle, and bone. In immunocompromised patients, cutaneous mucormycosis can seed the bloodstream and become disseminated.
Gastrointestinal mucormycosis is the rarest form in adults and is primarily described in premature neonates and severely malnourished individuals. Spores are ingested rather than inhaled; they invade the GI mucosa, most commonly the stomach, colon, or ileum. Bowel necrosis, perforation, and peritonitis can develop rapidly, and the mortality is extremely high. In neonates, it can present similarly to necrotizing enterocolitis.
Renal mucormycosis is rare and is thought to arise from hematogenous seeding. Patients present with fever, flank pain, and renal impairment. It is reported predominantly in injection drug users and renal transplant recipients.
Disseminated mucormycosis represents bloodstream invasion with simultaneous multi-organ involvement — typically two or more non-contiguous sites. It carries the worst prognosis of all forms, with mortality approaching 100 percent even with maximal therapy. It is most common in profoundly neutropenic patients and those with disseminated infection from another primary site that was not treated surgically.
Rhinocerebral Mucormycosis
Rhinocerebral mucormycosis is the classic clinical presentation that most clinicians and medical students learn first, and for good reason — it illustrates every important principle of the disease and occurs in the most recognizable setting: a patient with diabetes presenting in DKA with fever and sinus pain that is "not responding to antibiotics." It is a surgical and medical emergency with a narrow window between diagnosis and death.
The infection begins in the paranasal sinuses, most commonly the maxillary or ethmoid sinuses, as inhaled spores germinate into hyphae in the hyperglycemic, acidotic tissue environment. Early symptoms mimic bacterial sinusitis: facial pain and pressure, nasal congestion, purulent nasal discharge, fever, and headache. This is the critical window for diagnosis — before tissue infarction has made surgery more radical and outcomes worse. However, early rhinocerebral mucormycosis is almost always misdiagnosed as bacterial sinusitis or orbital cellulitis in its first 24 to 48 hours.
The first warning signs of angioinvasion are the appearance of bloody or black nasal discharge and the onset of facial hypoesthesia or anesthesia as nerve infarction accompanies vascular occlusion. The pathognomonic finding is the black necrotic eschar on the hard palate, nasal turbinates, or septum — a dark, ulcerated, non-bleeding lesion representing ischemic tissue death. This finding should prompt immediate surgical and infectious disease consultation and empiric antifungal treatment without waiting for culture confirmation.
Orbital extension occurs as infection spreads through the ethmoid sinus and orbital floor. It produces periorbital edema and erythema resembling orbital cellulitis, but rapidly progresses to proptosis (forward displacement of the globe), chemosis (conjunctival edema), ptosis, ophthalmoplegia (inability to move the eye), and diplopia as the orbital apex becomes involved. Orbital apex syndrome — the combination of visual loss, ophthalmoplegia, and ptosis — indicates cranial nerve III, IV, V, and VI involvement and signals imminent intracranial spread. The decision to perform orbital exenteration (surgical removal of the eye and orbital contents) is one of the most difficult in medicine; it is often the difference between survival and death.
Cavernous sinus thrombosis occurs as hyphae spread posteriorly from the orbital apex and sphenoid sinus into the cavernous sinus, causing septic thrombosis with high fever, rigors, and severe headache. From the cavernous sinus, hyphae can invade the internal carotid artery, causing stroke, or spread directly into brain parenchyma, causing cerebral infarction, abscess, and ultimately death.
Imaging is essential for staging extent of disease. CT of the sinuses with bone windows reveals the extent of sinusitis and, critically, bone erosion — an ominous sign of aggressive invasion. MRI with gadolinium is superior for assessing soft tissue extension into the orbit, cavernous sinus, and brain parenchyma. The "black turbinate sign" on MRI (loss of normal T1 signal within the turbinates, reflecting infarction) has been proposed as an early radiologic indicator. MRI also identifies cavernous sinus thrombosis and cerebral infarction that CT may miss.
Pulmonary Mucormycosis
Pulmonary mucormycosis is the dominant clinical form in patients with hematologic malignancies and HSCT recipients. It arises from inhalation of sporangiospores directly into the lung parenchyma, where prolonged neutropenia eliminates the primary cellular defense against germinating fungi. Unlike rhinocerebral mucormycosis, pulmonary disease lacks a single pathognomonic clinical finding, making it highly susceptible to diagnostic delay — especially because it occurs in the same clinical context as invasive pulmonary aspergillosis, which is far more common and has overlapping radiologic features.
Symptoms are nonspecific and include persistent fever despite broad-spectrum antibacterials, pleuritic chest pain, dry or productive cough, and hemoptysis. Hemoptysis can be massive when large pulmonary vessels are invaded and thrombosed; fatal hemorrhage can occur. Physical examination and basic laboratory tests rarely distinguish pulmonary mucormycosis from other opportunistic infections in neutropenic patients.
CT chest imaging provides the most useful diagnostic information. The reverse halo sign (also called the atoll sign) — central consolidation surrounded by a rim of peripheral ground-glass opacity — is the most characteristic CT finding, with a specificity for angioinvasive fungal infection in the neutropenic patient that approaches 90 percent in some series, though sensitivity is only around 20 to 25 percent. Multiple pulmonary nodules, wedge-shaped infarcts, pleural effusion, and the air crescent sign (a crescent of air within a consolidating nodule) are also reported. Importantly, CT findings in pulmonary mucormycosis overlap substantially with invasive pulmonary aspergillosis, and the two cannot be reliably distinguished by imaging alone.
This distinction is clinically critical because voriconazole — the first-line treatment for invasive aspergillosis — has no activity against Mucorales. Azole antifungals work by inhibiting the fungal enzyme CYP51A (lanosterol 14-alpha-demethylase) in the ergosterol biosynthesis pathway. Mucorales lack a susceptible CYP51A isoform and additionally express efflux pumps that reduce intracellular azole concentrations. Voriconazole therefore does not kill Mucorales at clinically achievable concentrations. A neutropenic patient with pulmonary infiltrates who is "failing voriconazole" — worsening clinically or radiologically despite 72 to 96 hours of treatment — must be urgently evaluated for mucormycosis as a breakthrough or alternate diagnosis. Standard diagnostic tests that help distinguish the two infections include serum beta-D-glucan (negative in mucormycosis — Mucorales cell walls do not release detectable beta-D-glucan; positive in aspergillosis and candidiasis) and serum galactomannan (negative in mucormycosis; positive in aspergillosis). These negative predictive values are clinically actionable.
Bronchoscopy with bronchoalveolar lavage (BAL) is the standard diagnostic procedure for pulmonary cases where tissue cannot be obtained surgically. BAL samples should be sent for both direct microscopy (KOH preparation to identify broad aseptate hyphae) and fungal culture, though culture sensitivity is poor — Mucorales hyphae are fragile and are frequently dead or non-viable in clinical specimens, yielding false-negative cultures even when active infection is present. Surgical lung biopsy provides the highest diagnostic yield but is often precluded by the patient's clinical condition and thrombocytopenia.
Diagnosis
Rapid diagnosis is the cornerstone of survival in mucormycosis. Every 24-hour delay in initiating appropriate treatment increases mortality. The clinical challenge is that definitive diagnosis requires tissue, but collecting tissue requires procedures that carry procedural risk in often-coagulopathic, thrombocytopenic, or critically ill patients. The practical approach is to simultaneously pursue diagnostic workup and initiate empiric treatment in any patient with a compelling clinical syndrome and predisposing risk factor.
Tissue biopsy with histopathology is the gold standard. Culture alone is insufficient and should not be relied upon — culture sensitivity is approximately 50 percent even with active, disseminated infection, because Mucorales hyphae lyse during tissue processing and transport. Histopathology on fresh or formalin-fixed tissue using Grocott-Gomori methenamine silver (GMS) stain and hematoxylin-eosin (H&E) reveals the characteristic broad, aseptate, ribbon-like hyphae branching at right angles. In rhinocerebral disease, biopsy of the black eschar or turbinate tissue can be performed at the bedside with minimal procedural risk. Intraoperative frozen section is valuable — it provides same-day histologic confirmation and guides the surgical team on adequacy of resection margins in real time.
Direct microscopy using potassium hydroxide (KOH) preparation of nasal scrapings, BAL fluid, or wound material provides rapid same-day results without culture delays. KOH dissolves cellular material while leaving fungal cell walls intact, making hyphae visible under light microscopy. This is a fast, inexpensive test that any microbiology laboratory can perform, and a positive result should prompt immediate action.
Imaging is essential for staging extent of disease and surgical planning but cannot replace histologic confirmation. CT sinuses with bone windows (rhinocerebral), MRI brain with gadolinium (intracranial extension), and CT chest (pulmonary disease) all contribute specific information. The specific radiologic features are described under each clinical form section above.
Serum biomarkers: beta-D-glucan is characteristically negative in mucormycosis — this is diagnostically useful because it helps distinguish mucormycosis from aspergillosis (positive) and candidiasis (positive) in the same clinical settings. Galactomannan is also negative. A patient with a neutropenic fever syndrome and negative beta-D-glucan and galactomannan has a higher pre-test probability of mucormycosis than aspergillosis/candidiasis, and this should inform empiric antifungal choice. Mucorales-specific PCR assays are available in some reference laboratories but are not yet standardized or widely deployed.
The clinical diagnosis algorithm for rhinocerebral disease is: any patient presenting with DKA, fever, sinus pain, facial swelling, periorbital changes, and/or a black nasal or palatal lesion should be presumptively diagnosed with rhinocerebral mucormycosis and referred for immediate combined ENT-ophthalmology-infectious diseases evaluation. Do not wait for culture results. Start liposomal amphotericin B and arrange emergent operative debridement.
Treatment
Treatment of mucormycosis requires the simultaneous execution of three interdependent strategies. Pursuing any one in isolation is insufficient; survival depends on all three working together.
1. Surgical debridement — the most important single intervention. All necrotic and infected tissue must be physically removed. The reason is mechanistic, not optional: liposomal amphotericin B and all other systemic antifungals are delivered via the bloodstream. Infarcted, thrombosed tissue has no blood supply. Antifungals cannot penetrate a necrotic eschar. No dose escalation and no drug combination will compensate for leaving infected dead tissue in place. Surgery must be aggressive — surgeons should not hesitate to remove tissue that appears marginally viable. Multiple return-to-operating-room procedures are the norm in rhinocerebral disease; patients may require weekly or more frequent debridements as disease evolves. In rhinocerebral disease with orbital extension, orbital exenteration (surgical removal of the eye, eyelids, and all orbital contents) is sometimes required to achieve adequate resection and prevent intracranial spread. This is among the most disfiguring procedures in surgery and is performed only because the alternative is death; the decision should be made by an experienced team including infectious diseases, ophthalmology, and neurosurgery.
2. Antifungal therapy. Liposomal amphotericin B (LAmB) is the first-line agent. The liposomal formulation is preferred over amphotericin B deoxycholate (conventional AmB) because it achieves higher tissue concentrations (particularly in the CNS), is less nephrotoxic, and allows higher dosing. Recommended doses are 5 to 10 mg/kg/day IV — significantly higher than doses used for aspergillosis or candidiasis, reflecting the need for maximum drug delivery in the face of limited tissue penetration. Infusion-related reactions (fever, rigors, hypotension) can be minimized with premedication. Nephrotoxicity and electrolyte abnormalities (hypokalemia, hypomagnesemia) are the dose-limiting toxicities and require aggressive monitoring and replacement during treatment.
Isavuconazole (oral and IV) received FDA approval for mucormycosis in 2015 based on the VITAL trial and is the preferred oral step-down agent once a patient has improved clinically on LAmB. Its advantages include oral bioavailability (allowing outpatient completion of therapy), a favorable drug interaction profile compared to posaconazole, and avoidance of the renal toxicity associated with prolonged LAmB. Posaconazole (oral suspension or IV) is an alternative for step-down or salvage therapy. The combination of LAmB plus an azole (isavuconazole or posaconazole) is used at many centers for severe disease based on biological rationale and retrospective data, though no randomized trial has proven superiority of combination therapy over LAmB alone. Voriconazole, fluconazole, itraconazole, and echinocandins (caspofungin, micafungin, anidulafungin) have no activity against Mucorales and must not be used.
3. Correction of the underlying condition — essential for cure. Blood glucose must be normalized and DKA reversed. Corticosteroids must be reduced to the minimum dose required for the underlying indication, or discontinued entirely if clinically feasible. In transplant recipients, immunosuppression regimens should be reduced where possible in consultation with the transplant team. Neutrophil recovery from chemotherapy is awaited or accelerated with granulocyte colony-stimulating factors. Deferoxamine must be stopped immediately and permanently. Granulocyte transfusions have been used in profoundly neutropenic patients without evidence of sustained efficacy but remain an option in refractory cases.
Adjunctive approaches include hyperbaric oxygen (HBO), which increases tissue oxygen tension in peri-wound tissue, potentially improving neutrophil killing in borderline-perfused tissue. Evidence is limited to case series, but HBO is offered at centers where it is available for rhinocerebral and cutaneous disease. Deferasirox (not deferoxamine), a newer oral iron chelator, was evaluated in the DEFEAT Mucor trial. The primary endpoint was not met, but subgroup analyses suggested potential benefit in immunocompromised patients. It is occasionally used as adjunctive therapy at experienced centers. Treatment duration is prolonged — typically until complete radiographic resolution and clinical cure, which often requires months of azole step-down therapy.
Complications
Orbital exenteration is both a complication of the disease and a surgical intervention required to prevent intracranial spread. Loss of the eye and orbital contents is among the most visible and psychologically devastating consequences of rhinocerebral mucormycosis. Reconstruction and orbital prosthetics can be considered after infection is controlled, but cure takes absolute priority over cosmesis.
Cavernous sinus thrombosis and cerebral infarction result from intracranial extension of rhinocerebral disease. Stroke-like neurologic deficits — hemiplegia, cranial nerve palsies, aphasia — can be permanent even in survivors. The internal carotid artery is particularly vulnerable as it transits the cavernous sinus; carotid thrombosis produces major hemispheric infarction.
Amphotericin B nephrotoxicity is the dominant pharmacologic complication of treatment. Extended high-dose LAmB therapy causes dose-dependent renal tubular toxicity; serum creatinine, BUN, and electrolytes require daily monitoring during induction therapy. Hypokalemia and hypomagnesemia are nearly universal and require aggressive IV replacement to prevent cardiac arrhythmias. In some patients, nephrotoxicity necessitates dose reduction or transition to azole therapy before mycologic cure is achieved, compromising outcomes.
Disease relapse occurs in a significant proportion of survivors who require ongoing immunosuppression for their underlying condition. Patients with hematologic malignancy returning to chemotherapy, HSCT recipients requiring intensified immunosuppression for GVHD, and transplant recipients on calcineurin inhibitors are all at elevated relapse risk. Long-term secondary prophylaxis with posaconazole or isavuconazole is used at many centers in these settings.
Recurrence with new immunosuppressive episodes can occur months to years after apparent cure when a new immunosuppressive challenge (second transplant, relapsed leukemia, COVID-19 requiring steroids) reactivates residual fungal elements at the site of previous infection. MRI or CT at the previously infected site before starting new immunosuppression is standard practice at expert centers.
Prognosis
Prognosis in mucormycosis is highly variable and determined primarily by four factors: (1) the speed of diagnosis and treatment initiation, (2) the anatomic extent of disease at the time of presentation, (3) the ability to reverse the underlying predisposing condition, and (4) the feasibility of achieving adequate surgical resection.
Among patients with rhinocerebral disease confined to the sinuses without orbital or intracranial extension, aggressive combined treatment (early surgery, LAmB, glucose control) produces survival rates of 40 to 60 percent. With orbital extension, mortality increases to 60 to 80 percent. With intracranial involvement, mortality approaches 80 to 100 percent regardless of treatment. The rapidity of progression — from sinus disease to brain invasion in 24 to 48 hours in some cases — means that hours matter in the initial management decision.
For pulmonary mucormycosis in the hematologic malignancy/HSCT population, mortality is 65 to 90 percent. The key prognostic determinants in this population are neutrophil recovery (patients who recover their neutrophil count during antifungal therapy have dramatically better outcomes than those who remain neutropenic) and whether surgical resection of the primary pulmonary lesion is feasible. Bilateral pulmonary disease and disseminated disease carry survival rates near zero.
Historically, before the amphotericin B era, mucormycosis was essentially universally fatal. The introduction of surgical debridement combined with amphotericin B (beginning in the 1950s and 1960s) reduced mortality from near 100 percent to the current range of 40 to 80 percent — a meaningful improvement, but far from satisfactory. No treatment advance since has produced comparably dramatic improvements. The addition of isavuconazole as a step-down and the refinement of surgical approaches have improved outcomes at expert centers, but the fundamental biology of the disease — rapid progression, angioinvasion, tissue infarction, and the need to reverse profound immunosuppression — limits how much antifungal pharmacology alone can accomplish.
Key favorable prognostic factors across all forms include: early diagnosis before extensive tissue infarction, complete surgical debridement with clear margins, prompt initiation of high-dose LAmB, successful reversal of the underlying condition (DKA resolution, neutrophil recovery), and treatment at a center with experience in managing this rare infection.
Prevention
Optimal diabetes management is the most impactful population-level prevention measure. The vast majority of rhinocerebral mucormycosis cases occur in patients with uncontrolled or undiagnosed diabetes. Broad public health efforts to identify and treat diabetes before DKA-level decompensation would prevent more cases than any antifungal prophylaxis strategy. At the individual patient level, maintaining HbA1c below 8 percent and educating patients to seek immediate care for DKA symptoms (polyuria, vomiting, abdominal pain) is the primary prevention approach.
Minimizing corticosteroid exposure in immunosuppressed patients is critical. Steroids should be used at the minimum effective dose for the minimum required duration. The COVID-19 era provided a global natural experiment demonstrating that population-level increases in corticosteroid use (entirely medically justified for COVID-19 management) produced parallel increases in mucormycosis incidence in populations with high background diabetes rates. Careful glucose monitoring and insulin supplementation in patients receiving corticosteroids may partially mitigate the hyperglycemia-mediated risk.
Environmental controls for high-risk patients (HSCT recipients and severely neutropenic hematology patients) include HEPA-filtered air supply in hospital rooms, positive-pressure isolation rooms, and restrictions on exposure to construction dust, potted plants, and other environmental Mucorales sources. These measures are primarily directed at aspergillosis but confer parallel protection against mucormycosis given the shared inhalational route of acquisition.
Avoidance of deferoxamine in immunosuppressed and diabetic patients is an absolute preventive measure. Newer oral iron chelators (deferasirox, deferiprone) are preferred when iron chelation is necessary in at-risk patients, though deferasirox should be used cautiously given its own adverse effect profile.
Antifungal prophylaxis specific to mucormycosis is not established. Posaconazole prophylaxis in high-risk hematology patients (AML/MDS induction, GVHD treatment) is standard practice primarily for aspergillosis and candida prevention; it has variable and uncertain activity against Mucorales (in vitro susceptibility data are inconsistent, and clinical evidence is largely observational). There is concern that widespread posaconazole prophylaxis in hematologic malignancy populations may actually select for breakthrough mucormycosis by suppressing the competing aspergillosis flora. Routine mucormycosis-specific prophylaxis is not currently recommended by major guidelines outside of clinical trial settings.
Early recognition protocols at high-risk centers — standing orders for immediate ENT evaluation of neutropenic or diabetic patients with fever and sinus symptoms, and systematic nasal and oral cavity inspection in DKA patients — are low-cost, high-impact prevention measures for the most time-sensitive clinical scenarios.
References
- Cornely OA et al. Global guideline for the diagnosis and management of mucormycosis: an initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium. Lancet Infect Dis. 2019. PMID 31699664
- Patel A et al. Multicenter epidemiologic study of coronavirus disease-associated mucormycosis, India. Emerg Infect Dis. 2021. — Search PubMed
- Spellberg B et al. Novel perspectives on mucormycosis: pathophysiology, presentation, and management. Clin Microbiol Rev. 2005. PMID 16020687
- Ibrahim AS et al. Pathogenesis of mucormycosis. Clin Infect Dis. 2012. PMID 22247443
- Marty FM et al. Isavuconazole treatment for mucormycosis: a single-arm open-label trial and case-control analysis. Lancet Infect Dis. 2016. — Search PubMed
- Skiada A et al. Trends in the epidemiology and clinical characteristics of invasive zygomycosis in Europe: analysis of 230 ECMM cases. Clin Microbiol Infect. 2011. — Search PubMed
- Roden MM et al. Epidemiology and outcome of zygomycosis: a review of 929 reported cases. Clin Infect Dis. 2005. — Search PubMed
- Walsh TJ et al. Treatment of aspergillosis: clinical practice guidelines of the Infectious Diseases Society of America. Clin Infect Dis. 2008. — Search PubMed
- Lanternier F et al. A global analysis of mucormycosis in France: the RetroZygo Study (2005–2007). Clin Infect Dis. 2012. — Search PubMed
- Bitar D et al. Increasing incidence of zygomycosis (mucormycosis), France, 1997–2006. Emerg Infect Dis. 2009. — Search PubMed
- Kontoyiannis DP et al. Zygomycosis in a tertiary-care cancer center in the era of Aspergillus-active antifungal therapy: a case-control observational study of 27 recent cases. J Infect Dis. 2005. — Search PubMed
- Chander J et al. Rhinocerebral zygomycosis: a review of the disease, its risk factors and management. Mycopathologia. 2010. — Search PubMed
Connections
- Infectious Disease
- Aspergillosis
- Cryptococcosis
- Diabetes Mellitus
- Hematology
- HIV/AIDS
- Meningitis
- Pneumonia