Cyclic Vomiting Syndrome
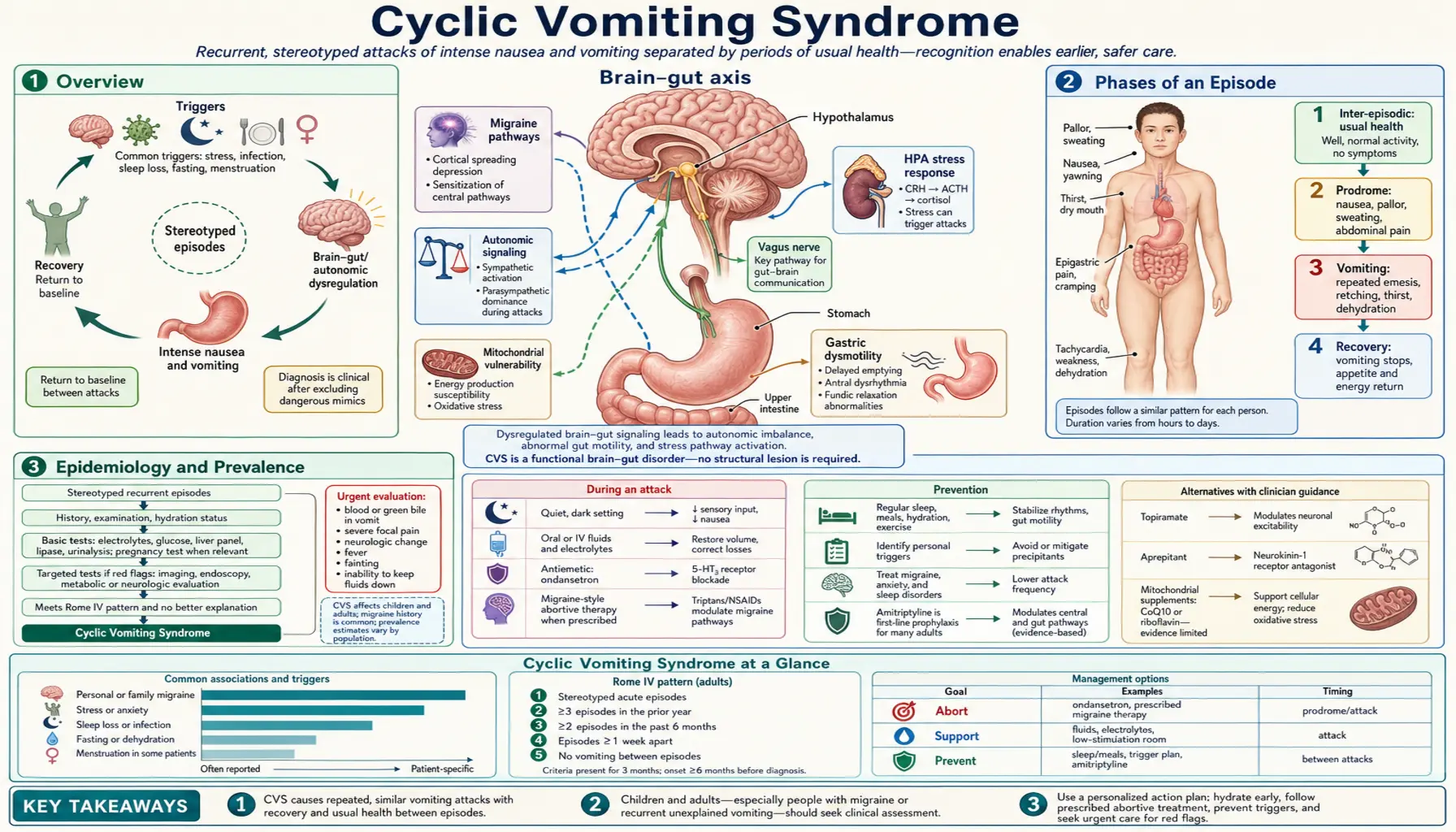
Table of Contents
- Overview
- Phases of an Episode
- Epidemiology and Prevalence
- Pathophysiology
- Triggers
- Cannabis Hyperemesis Syndrome
- Diagnosis
- Abortive Treatment
- Prophylactic Treatment
- Complications
- Prognosis and Long-term Outcomes
- References
- Connections
- Featured Videos
1. Overview
Cyclic Vomiting Syndrome (CVS) is a functional gut-brain disorder characterized by recurrent, stereotyped episodes of intense nausea and vomiting that are separated by completely symptom-free intervals. Each episode follows a predictable personal pattern — the same warning signs, the same severity, the same duration — and then resolves entirely, leaving the person feeling completely normal between attacks. This stereotypy is both the hallmark diagnostic feature and one of the most puzzling aspects of the condition.
CVS belongs to the family of migrainous disorders. More than 90% of patients with CVS have a personal or family history of migraine headaches, and CVS is now understood as a gut-brain axis disorder in which the migraine-generating mechanisms of the central nervous system manifest in the gastrointestinal tract rather than — or in addition to — the head. Many children with CVS go on to develop classic migraine headaches as adults, and the two conditions respond to the same prophylactic medications.
Despite its significant burden — episodes can last days, require emergency hospitalization, and cause chronic dehydration — CVS remains underdiagnosed. The average delay between symptom onset and correct diagnosis exceeds 3 years. Clinicians unfamiliar with the condition often pursue repeated unnecessary endoscopies and imaging studies before recognizing the characteristic episodic pattern.
2. Phases of an Episode
A CVS episode unfolds in three clinically distinct phases. The timing and characteristics of each phase are remarkably consistent for a given individual across different episodes, which is why recognizing the patient's personal pattern is central to both diagnosis and management.
Phase 1: Prodrome (30–60 Minutes)
The prodrome signals that an episode is imminent. It typically lasts 30 to 60 minutes and gives patients and families a narrow window to initiate abortive therapy. Key features include:
- Intense nausea — often described as building waves of sickness rather than constant queasiness
- Pallor — a characteristic blanching of the skin, particularly notable in children
- Profuse sweating (diaphoresis) — cold sweats out of proportion to the degree of physical activity
- Lethargy and social withdrawal — children often become quiet and stop playing; adults retreat to a darkened room
- Abdominal pain — a cramping or burning sensation, often periumbilical, that intensifies through the prodrome
- Photophobia and phonophobia — sensitivity to light and sound, mirroring migraine prodrome features
Recognizing the prodrome is clinically critical because triptans and antiemetics administered during this phase can abort some episodes entirely before the vomiting phase begins.
Phase 2: Vomiting Phase (Hours to Days)
The vomiting phase is the defining and most debilitating part of the episode. Vomiting is intense, forceful, and relentless — occurring up to 6 times per hour at peak intensity, compared to the 1–2 episodes per hour typical of gastroenteritis. The median episode duration is approximately 5 days in adults (range: a few hours to more than 10 days), though pediatric episodes tend to be somewhat shorter.
During this phase, patients typically:
- Are incapacitated and unable to eat, drink, or stand
- Seek a dark, quiet, cool room (heightened sensory sensitivity identical to migraine)
- Experience severe abdominal pain and retching even when nothing remains in the stomach (dry heaving)
- Show signs of progressive dehydration: dry mucous membranes, decreased urine output, orthostatic hypotension
- Often require emergency department visits for intravenous fluid replacement and antiemetic therapy
A characteristic but underappreciated feature of the vomiting phase is its predictable onset time. Many patients find their episodes begin at the same hour of day — frequently in the early morning hours (2–4 AM) — following their personal biological clock. This circadian pattern is consistent across episodes for the same patient and is another diagnostic clue distinguishing CVS from other causes of recurrent vomiting.
Phase 3: Recovery Phase
The recovery phase begins when vomiting ceases and the patient can tolerate oral intake. Recovery is not instantaneous — it typically takes 24–48 hours of gradual rehydration, light foods, and rest before the person feels fully normal. However, the defining feature of recovery from a CVS perspective is its completeness: patients return to their exact baseline state of health with no residual nausea, pain, or functional impairment between episodes. This symptom-free interlude is the feature that most clearly distinguishes CVS from chronic conditions such as gastroparesis or functional dyspepsia, where symptoms persist continuously at varying intensity.
3. Epidemiology and Prevalence
CVS was historically considered a rare childhood disorder, but large-scale population studies have established it as more prevalent than previously recognized. In adults, prevalence estimates range from 1.9% to 2.7% of the general population — comparable to the prevalence of inflammatory bowel disease. In children, population-based estimates suggest a prevalence of approximately 1.9–2.3%, with a peak incidence in the school-age years (5–12 years old).
CVS affects women and men roughly equally in adults, though some series show a slight female predominance. In children, boys are affected slightly more often than girls. The condition is diagnosed across all ethnic groups, though published series may underrepresent non-White populations due to diagnostic access barriers.
The true prevalence is almost certainly higher than reported figures, because:
- The diagnosis requires recognizing the stereotyped episodic pattern, which can take years of repeated presentations to become apparent
- Episodes are frequently attributed to acute gastroenteritis, food poisoning, or psychosomatic causes
- Many patients normalize their pattern ("I always get these sick spells a few times a year") without seeking specialized evaluation
- CVS in adults was only formally characterized and given diagnostic criteria in the late 2000s, long after pediatric CVS was recognized
Economically, CVS imposes a substantial burden. Emergency department visits average 2–5 per patient per year, each generating hospitalization costs for IV fluids, antiemetics, and diagnostic workup. School absenteeism in children and workplace absenteeism in adults are major impacts; one study found that adults with CVS missed a mean of 22 days of work per year attributable to episodes.
4. Pathophysiology
The pathophysiology of CVS is incompletely understood, but converging evidence points to dysfunction at the intersection of the central nervous system, autonomic nervous system, hypothalamic-pituitary-adrenal (HPA) axis, and mitochondrial energy metabolism — all consistent with its classification as a disorder of the gut-brain axis.
Gut-Brain Axis and Migraine Overlap
CVS shares a mechanistic kinship with migraine at multiple levels. Both conditions feature episodic attacks, stereotyped symptom patterns, similar triggers (stress, hormonal changes, certain foods, sleep disruption), identical autonomic features (pallor, diaphoresis, nausea, photophobia), and response to the same treatments (triptans, amitriptyline, topiramate). The leading hypothesis is that CVS represents a migraine variant in which the brain's migraine-generating cascade activates the vomiting center in the brainstem (area postrema) and dorsal vagal complex rather than — or in addition to — the cortical spreading depression that underlies visual aura and headache.
The trigeminovascular system, central sensitization pathways, and serotonergic neurotransmission that are dysregulated in migraine are similarly implicated in CVS. The high co-occurrence of CVS and migraine (90% of CVS patients have personal or family migraine history) and the frequent transition from childhood CVS to adult migraine headaches support shared underlying neurobiology.
Corticotropin-Releasing Factor (CRF) and the HPA Axis
Physical or emotional stress — the most common CVS trigger — activates the hypothalamus to release corticotropin-releasing factor (CRF), which coordinates the stress response via the HPA axis (stimulating cortisol release) and directly activates CRF receptors in the brainstem vomiting centers and the enteric nervous system. In susceptible individuals with CVS, this CRF-driven stress circuit appears to be dysregulated — with exaggerated or sustained CRF signaling translating acute stressors into the full vomiting cascade. This mechanism explains why episodes cluster during periods of psychological stress, illness, or physiological stress (menstruation, exercise, sleep deprivation).
Mitochondrial Dysfunction
A subset of CVS patients — particularly those with maternal inheritance patterns and additional features suggesting mitochondrial disease (exercise intolerance, developmental delays, myopathy) — carry mitochondrial DNA variants affecting energy metabolism. A landmark study by Boles et al. identified mitochondrial DNA variants in a significant proportion of CVS patients, and there is substantial overlap between CVS and mitochondrial disorders.
The mitochondrial hypothesis proposes that cells with high energy demands (neurons, enterocytes, cardiomyocytes) in CVS patients have impaired mitochondrial oxidative phosphorylation. During metabolic stress — illness, fasting, intense exercise, hormonal fluctuations — energy depletion in these cells triggers the vomiting cascade. This hypothesis explains the efficacy of mitochondrial cofactors (coenzyme Q10, riboflavin/B2, L-carnitine) as CVS prophylaxis, as these agents support mitochondrial respiratory chain function.
Autonomic Nervous System Dysregulation
CVS patients demonstrate measurable autonomic dysfunction during both episodes and interictal periods. Tilt-table testing reveals orthostatic intolerance in many patients. Heart rate variability analysis shows reduced parasympathetic tone. Skin conductance studies confirm heightened sympathetic reactivity. The sympathetic surges that accompany emotional or physical stress may directly trigger CRF release and activate the brainstem vomiting centers, representing the neurological bridge between environmental triggers and episodes.
5. Triggers
Identifying and managing personal triggers is a cornerstone of CVS prevention. Triggers vary among patients, but certain categories recur consistently across the literature:
Psychological and Physical Stress
Stress — both emotional (anxiety, excitement, conflict, grief, anticipatory excitement before holidays) and physical (illness, overexertion, travel, sleep deprivation) — is the most commonly reported trigger, identified in 50–80% of patients. Importantly, positive excitement (birthday parties, holidays, school events) triggers episodes as commonly as negative stress, reflecting the shared HPA axis activation regardless of valence.
Menstrual Cycle
In women of reproductive age, episodes frequently cluster perimenstrually — in the days preceding or during menstruation. This pattern, sometimes called menstrual CVS, reflects the hormonal triggers of estrogen and progesterone fluctuations, which also trigger migraine attacks in many women. Recognition of this pattern can guide contraceptive strategies (hormonal suppression of the menstrual cycle) as an adjunct to standard prophylaxis.
Infections
Viral or bacterial illnesses — particularly upper respiratory infections and gastroenteritis — frequently precipitate CVS episodes. The combination of systemic inflammation, fever, and HPA axis activation during infection lowers the threshold for episode initiation. This creates a confusing clinical picture, as the vomiting of a CVS episode triggered by viral illness can be indistinguishable from the vomiting of the illness itself during the acute phase.
Dietary Triggers
Specific foods trigger episodes in a subset of patients. The most commonly implicated are:
- Cheese — particularly aged cheeses high in tyramine
- Chocolate — a classical migraine trigger, shared with CVS
- Monosodium glutamate (MSG) — food additive found in processed foods, fast food, and Asian cuisine
- Caffeine — both excess intake and caffeine withdrawal
- Fasting or prolonged intervals between meals — metabolic stress from hypoglycemia is a potent trigger, particularly in children
Sleep Disruption
Insufficient sleep, sleep deprivation, and disrupted circadian rhythms consistently trigger episodes. The mechanism likely involves both HPA axis dysregulation and melatonin/cortisol rhythm disruption. The characteristic early-morning episode onset in many CVS patients may relate to the nadir of cortisol suppression and the peak of melatonin withdrawal in the pre-dawn hours.
Cannabis
Chronic heavy cannabis use is a specific and increasingly recognized CVS trigger that produces a distinct clinical entity — Cannabis Hyperemesis Syndrome — described in detail in the next section.
Other Triggers
Additional reported triggers include: car travel and motion sickness, intense exercise, hot weather and heat exposure, overheating, strong odors, and allergic reactions. Many patients can identify their personal trigger profile with a symptom diary.
6. Cannabis Hyperemesis Syndrome
Cannabis Hyperemesis Syndrome (CHS) is a distinct clinical entity — a form of cyclic vomiting caused specifically by chronic, heavy cannabis use. As legalization and normalization of cannabis have expanded, CHS has emerged as a significant and frequently missed diagnosis in emergency departments. Understanding the distinction between CHS and classic CVS — and the unique pathognomonic features of CHS — is essential for appropriate management.
Definition and Mechanism
CHS occurs in a subset of long-term, daily or near-daily cannabis users who develop paradoxical hyperemesis despite cannabis's well-known acute antiemetic properties. The mechanism involves desensitization and downregulation of cannabinoid CB1 receptors in the enteric nervous system and brainstem with chronic heavy exposure. Acutely, cannabis activates CB1 receptors to suppress nausea; chronically, receptor downregulation reverses this effect, and the sympathomimetic and thermoregulatory properties of cannabinoids come to dominate. High-potency THC products (concentrates, dabs, edibles) accelerate the development of CHS.
The thermoregulatory aspect is central to CHS pathophysiology. Hypothalamic CB1 receptors normally help maintain core body temperature; their dysregulation in CHS leads to impaired thermoregulation, causing patients to feel subjectively overheated during episodes. This drives the compulsive hot showering behavior that is the clinical hallmark of CHS.
The Hot Shower Sign
The single most clinically distinctive feature of CHS — absent in classic CVS — is compulsive bathing in very hot water for prolonged periods during vomiting episodes. Patients report that immersion in scalding-hot showers or baths provides dramatic, near-complete temporary relief of nausea and vomiting, sometimes lasting 20–30 minutes after emerging. They return to the shower repeatedly throughout the episode — sometimes spending hours per day bathing. This behavior is pathognomonic for CHS.
The mechanism appears to be thermal cutaneous stimulation activating transient receptor potential vanilloid (TRPV1) channels in skin afferents, which override the dysregulated hypothalamic thermostat and temporarily restore normal thermoregulatory balance. Topical capsaicin applied to the abdomen has been shown to replicate this effect and is used as a diagnostic test and symptomatic bridge treatment in the emergency department.
CHS vs. Classic CVS: Key Distinctions
- Cannabis use history: CHS requires chronic heavy cannabis use (typically daily use for >1 year); classic CVS does not
- Compulsive hot showering: Pathognomonic for CHS; absent or rare in classic CVS
- Age of onset: CHS typically presents in young adults (20s–30s) who have been cannabis users since adolescence; classic CVS can present at any age
- Migraine history: 90% of classic CVS patients have migraine or family history; migraine association is less prominent in CHS
- Response to cannabis cessation: CHS resolves completely with sustained cannabis cessation; classic CVS is unaffected by cannabis use history
- Worsening with cannabis: CHS episodes are precipitated by cannabis use; patients with classic CVS may actually use cannabis to self-treat nausea (which is counterproductive in CHS)
Diagnosis and Emergency Management
CHS is diagnosed clinically based on the triad of: (1) chronic heavy cannabis use, (2) recurrent stereotyped vomiting episodes, and (3) relief with hot bathing. In the emergency department, topical capsaicin cream (0.075–0.1%) applied to the abdomen provides diagnostic confirmation and symptomatic relief — it is more effective than haloperidol alone for acute CHS and is now used in many emergency protocols. Haloperidol 5 mg IV has shown superior efficacy to ondansetron for CHS in randomized emergency department trials.
Definitive Treatment: Cannabis Cessation
The only definitive treatment for CHS is complete, sustained cannabis cessation. Symptoms typically resolve within 1–3 months of cessation in most patients, though some require up to 6 months. Partial reduction in cannabis use does not resolve CHS — complete abstinence is required. Relapse to cannabis use invariably results in recurrence of CHS. Patients should be counseled that all cannabis products — including CBD-dominant products containing trace THC — can maintain CHS in susceptible individuals. Cessation support, addiction counseling, and motivational interviewing are integral to CHS management.
7. Diagnosis
CVS diagnosis is clinical, based on recognition of the characteristic episodic pattern after exclusion of structural, metabolic, and surgical causes. There is no diagnostic test for CVS — the diagnosis is made by applying validated criteria to a careful history.
Rome IV Criteria
The Rome IV criteria (2016) are the current gold standard for diagnosing adult CVS. All of the following must be present:
- Stereotyped episodes of vomiting regarding onset (acute) and duration (less than 1 week)
- Three or more discrete episodes in the prior year
- Absence of vomiting between episodes — though other, milder symptoms (mild nausea, fatigue) may persist
- Symptoms not better explained by another diagnosis
Supportive criteria (not required but strengthen the diagnosis) include: a personal or family history of migraine, a predictable stereotyped onset time, the ability to abort episodes with sleep or triptans, and a stereotyped prodrome.
Differential Diagnosis
The key differential diagnoses that must be excluded before accepting a CVS diagnosis include:
- Gastroparesis: Delayed gastric emptying causes chronic nausea and intermittent vomiting, but symptoms are continuous rather than episodic, and symptom-free intervals do not occur. A gastric emptying study distinguishes the two conditions — CVS has normal gastric emptying during the interictal period.
- Functional nausea and vomiting: Functional dyspepsia and functional nausea present with chronic, persistent symptoms rather than discrete episodic attacks separated by complete normalcy.
- Small bowel obstruction: Intermittent obstruction from adhesions, internal hernias, or malrotation can mimic CVS. CT imaging or small bowel follow-through is indicated, particularly in patients with prior abdominal surgery.
- Pheochromocytoma: Episodic catecholamine release causes paroxysmal hypertension, diaphoresis, and vomiting that can closely mimic CVS. Plasma free metanephrines or 24-hour urine catecholamines are an essential part of the workup.
- Arnold-Chiari malformation: Type I Chiari malformation causes raised intracranial pressure, which can present with episodic vomiting, headache, and autonomic instability. Brain MRI with posterior fossa views is indicated.
- Addison's disease: Primary adrenal insufficiency produces episodic nausea, vomiting, and fatigue triggered by physiological stress — a potentially life-threatening mimic of CVS that requires cortisol and ACTH measurement.
- Mitochondrial disorders: MELAS (mitochondrial encephalomyopathy, lactic acidosis, and stroke-like episodes) and other mitochondrial diseases can present with recurrent vomiting. Lactate, pyruvate, and mitochondrial DNA testing should be considered in patients with suggestive systemic features.
Diagnostic Workup
The recommended workup for a patient presenting with recurrent stereotyped vomiting includes:
- Upper endoscopy (EGD): To exclude structural causes — peptic ulcer disease, outlet obstruction, eosinophilic esophagitis. Also evaluates for Mallory-Weiss tears from forceful vomiting.
- Gastric emptying scintigraphy: To exclude gastroparesis. Performed during the symptom-free interictal period — results are normal in CVS.
- Brain MRI with posterior fossa protocol: To exclude Arnold-Chiari malformation and intracranial lesions affecting the vomiting center.
- Abdominal CT or MRI: To exclude structural small bowel pathology, superior mesenteric artery (SMA) syndrome, and retroperitoneal masses.
- Metabolic screen: Plasma free metanephrines (pheochromocytoma), morning cortisol/ACTH stimulation test (Addison's disease), serum lactate/pyruvate (mitochondrial disease), urine organic acids.
- Cannabis use history: Explicit, non-judgmental inquiry about cannabis use history — frequency, duration, product type, quantity — is essential given the prevalence of CHS.
8. Abortive Treatment
Abortive therapy aims to interrupt an episode during the prodrome or early vomiting phase, shortening its duration and reducing its severity. The prodromal window of 30–60 minutes is the critical treatment opportunity.
Triptans (Sumatriptan)
Sumatriptan, a serotonin 5-HT1B/1D receptor agonist, is the most effective abortive agent for CVS, reflecting the condition's migrainous basis. Its mechanism — constriction of intracranial blood vessels and inhibition of trigeminovascular inflammatory peptides (CGRP, substance P) — directly targets the shared CVS-migraine pathophysiology. Subcutaneous sumatriptan (6 mg) is preferred over oral formulations during CVS episodes, because nausea and the high vomiting frequency make oral absorption unreliable. A nasal spray formulation (20 mg) is a useful intermediate option. Sumatriptan should be given at the first sign of the prodrome — before vomiting begins — to achieve maximum benefit. It is most effective in patients with a clear migrainous history.
Ondansetron
Ondansetron (4–8 mg orally, sublingually, or IV) is a 5-HT3 receptor antagonist antiemetic that reduces the intensity of nausea and the frequency of vomiting during established episodes. It does not abort episodes in the same way triptans do, but is an essential component of supportive care — reducing dehydration risk by allowing brief oral rehydration attempts, reducing distress, and reducing the need for IV hydration. Oral dissolving tablet (ODT) formulations are practical during episodes when the patient cannot swallow pills reliably.
Lorazepam
Lorazepam (0.5–1 mg orally or IV) serves multiple roles in CVS abortive therapy. As a benzodiazepine, it reduces anxiety and activates GABA receptors in the brainstem, which modulate the vomiting center. It produces sedation that allows the patient to sleep — and sleep is one of the most effective ways to terminate a CVS episode. It also has independent antiemetic properties and reduces the intense distress accompanying severe vomiting. The combination of lorazepam plus ondansetron is a standard emergency department regimen for acute CVS management.
Haloperidol (Refractory Episodes)
Haloperidol (0.05 mg/kg IV, typical dose 1–5 mg) is a typical antipsychotic with potent antiemetic properties mediated through dopamine D2 receptor blockade in the area postrema. It has emerged as a particularly effective agent for CVS and CHS episodes refractory to ondansetron and lorazepam. Multiple emergency department studies have demonstrated superior efficacy of IV haloperidol over standard antiemetics for acute CVS, particularly when episodes involve extreme vomiting frequency or severe distress. QTc monitoring is recommended, and akathisia (motor restlessness) can be managed with diphenhydramine pretreatment.
Intravenous Fluid Resuscitation
Dehydration is a universal complication of severe CVS episodes. IV fluid resuscitation with normal saline or lactated Ringer's solution — often including potassium supplementation for hypokalemia — is a mainstay of emergency department management. Many patients require 1–3 liters of IV fluid per episode. Dextrose-containing solutions may be preferred for patients with suspected mitochondrial disease, as fasting-induced metabolic stress may be a trigger. A dark, quiet room with minimal stimulation during IV infusion reduces sensory triggering of continued vomiting.
9. Prophylactic Treatment
Prophylactic (preventive) therapy is indicated for patients with frequent episodes (≥4/year), prolonged episodes (>3 days), significant disability, or episodes requiring emergency care. The goal is to reduce episode frequency, severity, and duration — not necessarily to eliminate all episodes.
Amitriptyline (First-Line Adults)
Amitriptyline is the first-line prophylactic agent for CVS in adults, endorsed by the 2019 multidisciplinary clinical practice guideline. It is a tricyclic antidepressant that modulates serotonergic and noradrenergic neurotransmission, reduces central sensitization, and has direct antiemetic properties through its anticholinergic and antihistamine effects. Starting doses of 10–25 mg at bedtime are titrated upward over weeks to 50–75 mg (or higher in adults without dose-limiting side effects). The sedating side effects (drowsiness, dry mouth) are often beneficial in CVS — promoting sleep, which is itself therapeutic. Clinical trials report episode frequency reductions of 50–75% in responders. The drug also treats comorbid anxiety and depression, which are prevalent in CVS populations. Amitriptyline is less commonly used in children due to cardiac side effect concerns; in pediatric CVS, cyproheptadine is often preferred.
Coenzyme Q10 (CoQ10)
Coenzyme Q10 (ubiquinol, 100–600 mg/day) is a mitochondrial cofactor that functions as an electron carrier in the respiratory chain. Its role in CVS prophylaxis is grounded in the mitochondrial dysfunction hypothesis. Several observational series and a pilot randomized trial have reported significant reductions in episode frequency with CoQ10 supplementation. It is particularly recommended for patients with evidence of mitochondrial involvement (maternal inheritance, exercise intolerance, elevated lactate) and as an adjunct to first-line pharmacological prophylaxis. CoQ10 has an excellent safety profile and is well tolerated.
Riboflavin (Vitamin B2)
Riboflavin (vitamin B2) at doses of 200–400 mg/day supports mitochondrial complex I and II function and has established efficacy in migraine prophylaxis. Its use in CVS is extrapolated from the shared mitochondrial and migrainous mechanisms. Riboflavin is inexpensive, safe, and well tolerated — side effects are limited to harmless bright-yellow urine discoloration. It is commonly combined with CoQ10 as a mitochondrial support regimen, particularly in patients with a strong migrainous or mitochondrial profile.
L-Carnitine
L-Carnitine (50–100 mg/kg/day, maximum 3 g/day) facilitates the transport of long-chain fatty acids into mitochondria for beta-oxidation and plays a role in buffering the acetyl-CoA pool during metabolic stress. In CVS patients with evidence of carnitine deficiency or mitochondrial dysfunction, L-carnitine supplementation may reduce episode frequency. It is particularly used in pediatric CVS and in adult patients with a mitochondrial phenotype. Plasma carnitine levels can be measured to identify deficiency before initiating supplementation.
Topiramate
Topiramate (25–100 mg/day) is an alternative prophylactic agent for CVS patients who fail or cannot tolerate amitriptyline. It is a sodium channel blocker and GABA agonist with proven efficacy in migraine prophylaxis that translates to CVS through shared mechanisms. Its main limitations are cognitive side effects ("word-finding difficulties," slowed thinking) and weight loss, which can be problematic in patients already prone to nutritional deficits from repeated vomiting episodes. Topiramate is preferred over amitriptyline in patients with obesity or in those for whom the anticholinergic side effects of tricyclics are poorly tolerated.
Behavioral and Lifestyle Prophylaxis
Non-pharmacological prophylaxis is integral to CVS management. Key strategies include:
- Trigger avoidance: Personalized trigger diary to identify and systematically reduce exposure to individual triggers (dietary, sleep, stress)
- Regular sleep schedule: Maintaining consistent sleep and wake times reduces circadian dysregulation — one of the most modifiable risk factors
- Regular meals: Avoiding fasting; carrying snacks to prevent hypoglycemia-triggered episodes
- Stress management: Cognitive-behavioral therapy, biofeedback, and mindfulness-based interventions reduce the HPA axis hyperreactivity that drives stress-triggered episodes
- Cannabis cessation: Mandatory for patients with CHS; also recommended for classic CVS patients who use cannabis to self-treat, as this may worsen long-term course
10. Complications
- Dehydration and electrolyte abnormalities: The most immediate and universal complication. Severe vomiting produces hypokalemia (potassium depletion from gastric losses), hyponatremia (from hypotonic fluid replacement), and metabolic alkalosis (from loss of hydrochloric acid). Severe dehydration can cause prerenal azotemia, orthostatic hypotension, and in extreme cases, cardiovascular compromise. IV fluid resuscitation with electrolyte correction is the cornerstone of emergency management.
- Mallory-Weiss tears: Forceful retching during CVS episodes can produce longitudinal mucosal lacerations at the gastroesophageal junction — Mallory-Weiss tears — causing hematemesis (vomiting blood). These tears are typically self-limiting and heal spontaneously, but can cause significant alarming bleeding during an already-distressing episode. Severe or persistent hematemesis warrants urgent endoscopy.
- Boerhaave syndrome (esophageal rupture): Extremely rare but life-threatening complication of explosive vomiting — full-thickness esophageal perforation causing mediastinitis. Presents with severe chest pain, subcutaneous emphysema, and rapidly developing sepsis after a vomiting episode. Requires emergency surgical consultation.
- Dental erosion: Repeated exposure of tooth enamel to gastric acid during frequent vomiting episodes causes progressive erosion of the lingual (tongue-side) surfaces of the upper teeth — the characteristic pattern of acid reflux injury. Dental referral and fluoride protection should be part of long-term CVS management.
- Nutritional deficiencies: Frequent prolonged vomiting episodes — each lasting several days with inability to eat — cumulatively produce caloric, protein, and micronutrient deficits over time. Thiamine (B1) deficiency is a specific risk in patients with frequent and severe episodes, because thiamine stores are limited and depletion can occur within days of reduced intake. Wernicke's encephalopathy (ataxia, ophthalmoplegia, confusion) from thiamine deficiency is a rare but documented complication of severe CVS and should be treated empirically with IV thiamine in any CVS patient presenting with altered mental status.
- School and work absenteeism: CVS episodes, each lasting a mean of 5 days and occurring multiple times per year, produce substantial functional impairment. Children with CVS miss a mean of 24 school days per year — well above the threshold for educational impact. Adults lose a mean of 22 workdays per year. Academic failure, social isolation, and reduced career opportunity are recognized long-term consequences of inadequately treated CVS.
- Psychological impact and psychiatric comorbidity: The chronic unpredictable nature of CVS — with its dramatic, debilitating attacks arising at random and disrupting normal life — produces significant psychological burden. Rates of anxiety disorders (40–50%), depression (25–35%), and health anxiety are substantially elevated in CVS populations. Anticipatory anxiety about the next episode further amplifies sympathetic nervous system activation, potentially increasing episode frequency in a vicious cycle. Psychological support should be a routine component of comprehensive CVS care.
- Opiate dependence: Prior to the recognition of CVS as a distinct entity and the codification of effective treatments, patients frequently received repeated courses of IV opiates during emergency visits. Long-term opiate use for CVS pain management has produced opiate dependence in a significant number of patients, complicating subsequent care. Current guidelines recommend against routine opiate use for CVS and emphasize non-opiate management protocols in emergency settings.
11. Prognosis and Long-term Outcomes
The long-term prognosis of CVS is variable and depends heavily on age of onset, the underlying mechanism, and the adequacy of prophylactic treatment.
Childhood CVS: Transition to Migraine
A defining feature of pediatric CVS is its frequent natural evolution over time. Longitudinal studies show that approximately 50–75% of children with CVS experience resolution or significant reduction of vomiting episodes in adulthood, but the majority of these children go on to develop classic migraine headaches as adolescents or young adults. The vomiting syndrome transforms into a headache syndrome as the clinical expression of the same underlying neurological predisposition shifts with neurodevelopment. This transition is an important finding to discuss with families at diagnosis — CVS in childhood is not a lifelong vomiting disorder in most patients, but a precursor to migraine that requires the same preventive approach.
A minority of children (approximately 20–30%) continue to experience CVS episodes into adulthood without transitioning to headache-predominant migraine, and a small subset develop concurrent migraine headaches alongside persistent CVS episodes.
Adult CVS: Chronic Course
Adult-onset CVS tends to follow a more persistent course without the natural remission seen in childhood CVS. Adults diagnosed in their 20s and 30s — particularly those with a strong CRF/stress-trigger pattern or mitochondrial features — commonly experience ongoing episodic disease for years to decades. With appropriate prophylactic therapy (amitriptyline first-line), approximately 50–75% of adults achieve a clinically meaningful reduction in episode frequency and severity. Complete remission is achievable but less common in adults than in children.
Prognostic Factors
Features associated with better long-term prognosis include: childhood onset, strong migrainous profile (good response to triptans), compliance with prophylactic therapy, successful trigger identification and avoidance, and absence of psychiatric comorbidity. Features associated with worse prognosis include: adult onset, psychiatric comorbidity (particularly anxiety disorders), cannabis use continuation, opiate dependence, frequent emergency department visits as a pattern of care, and late or missed diagnosis (delaying effective prophylaxis).
For patients with CHS, the prognosis following complete cannabis cessation is excellent — the vast majority experience full resolution of episodes within 1–3 months and remain episode-free indefinitely as long as cannabis abstinence is maintained.
12. References
- Search PubMed — North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition consensus statement on the diagnosis and management of cyclic vomiting syndrome. J Pediatr Gastroenterol Nutr. 2008;47(3):379-393.
- Search PubMed — Functional vomiting disorders in adults: cyclic vomiting syndrome and cannabinoid hyperemesis syndrome. Curr Gastroenterol Rep. 2014;16(6):392.
- Search PubMed — Gastroduodenal disorders. Gastroenterology. 2016;150(6):1380-1392. [Rome IV functional gastroduodenal disorders]
- Search PubMed — Idiopathic cyclic nausea and vomiting — a disorder of gastrointestinal motility? Mayo Clin Proc. 2008;63(12):1169-1175.
- Search PubMed — Role of chronic cannabis use: cyclic vomiting syndrome vs cannabinoid hyperemesis syndrome. Neurogastroenterol Motil. 2019;31(Suppl 2):e13606. [2019 multidisciplinary clinical practice guideline CVS]
- Search PubMed — Hypnosis as an adjuvant treatment for children with inflammatory bowel disease and cyclic vomiting syndrome. J Dev Behav Pediatr. 2004;25(6):442-448.
- Search PubMed — Cyclic vomiting syndrome in 41 adults: the illness, the patients, and problems of management. BMC Med. 2005;3:20.
- Search PubMed — Review article: cyclic vomiting syndrome in adults — rediscovering and redefining an old entity. Aliment Pharmacol Ther. 2011;34(3):263-273.
- Search PubMed — Maternal inheritance in cyclic vomiting syndrome. Am J Med Genet A. 2005;133A(1):71-77. [Mitochondrial DNA variants in CVS]
- Search PubMed — A pilot study of amitriptyline for cyclic vomiting syndrome: pilot results. J Pediatr Gastroenterol Nutr. 2010;50(2):E62-63.
- Search PubMed — Serotonin syndrome in children: a systematic review. Front Neurol. 2020;10:1300. [Emergency management of cyclic vomiting in children]
- Search PubMed — Cannabinoid hyperemesis: cyclical hyperemesis in association with chronic cannabis abuse. Gut. 2017;53(11):1566-1570. [Systematic review of cannabis hyperemesis syndrome]
Connections
- Gastroenterology
- Gastroparesis
- Gastroesophageal Reflux Disease
- Irritable Bowel Syndrome
- Functional Dyspepsia
- Peptic Ulcer Disease
- Pancreatitis
- All Conditions
- Riboflavin (Vitamin B2)
- L-Carnitine