Hairy Cell Leukemia
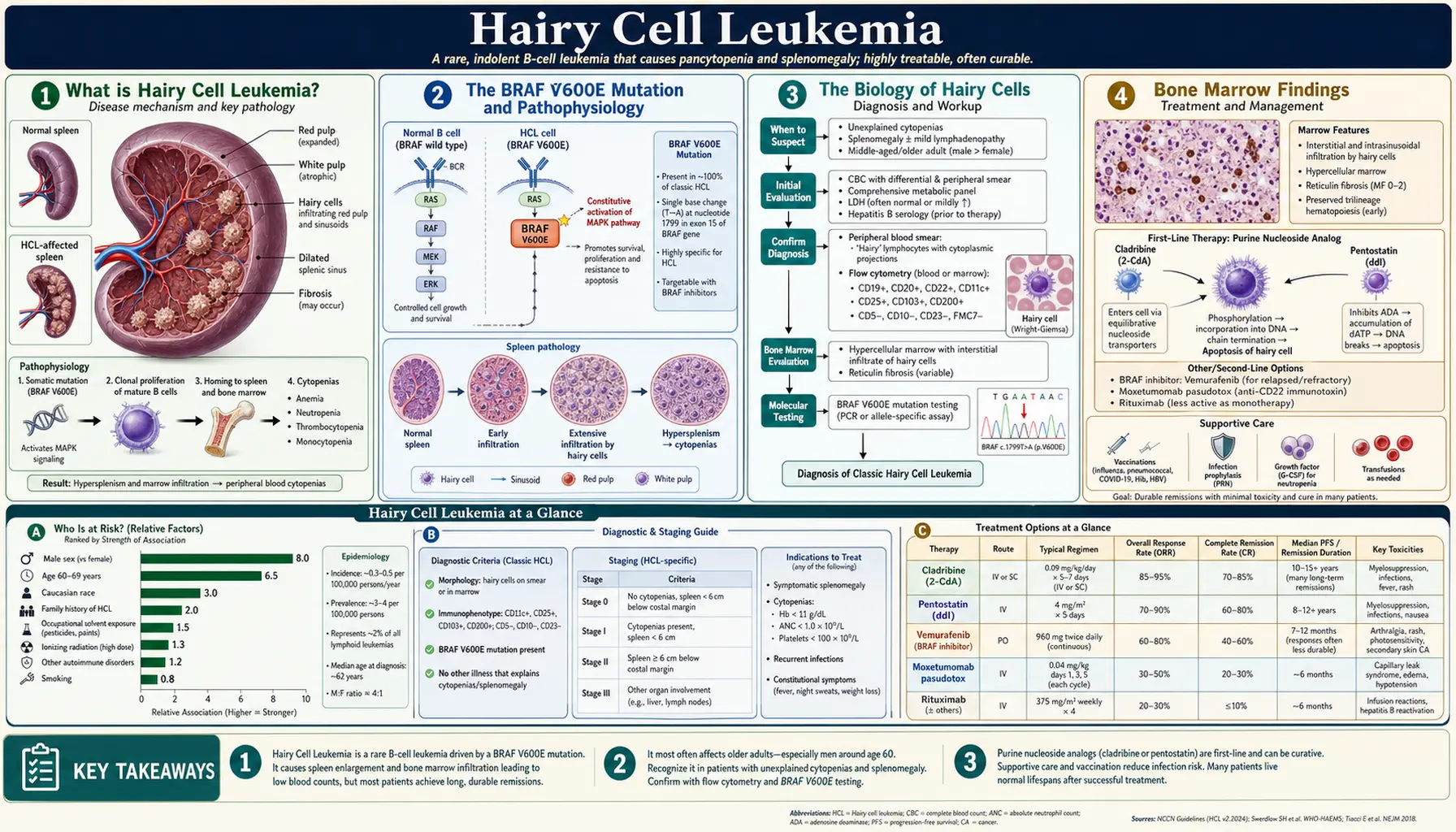
Table of Contents
- What is Hairy Cell Leukemia?
- The BRAF V600E Mutation and Pathophysiology
- The Biology of Hairy Cells
- Bone Marrow Findings
- Clinical Presentation
- Diagnosis: Laboratory and Pathology
- Cladribine: The Transformative Treatment
- Additional Therapies: Pentostatin, Rituximab, Vemurafenib, Moxetumomab
- HCL Variant (HCL-V): A Different Disease
- Long-Term Outcomes and Monitoring
- Research Papers
- Connections
- Featured Videos
What is Hairy Cell Leukemia?
Hairy Cell Leukemia (HCL) is a rare, chronic, mature B-cell lymphoproliferative disorder in which abnormal B lymphocytes accumulate in the bone marrow, spleen, and peripheral blood. The name comes from the characteristic appearance of these malignant cells under a microscope: irregular cytoplasmic projections — called villi or "hairy" extensions — extend outward from the cell surface, giving each cell a shaggy, unkempt appearance resembling fine hairs. These projections are best seen on light microscopy of peripheral blood smears and on electron microscopy, and they are one of the defining visual signatures of the disease.
HCL is uncommon. Approximately 600–800 new cases are diagnosed in the United States each year, accounting for about 2% of all leukemias. It affects predominantly older adults, with a median age at diagnosis of approximately 55 years. Men are affected roughly four times more often than women — one of the largest sex disparities in any hematologic malignancy, though the reason remains unclear. The disease has historically been associated with agricultural exposure, particularly pesticides and herbicides, though no single environmental trigger has been definitively established.
Despite its classification as a leukemia, HCL behaves more like an indolent lymphoma than a rapidly proliferating leukemia. Most patients do not need immediate treatment at diagnosis — a period of watchful waiting may be appropriate for those with mild disease. When treatment is required, HCL has one of the highest rates of durable complete remission of any hematologic malignancy, largely due to the development of purine analogue chemotherapy. For many patients, a single one-week course of cladribine produces a complete remission lasting a decade or longer.
A distinct variant called HCL-Variant (HCL-V) exists — sharing the microscopic "hairy" appearance but differing in molecular biology, immunophenotype, clinical behavior, and treatment response. Distinguishing classic HCL from HCL-V has important management implications and is discussed in its own section below.
The BRAF V600E Mutation and Pathophysiology
The most important discovery in the understanding of hairy cell leukemia was made in 2011: more than 95% of classic HCL cases carry a somatic point mutation in the BRAF gene, specifically the V600E substitution (valine replaced by glutamate at codon 600). This single mutation — the same mutation found in approximately 50% of melanomas and in several other solid tumors — is now recognized as the defining molecular driver of classic HCL.
BRAF and the MAPK/ERK Signaling Cascade
BRAF is a serine-threonine kinase that normally sits within the RAS–RAF–MEK–ERK mitogen-activated protein kinase (MAPK) signaling pathway. Under normal circumstances, this pathway is activated transiently in response to extracellular growth signals: a growth factor binds its receptor, activates RAS, which activates RAF (including BRAF), which phosphorylates MEK, which phosphorylates ERK. Activated ERK then drives nuclear events promoting cell proliferation, survival, and differentiation. Under normal conditions, this cascade switches off once the growth signal is withdrawn.
The BRAF V600E mutation locks BRAF in a permanently "on" state, independent of upstream RAS activation or any external growth signal. The mutant BRAF V600E protein has approximately 500 times the kinase activity of wild-type BRAF. The result is constitutive, growth-factor-independent activation of the MAPK/ERK pathway — driving continuous B-cell proliferation, suppression of apoptosis, and the clonal expansion of the malignant hairy cell population. The mutation is present in essentially every malignant hairy cell in a given patient, confirming it is an early and essential event in HCL pathogenesis rather than a secondary change.
Why Do the Cells Look "Hairy"?
The irregular cytoplasmic projections that give hairy cells their name are not a random morphological quirk — they reflect abnormal cytoskeletal organization driven by constitutive MAPK signaling. The projections are composed of actin filaments and other cytoskeletal proteins reorganized by abnormal kinase activity. In addition to their distinctive appearance, these projections may mediate abnormal interactions with the bone marrow microenvironment and red pulp of the spleen, contributing to the pattern of tissue infiltration characteristic of HCL. Hairy cells also secrete fibronectin, a matrix glycoprotein that promotes bone marrow fibrosis — a key feature that shapes both diagnosis and clinical findings.
The Biology of Hairy Cells
Hairy cells are mature B lymphocytes — they express the full complement of mature B-cell surface antigens and have undergone somatic hypermutation of their immunoglobulin genes, indicating they are post-germinal center cells. Their immunophenotype by flow cytometry is highly characteristic and is central to diagnosis.
Immunophenotype: The CD Marker Pattern
Classic HCL displays a distinctive combination of surface markers that together create a highly specific diagnostic pattern:
- CD19+, CD20+, CD22+: Pan-B-cell markers, confirming B-lymphocyte lineage.
- CD11c+: An integrin (complement receptor 3, CR3) expressed strongly on hairy cells; also seen on monocytes/macrophages (unusual for a B-cell malignancy).
- CD25+: The interleukin-2 receptor alpha chain (IL-2Rα, Tac antigen); strongly expressed in classic HCL but absent in HCL-V — a key distinguishing marker.
- CD103+: An integrin (αE integrin) normally expressed on intraepithelial lymphocytes; unusually expressed on HCL cells and highly specific for the diagnosis when combined with other markers.
- CD123+: The interleukin-3 receptor alpha chain; strongly expressed in classic HCL and helps distinguish it from other B-cell lymphomas.
- CD200+: Expressed on hairy cells; helps distinguish HCL from mantle cell lymphoma and CLL.
- FMC7+: Another B-cell marker expressed on hairy cells.
- Immunoglobulin light chain restriction: Hairy cells express surface immunoglobulin (most commonly IgM or IgG) with restriction to either kappa or lambda light chains, confirming clonality.
The combination of CD103+/CD11c+/CD25+/CD123+ is considered the most diagnostically specific four-marker combination for classic HCL by flow cytometry, with very high sensitivity and specificity. No other B-cell malignancy commonly expresses all four simultaneously.
TRAP Stain: The Classic Cytochemical Test
Before flow cytometry became routine, the tartrate-resistant acid phosphatase (TRAP) stain was the primary diagnostic test for HCL. Hairy cells express a particular isoform of acid phosphatase (isoenzyme 5) that, unlike the acid phosphatase in most other cells, is not inhibited by the addition of tartrate to the reaction mixture. A positive TRAP stain — bright red cytoplasmic granules that persist after tartrate treatment — was once considered nearly pathognomonic for HCL. TRAP staining is now largely supplanted by flow cytometry and BRAF V600E testing for diagnosis but may still be performed in some centers, particularly on bone marrow trephine sections where flow cytometry is not available.
Fibronectin Secretion and Bone Marrow Fibrosis
One of the most clinically significant biological properties of hairy cells is their secretion of fibronectin, an extracellular matrix glycoprotein that stimulates fibroblast activity and collagen deposition. This leads to reticulin fibrosis of the bone marrow — the accumulation of reticulin fibers (a fine type of connective tissue) between the marrow cells. The degree of bone marrow fibrosis in HCL is often severe enough to prevent aspiration of marrow cells through a needle — a phenomenon called a "dry tap" — making bone marrow trephine biopsy (a core biopsy) essential for diagnosis rather than an optional adjunct.
Bone Marrow Findings
The bone marrow in hairy cell leukemia shows a constellation of characteristic findings that, together, are highly specific for the diagnosis. Because of the fibrosis-induced dry tap, a trephine biopsy (core biopsy of a cylinder of marrow) is required for full evaluation.
The Dry Tap
When a hematologist performs a bone marrow aspirate in a patient with HCL, the needle passes into the marrow space as expected — but instead of yielding the usual liquid suspension of marrow cells that can be aspirated into a syringe, only blood or fibrous material is obtained. This dry tap occurs because the reticulin fibrosis from fibronectin secretion has created a rigid structural matrix that cannot be disrupted and aspirated. A dry tap in an adult being evaluated for cytopenias or splenomegaly should always raise suspicion for HCL (as well as other marrow fibrosis conditions such as primary myelofibrosis).
The Fried-Egg Appearance
On the trephine biopsy specimen, hairy cells display one of the most visually distinctive morphological patterns in hematopathology: the "fried-egg" appearance. Each hairy cell nucleus sits at the center of a large zone of pale, clear cytoplasm — separated from the nuclei of neighboring cells by abundant pale cytoplasm — giving the impression of a row of eggs sunny-side-up on a griddle. This spacious halo of cytoplasm reflects the abundant pale cytoplasm of hairy cells and the reticulin fibers between them that prevent the cells from clustering tightly. The fried-egg pattern is so characteristic that experienced hematopathologists can recognize HCL on low-power microscopy of a trephine biopsy.
ANNEXIN A1: The Most Specific Immunohistochemical Marker
On trephine biopsy sections, immunohistochemical staining for ANNEXIN A1 is the most specific single marker for classic HCL currently available. Annexin A1 is a calcium-binding protein normally expressed in granulocytes and monocytes — not in lymphocytes. Its aberrant expression in hairy cells (a B-lymphocyte malignancy) makes positive Annexin A1 staining highly specific for HCL. In practice, Annexin A1 staining is positive in essentially all classic HCL cases and negative in HCL-V and other B-cell lymphomas. Annexin A1 immunostaining is particularly valuable in the trephine biopsy setting where flow cytometry may be suboptimal due to fibrous material, and in archived (formalin-fixed, paraffin-embedded) specimens where flow cytometry is not possible.
Degree of Marrow Infiltration
Hairy cells typically infiltrate the bone marrow in an interstitial or diffuse pattern, weaving between residual normal hematopoietic cells and fat spaces. As the disease advances, the percentage of marrow space occupied by hairy cells increases, progressively displacing normal blood cell production — explaining the pancytopenia. Some patients show focal nodular infiltration rather than diffuse disease at early diagnosis.
Clinical Presentation
The clinical picture of hairy cell leukemia is shaped by two processes operating simultaneously: infiltration of the bone marrow (reducing normal blood cell production) and infiltration of the spleen (causing hypersplenism and massive organ enlargement). These two mechanisms together produce the characteristic clinical syndrome.
Pancytopenia: The Blood Count Picture
Pancytopenia — reduction in all three blood cell lines — is the most common laboratory finding at diagnosis and is present in the majority of patients to some degree. Each component has its own clinical consequences:
- Anemia (low red blood cells): Fatigue, weakness, pallor, shortness of breath on exertion, and reduced exercise tolerance are the most common complaints that bring patients to medical attention. Anemia in HCL is normocytic and due to marrow infiltration plus hypersplenism (accelerated red cell destruction in the enlarged spleen).
- Thrombocytopenia (low platelets): Easy bruising, petechiae (pinpoint skin hemorrhages), and prolonged bleeding from minor cuts. Severe thrombocytopenia (<50,000/µL) increases the risk of significant bleeding.
- Neutropenia (low neutrophils): Recurrent bacterial infections, particularly by encapsulated organisms and gram-negative bacteria. Infection is the most common cause of death in HCL — both from untreated disease and as a complication of treatment. Severe neutropenia (<500/µL) creates vulnerability to opportunistic infections and sepsis.
Massive Splenomegaly: The Hallmark Physical Finding
Massive splenomegaly is the most characteristic physical examination finding in HCL and is present in approximately 80–90% of patients at diagnosis. The spleen can be dramatically enlarged — sometimes extending across the midline of the abdomen and into the pelvis — and is often the reason a patient first seeks medical care, presenting with left-sided abdominal fullness, early satiety, or a palpable abdominal mass. Hairy cells have a strong predilection for the red pulp of the spleen (the filtering, sinusoidal region), which is unusual — most lymphoid malignancies home to the white pulp. Red pulp infiltration by hairy cells, combined with the fibronectin-induced fibrosis, leads to massive splenic enlargement. The degree of splenomegaly in HCL is characteristically out of proportion to the degree of peripheral blood cytopenias and lymphadenopathy.
Monocytopenia: A Very Characteristic Feature
One of the most diagnostically specific findings in HCL is monocytopenia — a near-complete absence of circulating monocytes in the peripheral blood. Normal monocyte counts range from approximately 200–800 per microliter; in HCL, monocyte counts below 100/µL (and often below 20/µL) are the rule. This monocytopenia is so characteristic that its presence in a patient with splenomegaly and cytopenias should prompt immediate evaluation for HCL.
The clinical consequence of monocytopenia is an unusual vulnerability to infections caused by organisms that are normally handled by monocytes and macrophages — most notably atypical mycobacteria (non-tuberculous mycobacteria such as Mycobacterium avium complex, M. kansasii, and M. fortuitum). Disseminated atypical mycobacterial infection in a middle-aged man with splenomegaly is a classic presentation of undiagnosed HCL. Legionella and fungal infections also occur with increased frequency due to monocyte deficiency.
Minimal Lymphadenopathy
Unlike chronic lymphocytic leukemia (CLL) and most other B-cell lymphomas — where lymph node enlargement is a prominent and often presenting feature — HCL causes minimal to absent peripheral lymphadenopathy in most patients. This is a clinically important distinguishing feature. Intra-abdominal lymphadenopathy (involving mesenteric or retroperitoneal nodes) may occasionally be detected on imaging, but peripheral lymph nodes are typically not enlarged to clinical palpation. The contrast between massive splenomegaly and minimal lymphadenopathy is one of the classic clinical clues to the diagnosis of HCL.
Presentation Mode
Many HCL patients are diagnosed incidentally — a routine complete blood count reveals unexpected pancytopenia in a person without symptoms, prompting further evaluation that leads to the diagnosis. Others present with fatigue from anemia, recurrent infections from neutropenia, or an incidentally discovered enlarged spleen during abdominal examination for an unrelated complaint. A small proportion of patients discover a palpable abdominal mass themselves. Constitutional symptoms (fever, night sweats, weight loss — the "B symptoms" of lymphoma) are uncommon in HCL at diagnosis.
Diagnosis: Laboratory and Pathology
The diagnosis of HCL rests on a combination of peripheral blood examination, bone marrow trephine biopsy, flow cytometry, and BRAF V600E molecular testing. No single test is sufficient alone, and the full picture across modalities is required for confident diagnosis.
Complete Blood Count and Peripheral Smear
The CBC typically shows pancytopenia in varying degrees. The absolute monocyte count is almost always severely reduced. Hairy cells themselves can sometimes be identified on the peripheral blood smear — their irregular cytoplasmic projections visible on careful examination — in approximately 10–20% of cases, but blood counts may be normal or only mildly abnormal in early disease, and hairy cells may be sparse. Leukocytosis (elevated total white count due to circulating hairy cells) is more common in HCL-V than classic HCL.
Bone Marrow Trephine Biopsy
As described above, the dry tap from the aspirate makes the trephine biopsy the essential diagnostic specimen. The fried-egg morphology, Annexin A1 immunostaining, and the pattern of reticulin fibrosis are evaluated on the trephine core. A reticulin stain confirms the degree of marrow fibrosis. Immunohistochemistry panels on the biopsy can include CD20, CD103, Annexin A1, and DBA.44 (another HCL-associated marker).
Flow Cytometry: The Immunophenotypic Fingerprint
Flow cytometry of peripheral blood or bone marrow aspirate (even when the aspirate yield is poor) is the most powerful diagnostic tool for HCL, identifying the specific CD marker combination that is essentially pathognomonic. The classic HCL immunophenotype — CD103+, CD11c+, CD25+, CD123+ on a clonal B-cell population — has very high sensitivity and specificity. Flow cytometry can also quantify the hairy cell burden in the blood and marrow, which is useful for monitoring minimal residual disease (MRD) after treatment.
BRAF V600E Molecular Testing
Testing for the BRAF V600E mutation is now a standard part of HCL diagnosis and is particularly valuable in three situations: (1) confirming the diagnosis of classic HCL versus HCL-V (which lacks the BRAF mutation); (2) establishing the diagnosis when biopsy material is limited or flow cytometry results are equivocal; and (3) monitoring for residual disease by highly sensitive PCR-based assays. The mutation can be detected by allele-specific PCR or digital droplet PCR on peripheral blood DNA with high sensitivity, even when the hairy cell burden in the blood is low. Immunohistochemistry using a VE1 antibody (which specifically recognizes the V600E mutant BRAF protein) can be performed on trephine biopsy sections as a practical screening test.
Imaging
CT scanning of the abdomen and pelvis is typically performed to assess the degree of splenomegaly and to look for intra-abdominal lymphadenopathy. The spleen in HCL often shows a characteristic homogeneous enlargement without discrete nodularity on CT — in contrast to lymphoma, where discrete splenic nodules may be seen. PET-CT is not routinely required for HCL staging but may be used in complex diagnostic situations or to evaluate potential transformation.
Cladribine: The Transformative Treatment
The development of cladribine (2-chlorodeoxyadenosine, 2-CdA) for hairy cell leukemia was one of the landmark achievements in modern hematology, transforming a disease with very limited treatment options into one of the most curable hematologic malignancies in terms of durable remission. For most patients with classic HCL requiring treatment, a single course of cladribine produces a complete remission lasting a decade or more.
Mechanism of Action
Cladribine is a purine nucleoside analogue — a synthetic compound that resembles the natural nucleoside deoxyadenosine. After uptake into cells and phosphorylation by the intracellular enzyme deoxycytidine kinase (dCK), cladribine is incorporated into DNA during replication and also accumulates as a triphosphate metabolite that inhibits DNA synthesis and repair enzymes. Critically, cladribine is resistant to degradation by adenosine deaminase (ADA) — the enzyme that normally inactivates natural deoxyadenosine. This ADA-resistance allows cladribine to accumulate to lethal levels in lymphoid cells, which have relatively high dCK activity and low ADA activity compared to other cell types. The net effect is selective cytotoxicity to lymphocytes, including malignant hairy cells, with relative sparing of non-lymphoid tissues.
Dosing Schedules
Cladribine is given as a short, single course of treatment. Two main schedules have been used:
- 7-day continuous intravenous infusion: Cladribine 0.09 mg/kg/day by continuous IV infusion for 7 days — the original FDA-approved schedule (approved 1992). This schedule requires either hospitalization with a central venous catheter for 7 days, or home administration via a portable infusion pump with an implanted port. It provides the original evidence base.
- 5-day subcutaneous or IV bolus schedule: Cladribine 0.14 mg/kg/day by IV infusion over 2 hours or by subcutaneous injection, once daily for 5 days. Equivalent total drug exposure to the 7-day schedule; equivalent efficacy; more convenient (outpatient administration, no continuous infusion device needed). This schedule has become widely preferred in clinical practice.
Response Rates and Durability
The efficacy of cladribine in classic HCL is remarkable. In the original series by Piro and colleagues at Scripps Clinic (1990), 11 of 12 patients achieved complete remission with a single course. Subsequent larger studies have confirmed:
- Complete remission rate: 80–90% after a single course in previously untreated patients.
- Partial remission rate: An additional 5–10%; most eventually convert to complete remission with retreatment or additional therapy.
- Median duration of first remission: Exceeds 10 years in most published series — meaning the average patient who achieves complete remission stays in remission for more than a decade after just one week of treatment.
- 10-year relapse-free survival: Approximately 55–65% in the largest series, with many patients achieving what appears to be functional cure.
Toxicity and Supportive Care
Cladribine is profoundly immunosuppressive. Even at the standard single-course dose, it depletes CD4+ T lymphocytes (T-helper cells) to very low levels — sometimes below 200 cells/µL (comparable to AIDS-level CD4 depletion) — for a period lasting weeks to months after treatment. This severe lymphopenia creates vulnerability to opportunistic infections, particularly:
- Pneumocystis jirovecii pneumonia (PCP): The most important opportunistic infection risk. Prophylaxis with trimethoprim-sulfamethoxazole (TMP-SMX) is required during and after cladribine treatment — typically continued until CD4+ counts recover above 200 cells/µL. Patients intolerant of TMP-SMX can use atovaquone or pentamidine.
- Herpes virus reactivation: Acyclovir prophylaxis is also commonly used to prevent reactivation of herpes simplex and varicella-zoster virus during the immunosuppressed period.
- Neutropenic fever: Febrile neutropenia in the first weeks after cladribine is common and requires prompt evaluation and empiric antibiotics.
Non-infectious toxicities of cladribine include nausea (mild, manageable), transient elevation of liver enzymes, and — rarely — neurotoxicity at high doses. Prolonged bone marrow suppression causes the peripheral blood counts to initially worsen after treatment (the drug kills hairy cells, but also transiently suppresses recovery) before improving over 4–8 weeks as normal hematopoiesis rebounds in the now-cleared marrow. Patients need close monitoring during this nadir period.
Additional Therapies: Pentostatin, Rituximab, Vemurafenib, Moxetumomab
While cladribine is the standard first-line treatment for classic HCL, a range of other agents play important roles in specific situations — as alternative first-line therapy, for eradication of minimal residual disease, or for relapsed and refractory disease.
Pentostatin (Deoxycoformycin)
Pentostatin is the other major purine analogue used in HCL. Unlike cladribine (which is ADA-resistant), pentostatin works by directly inhibiting adenosine deaminase itself, causing accumulation of naturally occurring deoxyadenosine to toxic levels in lymphocytes. Pentostatin has demonstrated complete remission rates of 76–89% in classic HCL and overall survival rates comparable to cladribine in randomized comparisons. The main practical difference is the dosing schedule: pentostatin is given as IV infusions every 2 weeks for 3–6 months, rather than as a single concentrated one-week course. This makes pentostatin administration more drawn out, but it may be preferred in some patients with specific comorbidities or concerns. Toxicity profile is similar to cladribine — immunosuppression, neutropenic fever, and opportunistic infection risk.
Rituximab
Rituximab is a chimeric anti-CD20 monoclonal antibody that depletes B lymphocytes by binding CD20 on their surface and directing immune destruction. Since hairy cells strongly express CD20 (CD20+), rituximab has significant activity in HCL. Rituximab's roles in HCL include:
- Combination with cladribine for upfront therapy: The combination of cladribine followed by rituximab has been evaluated in a phase 2 study (Ravandi et al., MD Anderson Cancer Center) demonstrating very high rates of minimal residual disease (MRD) negativity — essentially clearing every last detectable hairy cell from the marrow. Whether this translates to longer remissions compared to cladribine alone is still being studied.
- Treatment of minimal residual disease (MRD): After cladribine produces a clinical complete remission, sensitive flow cytometry or PCR testing can still detect small numbers of hairy cells (MRD positive). Rituximab can eradicate MRD and may prolong relapse-free survival.
- Relapsed or refractory HCL: Rituximab monotherapy or combined with a purine analogue for patients who relapse after initial cladribine treatment.
Vemurafenib (BRAF V600E Inhibitor)
The discovery that >95% of classic HCL cases carry the BRAF V600E mutation immediately suggested targeted therapy with BRAF V600E inhibitors — the same drugs developed for BRAF-mutant melanoma. Vemurafenib (and more recently dabrafenib) inhibit the constitutively active mutant BRAF kinase, turning off the MAPK/ERK signaling that drives hairy cell proliferation and survival.
Clinical results in relapsed/refractory HCL have been impressive: overall response rates of 96–100%, with complete remission rates of approximately 35–40% after vemurafenib alone in heavily pretreated patients. However, the limitation of BRAF inhibition as monotherapy is the relatively short median progression-free survival — approximately 9–19 months — compared to the 10+ year remissions achievable with cladribine. Resistance typically develops through reactivation of the MAPK pathway through alternate mechanisms. Vemurafenib is currently used for relapsed/refractory HCL, for patients with HCL-V (which lacks BRAF mutation responses to purine analogues), and increasingly in combination regimens with rituximab designed to achieve deeper, more durable responses. The BRAF-plus-rituximab combination (vemurafenib 960 mg twice daily + rituximab) has shown very high CR rates in relapsed disease.
Moxetumomab Pasudotox
Moxetumomab pasudotox-tdfk (Lumoxiti) is an anti-CD22 recombinant immunotoxin — a fusion protein consisting of a CD22-targeting antibody fragment connected to a fragment of Pseudomonas exotoxin A. CD22 is strongly expressed on hairy cells. When moxetumomab binds CD22 on a hairy cell, the immunotoxin is internalized and the Pseudomonas toxin fragment inhibits protein synthesis, killing the cell. Moxetumomab was FDA approved in September 2018 for adult patients with relapsed or refractory HCL who have received at least two prior therapies (including at least one purine analogue). The pivotal trial showed an overall response rate of 75% and a complete remission rate of 41%, with a very durable remission duration in CR patients. Key toxicities include hemolytic uremic syndrome (HUS), capillary leak syndrome, and thrombosis — requiring careful patient selection and monitoring. Moxetumomab is given as a 30-minute IV infusion on days 1, 3, and 5 of each 28-day cycle.
HCL Variant (HCL-V): A Different Disease
Hairy Cell Leukemia Variant (HCL-V) is a distinct clinicopathological entity that shares superficial features with classic HCL — most notably the presence of "hairy" cytoplasmic projections on the malignant cells visible on peripheral smear — but differs fundamentally in molecular biology, immunophenotype, clinical behavior, and response to standard HCL therapy. HCL-V was first recognized as a separate entity in the 1980s and comprises approximately 10% of all HCL diagnoses.
Key Differences from Classic HCL
- BRAF wild-type: The defining molecular distinction. HCL-V does not carry the BRAF V600E mutation. Instead, HCL-V commonly harbors mutations in MAP2K1 (the gene encoding MEK1, the kinase immediately downstream of BRAF in the MAPK pathway) or other pathway components. The absence of BRAF V600E mutation makes HCL-V unresponsive to BRAF inhibitors such as vemurafenib.
- CD25-negative: Unlike classic HCL (which is CD25+), HCL-V cells do not express CD25 (IL-2Rα). This marker is one of the most reliable distinguishing features between the two entities on flow cytometry.
- Annexin A1-negative: HCL-V cells do not express Annexin A1 on immunohistochemistry, in contrast to classic HCL.
- Higher white blood cell count: HCL-V often presents with leukocytosis (elevated total white count from circulating hairy variant cells) rather than the leukopenia typical of classic HCL. Splenomegaly is prominent, as in classic HCL.
- More aggressive clinical behavior: HCL-V follows a more aggressive clinical course than classic HCL, with shorter survival in historical series and earlier need for treatment.
- Reduced response to purine analogues: HCL-V responds poorly to cladribine and pentostatin compared to classic HCL. Complete remission rates with purine analogues are substantially lower — approximately 50% versus 80–90% in classic HCL — and remissions are shorter.
- Monocytopenia less prominent: The near-complete monocyte depletion characteristic of classic HCL is typically less severe or absent in HCL-V.
Treatment of HCL-V
Because HCL-V responds poorly to purine analogues as monotherapy, combination approaches are preferred:
- Pentostatin plus rituximab: The combination has shown higher response rates in HCL-V than either agent alone and is a commonly used regimen.
- Cladribine plus rituximab: Also used in HCL-V, with some improved responses compared to cladribine alone.
- Vemurafenib (with caution): Since HCL-V is BRAF wild-type, standard BRAF inhibitors are not appropriate. However, in HCL-V cases with MAP2K1 mutations, MEK inhibitors (trametinib, cobimetinib) are being investigated.
- Moxetumomab pasudotox: Since HCL-V cells express CD22, moxetumomab has activity and is an option for relapsed/refractory HCL-V.
- Splenectomy: Historically used in both classic HCL and HCL-V as palliative therapy, before effective medical treatments existed; now rarely needed but may be considered in selected HCL-V patients with massive symptomatic splenomegaly.
Long-Term Outcomes and Monitoring
Hairy cell leukemia is one of the success stories of modern hematology. Most patients with classic HCL achieve long-term remission with cladribine — often measured in decades — and die of unrelated causes rather than HCL. Nevertheless, HCL requires long-term surveillance because relapse can occur even after many years of remission, and monitoring tools now exist to identify recurrence early.
The Concept of Complete Remission in HCL
In HCL, complete remission (CR) is defined as normalization of peripheral blood counts (hemoglobin, platelet count, neutrophil count), disappearance of splenomegaly, and absence of hairy cells on bone marrow biopsy by standard histology and immunohistochemistry. Achieving CR after cladribine predicts significantly longer relapse-free survival than achieving only a partial response. However, even within "complete remission" by conventional criteria, many patients have detectable hairy cells by very sensitive tests — a concept called minimal residual disease (MRD).
Minimal Residual Disease
MRD in HCL can be assessed by multicolor flow cytometry (able to detect 1 hairy cell in 10,000 normal cells) or by allele-specific PCR for BRAF V600E (even more sensitive). Studies have shown that MRD-positive patients — those whose conventional CR is achieved but who have detectable hairy cells by sensitive testing — have a higher long-term risk of clinical relapse than MRD-negative patients. This has generated interest in MRD-directed therapy: treating MRD positivity with rituximab to eradicate remaining hairy cells and potentially prolong time to clinical relapse. Several investigators now recommend MRD assessment at 4–6 months after cladribine, with rituximab offered to MRD-positive patients.
Relapse Patterns and Retreatment
Relapse after cladribine can occur at any time after the initial response. Several patterns are recognized:
- Late relapse (>5 years): Most common. Patients who relapse after a long first remission can often be retreated with a second course of cladribine, with response rates of approximately 50–70%.
- Early relapse (<2 years): Suggests relative resistance to cladribine. These patients are better treated with an alternative regimen — rituximab plus a purine analogue, or vemurafenib-based therapy.
- Sequential therapies: With multiple effective options available (cladribine, pentostatin, rituximab, vemurafenib, moxetumomab), patients can often receive several lines of treatment over many years, achieving clinical remissions with each, resulting in cumulative survival measured in decades.
Second Malignancies
Long-term follow-up studies of HCL survivors have identified a modestly elevated risk of second cancers compared to the general population. The most commonly reported second malignancies include non-Hodgkin lymphomas (distinct from HCL), myeloid neoplasms, and certain solid tumors. Whether this reflects a shared etiological factor (such as pesticide exposure), immunosuppression from HCL treatment, or a background predisposition of the HCL B-cell clone to genomic instability is not fully established. Patients should follow standard age-appropriate cancer screening guidelines.
Monitoring Schedule
After achieving complete remission with cladribine, monitoring typically includes:
- Complete blood count every 3 months for 2 years, then every 6 months thereafter.
- Bone marrow biopsy with flow cytometry at 4–6 months after treatment to document depth of remission and assess MRD.
- Peripheral blood BRAF V600E PCR for MRD monitoring (high sensitivity, non-invasive).
- Annual physical examination with assessment of spleen size.
- Prompt evaluation of any unexplained cytopenias, recurrent infections, or new splenomegaly — early signs of relapse.
Patients with HCL generally maintain excellent quality of life during long remissions, with normalization of blood counts, resolution of fatigue and infection susceptibility, and return to full normal activity. The long-term CD4+ lymphopenia induced by cladribine generally resolves within 1–2 years after treatment in most patients.
Research Papers
The following PubMed links point to pivotal peer-reviewed studies on hairy cell leukemia, covering pathophysiology, the BRAF V600E discovery, treatment trials, and long-term outcomes.
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Robak T et al. (2017) Hairy cell leukemia: an overview — Blood — PMID 28034894
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
Connections
- Hematology
- Chronic Lymphocytic Leukemia
- Multiple Myeloma
- Waldenström's Macroglobulinemia
- Non-Hodgkin's Lymphoma
- Aplastic Anemia
- Thrombocytopenia
- Anemia
- Splenomegaly
- Myelofibrosis
- Atypical Mycobacterial Infections
- Pneumocystis Pneumonia (PCP)
- Complete Blood Count
- Leukemia Overview — the broader family of blood cancers HCL accounts for about 2% of.