PCOS (Polycystic Ovary Syndrome): History and Discovery
Polycystic ovary syndrome is one of medicine's oldest puzzles and one of its most actively renamed. Enlarged, abnormal ovaries were sketched by anatomists as far back as Antonio Vallisneri in 1721, but the modern syndrome dates to 1935, when the Chicago gynecologists Irving F. Stein and Michael L. Leventhal described seven women sharing absent periods, excess body hair, obesity, and enlarged polycystic ovaries — the cluster that became "Stein-Leventhal syndrome." For decades it was seen as a reproductive disorder of the ovary. That changed in 1980, when Burghen, Givens, and Kitabchi linked it to insulin resistance, reframing it as a metabolic as well as reproductive condition. The Rotterdam criteria (2003) standardized who counts as having it. Today the name itself is on trial: the "cysts" are not true cysts but arrested egg follicles, and in 2026 an international consensus proposed renaming the condition entirely. This page traces that long arc — and flags clearly where history is solid and where it is still being written.
Table of Contents
- What PCOS Is, and Why Its History Is Confusing
- Early Anatomy: Vallisneri (1721) and the 19th-Century Pathologists
- Stein and Leventhal, 1935: The Syndrome Named
- Wedge Resection: The First Treatment
- From "Stein-Leventhal" to "Polycystic Ovary Syndrome"
- 1980: The Insulin-Resistance Revolution
- Defining the Diagnosis: NIH 1990 and Rotterdam 2003
- A Misnomer on Trial: The Renaming Debate
- Legacy: From Ovarian Curiosity to Whole-Body Syndrome
- Research Papers and References
- Connections
- Featured Videos
What PCOS Is, and Why Its History Is Confusing
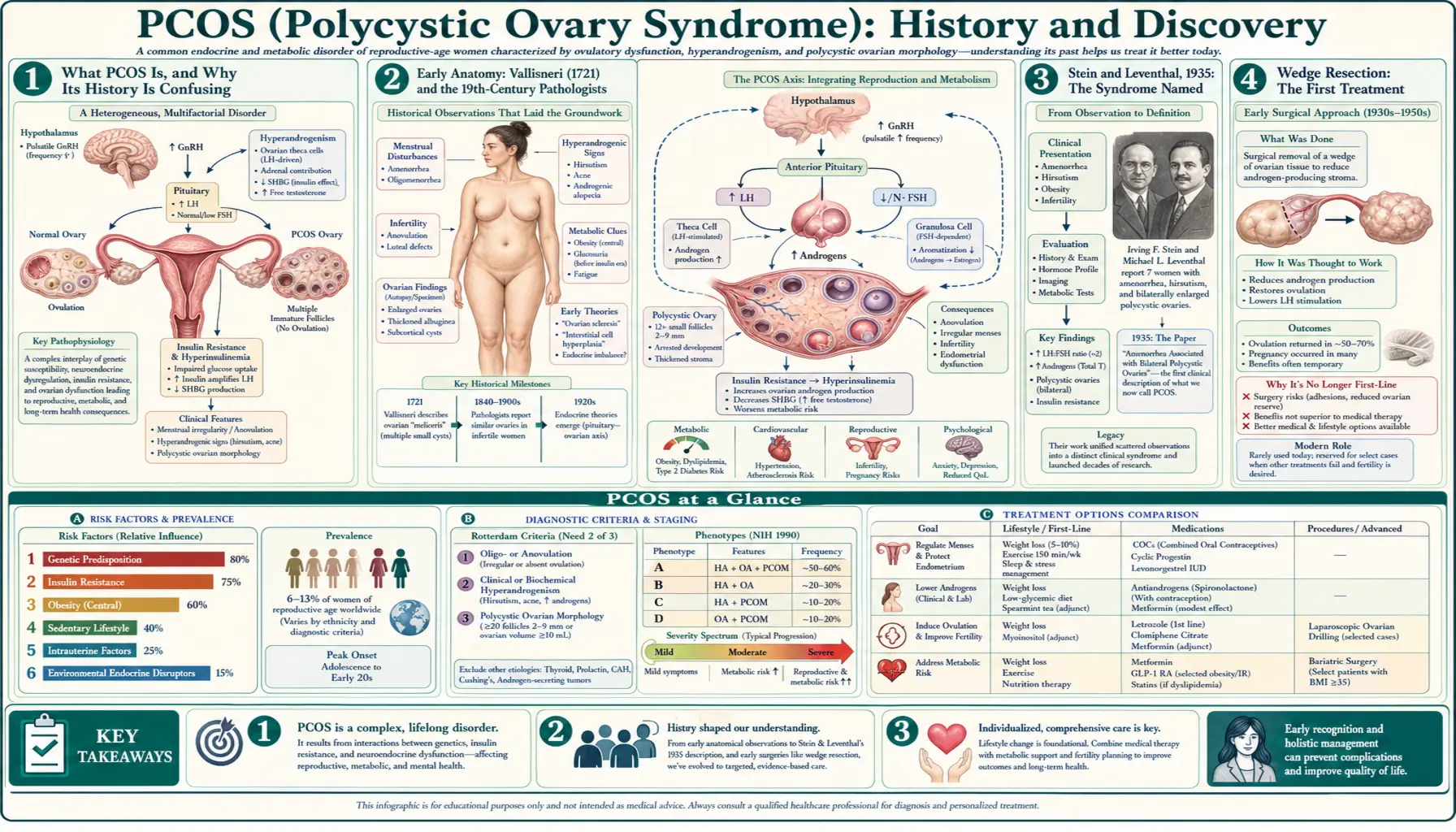
Polycystic ovary syndrome (PCOS) is the most common hormonal disorder of women of reproductive age, affecting an estimated one in eight to one in ten. Its core features are irregular or absent ovulation, signs of excess male-type hormones (androgens) such as unwanted facial and body hair (hirsutism) and acne, and ovaries that on ultrasound carry many small fluid-filled sacs around their rim. It is closely tied to insulin resistance, weight gain, and a raised long-term risk of type 2 diabetes and metabolic disease. Yet none of these features is universal, which is exactly why the condition's history is so tangled: different doctors in different eras saw different faces of the same disorder.
Understanding the history requires keeping three distinct threads separate, because they are often blurred together. The first is the anatomical observation — the centuries-old recognition that some infertile women have enlarged, cyst-studded ovaries. The second is the clinical syndrome — Stein and Leventhal's 1935 insight that a specific group of symptoms travels together. The third is the underlying mechanism — the much later discovery that insulin resistance sits near the center of it. A discovery in one thread is not the same as a discovery in another, and conflating them is the single most common error in popular accounts of PCOS history.
This page keeps those threads apart and is careful about what counts as a verified "first." Where a name, a date, or a priority claim rests on solid primary or scholarly sources, it is stated plainly. Where the historical record is partial — as with the earliest anatomical sightings — that uncertainty is named rather than smoothed over. The aim is an honest account of how a roadside anatomical curiosity became one of the most studied endocrine syndromes in the world.
Early Anatomy: Vallisneri (1721) and the 19th-Century Pathologists
Long before anyone spoke of a "syndrome," anatomists noticed that certain women who could not conceive had strikingly abnormal ovaries. The most frequently cited early description belongs to the Italian scientist Antonio Vallisneri, who in 1721 recorded the case of a young, married, infertile peasant woman whose ovaries were larger than normal, shiny, with a smooth whitish surface, and — in his memorable comparison — about the size of pigeon (dove) eggs. This is widely regarded by historians of the syndrome as the earliest clear anatomical account of what would later be called polycystic ovaries, though it is an observation of structure, not a description of the clinical syndrome.
Through the nineteenth century, pathologists added to the picture as the microscope and systematic post-mortem study matured. The French physician Achille Chereau is credited with describing sclerocystic (hardened, cyst-bearing) changes of the ovary in 1844, and other European anatomists of the era catalogued enlarged, thick-walled, multi-cystic ovaries in women with menstrual disturbance. These reports established, piece by piece, that a recognizable abnormal ovarian morphology existed; what they could not do, without the hormonal science of the next century, was explain it or tie it reliably to a living patient's symptoms.
A word of historical caution is warranted. The oldest priority claims in any field tend to accrete embellishment as they are retold, and details of these early cases are thin by modern standards. The Vallisneri (1721) and Chereau (1844) attributions are reported consistently across modern scholarly histories of PCOS and are presented on that basis — well-attested landmarks in the anatomical thread of the story, not descriptions of the syndrome itself, which arrived only in 1935.
Stein and Leventhal, 1935: The Syndrome Named
The decisive moment in PCOS history is firmly dated and well documented. In 1935, two gynecologists at Michael Reese Hospital and Northwestern University Medical School in Chicago — Irving Freiler Stein, Sr. and Michael Leo Leventhal — published Amenorrhea associated with bilateral polycystic ovaries in the American Journal of Obstetrics and Gynecology (1935;29:181–185). The work had been presented the previous autumn at the meeting of the Central Association of Obstetricians and Gynecologists held in New Orleans on November 1–3, 1934. Their crucial contribution was not the cysts, which others had seen, but the recognition of a pattern.
Stein and Leventhal described a series of seven women who shared a recurring constellation: absent or irregular menstruation (amenorrhea or oligomenorrhea), excessive body and facial hair (hirsutism), in many cases obesity, and enlarged ovaries packed with multiple small follicular cysts. Reporting a series rather than isolated case reports was what mattered: it transformed a scattering of separate observations — polycystic ovaries here, hirsutism there, missed periods elsewhere — into a single, reproducible clinical entity. Because of this, the condition was named after them as the Stein-Leventhal syndrome, a label still used today as a historical synonym for PCOS.
It is worth being precise about priority. Stein and Leventhal did not discover polycystic ovaries (Vallisneri and the nineteenth-century pathologists had described the anatomy), and they did not uncover the cause (the insulin link lay decades ahead). What they did, and what justifies their eponym, was to define the syndrome — to show that these features cluster non-randomly in living patients and to give clinicians a recognizable diagnosis. In the careful framing used throughout this page, theirs is the founding description of the clinical syndrome, distinct from the older anatomical sightings and the later mechanistic discoveries.
Wedge Resection: The First Treatment
Stein and Leventhal's 1935 paper is remembered for a second reason: it introduced the first effective treatment. Reasoning that the thick-walled, enlarged ovary was mechanically and hormonally obstructing normal ovulation, they performed bilateral ovarian wedge resection — surgically removing a wedge-shaped portion of each ovary to reduce its bulk. In their original series the results were striking by the standards of the day: regular menstrual cycles reportedly returned in all seven women after surgery, and two of them subsequently became pregnant. For an era with no hormonal therapy for anovulation, this was a genuine therapeutic breakthrough.
Ovarian wedge resection became a standard operation for the syndrome for roughly the next four decades. We now understand its likely mechanism better than its originators could: removing or destroying a portion of androgen-producing ovarian tissue temporarily lowers circulating androgens and can restart ovulation. But the procedure carried real costs — it was major abdominal surgery, and it could cause pelvic adhesions (scar tissue) that themselves impaired fertility, an irony for an operation done largely to help women conceive.
Wedge resection faded from routine use as gentler options emerged: ovulation-inducing drugs such as clomiphene citrate from the 1960s, and later laparoscopic "ovarian drilling," a minimally invasive descendant that uses heat or laser to puncture the ovarian surface in a few spots rather than cutting away tissue. The arc from wedge resection to drug therapy to keyhole drilling mirrors the broader shift in PCOS care — away from treating the ovary as a mechanical problem and toward treating the hormonal and metabolic disturbance behind it.
From "Stein-Leventhal" to "Polycystic Ovary Syndrome"
For a generation after 1935 the disorder was known chiefly by its eponym, the Stein-Leventhal syndrome. As physiology advanced through the mid-twentieth century, the descriptive term polycystic ovary syndrome (and the related "polycystic ovarian disease," PCOD) gradually took over, because it named the most visible anatomical feature rather than its discoverers. The shift tracked a deeper change in how the condition was understood: from a surgically managed ovarian abnormality toward a systemic endocrine disorder.
Two mid-century currents drove this. First, hormone measurement matured: by the 1960s and 1970s clinicians could document elevated androgens and the characteristically skewed pituitary signaling (a raised ratio of luteinizing hormone to follicle-stimulating hormone) that accompany the syndrome, anchoring it in measurable endocrinology rather than surgical impression alone. Second, imaging arrived: pelvic ultrasound, refined through the 1980s, let doctors see the multifollicular ovary in a living patient without surgery, making "polycystic ovaries" an observable clinical sign and cementing the descriptive name.
By the time formal diagnostic criteria were drawn up at the close of the twentieth century, "polycystic ovary syndrome" was the standard term and "Stein-Leventhal syndrome" had become a respected historical synonym. As the next sections show, that descriptive victory carried a hidden problem: the word at the heart of the name — cystic — turns out to describe the ovary inaccurately, a tension that would eventually fuel a serious movement to rename the disease.
1980: The Insulin-Resistance Revolution
For its first forty-five years, PCOS was treated essentially as a disorder of the ovary and the reproductive axis. That picture was upended in 1980, when G. A. Burghen, J. R. Givens, and A. E. Kitabchi published Correlation of hyperandrogenism with hyperinsulinism in polycystic ovarian disease in the Journal of Clinical Endocrinology & Metabolism (1980;50(1):113–116). Studying obese women with PCOD against obese controls, they found that the patients had significantly higher circulating insulin, and that insulin levels correlated with androgen levels. The implication was profound: the syndrome was not confined to the ovary at all but was entangled with the body's handling of insulin and glucose.
This observation seeded what became the dominant modern understanding of PCOS as a metabolic as well as a reproductive disorder. The leading hypothesis that grew from it — and it should be read explicitly as a hypothesis, a model that organizes the evidence rather than a closed case — runs roughly as follows: many women with PCOS have insulin resistance, so the pancreas compensates by secreting more insulin (hyperinsulinemia); the excess insulin acts on the ovary and the liver to push androgen production up and to lower a carrier protein (sex-hormone-binding globulin), raising free androgen levels; and those androgens disrupt the orderly maturation of egg follicles, producing the arrested follicles, irregular ovulation, and outward signs of androgen excess. The precise weighting of cause and effect, and how much is genetic versus acquired, remains under active investigation.
The clinical consequences of this reframing have been enormous. It explains why PCOS clusters with obesity, type 2 diabetes, and metabolic syndrome; why weight loss and exercise can restore ovulation; why metformin, an insulin-sensitizing drug, entered PCOS care in the 1990s; and why a reproductive diagnosis is now routinely paired with screening for glucose intolerance and cardiovascular risk. The 1980 insulin link did not replace Stein and Leventhal's syndrome; it revealed the metabolic engine running beneath it.
Defining the Diagnosis: NIH 1990 and Rotterdam 2003
A syndrome with such varied features needs agreed rules for who has it, and for most of the twentieth century those rules did not formally exist — diagnosis rested on clinical judgment. The first attempt at consensus came from a National Institutes of Health conference (sponsored by the NICHD) on April 16–18, 1990. The resulting NIH 1990 criteria, articulated by Zawadski and Dunaif, defined PCOS by the combination of clinical and/or biochemical hyperandrogenism and chronic anovulation, after excluding other conditions that mimic it (such as thyroid disease, hyperprolactinemia, and congenital adrenal hyperplasia). Notably, ovarian appearance on ultrasound was not required.
The most influential framework arrived thirteen years later. At an ESHRE/ASRM-sponsored consensus workshop in Rotterdam, the Netherlands, in 2003, experts broadened the definition. The Rotterdam criteria require two of three features — (1) oligo- or anovulation, (2) clinical and/or biochemical hyperandrogenism, and (3) polycystic ovaries on ultrasound — again with other disorders excluded. Because only two of three are needed, Rotterdam recognizes several "phenotypes," including women with polycystic ovaries and irregular cycles but no overt androgen excess, widening the diagnosable population well beyond the stricter NIH definition. The consensus was published as Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (Fertil Steril 2004;81(1):19–25; companion report Hum Reprod 2004;19(1):41–47).
The Rotterdam criteria became the most widely used standard in research and practice and remain influential, though not the last word. Later refinements — the Androgen Excess and PCOS Society's 2006 position that androgen excess should be central, and subsequent international guidelines updating follicle-count thresholds and adding anti-Mullerian hormone (AMH) — show that defining PCOS is a living, contested process. Each revision changes how many women carry the label, one practical reason the syndrome's name and boundaries are still debated.
A Misnomer on Trial: The Renaming Debate
One of the most important facts about "polycystic ovary syndrome" is that the name is, in a strict sense, wrong — and this is not a fringe complaint but a mainstream criticism. The structures that ultrasound reveals around the ovarian rim are not true cysts (fluid-filled pathological sacs). They are ordinary egg follicles arrested in early development, halted before any one of them matures and releases an egg. Many women diagnosed with the syndrome do not even have these visible follicles, and conversely, polycystic-appearing ovaries can occur in women without the syndrome. The name highlights a feature that is neither necessary nor truly "cystic."
Critics have long argued the name does real harm: it focuses attention on the ovary and on "cysts" while obscuring the metabolic dimension uncovered in 1980, and it can frighten and confuse patients who are told they have ovarian cysts they do not have. Calls to rename the condition gathered momentum in the 2010s — an NIH-sponsored evidence-based methodology workshop in 2012 explicitly identified the name as a barrier to progress and urged change — but for years no replacement achieved consensus, and "PCOS" persisted by sheer inertia.
That impasse appears to have broken recently, and this is current, fast-moving news that readers should treat as developing rather than settled history. In 2026, following a multi-year international consensus process, a proposal published in The Lancet recommended renaming the condition polyendocrine metabolic ovarian syndrome (PMOS) — a term chosen to capture its multisystem, hormonal-and-metabolic nature and to drop the misleading "cystic." Reports describe endorsement by dozens of professional and patient organizations. How quickly "PMOS" replaces "PCOS" in clinics, coding systems, and everyday speech remains to be seen; for now both terms are in use, and this site notes the change while retaining the familiar "PCOS" for clarity. The honest summary is that the naming of this disorder is, in 2026, still being decided.
Legacy: From Ovarian Curiosity to Whole-Body Syndrome
The history of PCOS is a model of how medical understanding deepens in layers. An anatomical curiosity (Vallisneri, 1721; the nineteenth-century pathologists) became a defined clinical syndrome (Stein and Leventhal, 1935), which was then revealed to have a metabolic engine (Burghen, Givens, and Kitabchi, 1980), and finally a standardized, contested definition (NIH 1990; Rotterdam 2003 and beyond). Each layer did not erase the one before; it added depth. The woman with enlarged ovaries Vallisneri described three centuries ago and the woman screened today for insulin resistance and offered an evidence-based guideline are recognizably the same patient, seen through ever-sharper lenses.
That trajectory has reshaped care in concrete, checkable ways. PCOS is no longer managed as a surgical problem of the ovary but as a lifelong condition spanning gynecology, endocrinology, and metabolic medicine: ovulation induction for those seeking pregnancy, but also weight management, insulin-sensitizing therapy, screening for diabetes and cardiovascular risk, and attention to the anxiety, depression, and quality-of-life burden the syndrome carries. The 1980 insulin insight, in particular, turned a fertility diagnosis into a whole-body health concern that follows women across the lifespan.
It is fitting that a disorder whose history is one of repeated reframing should end this account with its own name in question. The very fact that a condition first sketched in 1721 and named in 1935 is being formally rechristened in 2026 is the clearest possible sign that PCOS is not a closed chapter but an open field. For patients, the practical message is steadying: whatever it is ultimately called, this is one of the best-studied hormonal conditions in medicine, and the centuries of work traced here have produced real, effective ways to manage it.
Research Papers and References
The list below combines landmark primary papers in the history of PCOS with curated PubMed topic-search links into the broader literature. Where a stable DOI or PubMed identifier is available and verified it is given directly; the remaining entries are topic searches that open at PubMed (U.S. National Library of Medicine) in a new tab. The earliest anatomical accounts (Vallisneri, 1721; Chereau, 1844) are named in the article as historical sources documented through modern scholarly histories rather than as directly linkable papers.
- Stein IF, Leventhal ML. Amenorrhea associated with bilateral polycystic ovaries. American Journal of Obstetrics and Gynecology. 1935;29:181–185. (Founding description of the clinical syndrome; ovarian wedge resection.) — PubMed: Stein and Leventhal 1935
- Burghen GA, Givens JR, Kitabchi AE. Correlation of hyperandrogenism with hyperinsulinism in polycystic ovarian disease. Journal of Clinical Endocrinology & Metabolism. 1980;50(1):113–116. (Landmark insulin–androgen link.) — doi:10.1210/jcem-50-1-113
- Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Fertility and Sterility. 2004;81(1):19–25. — doi:10.1016/j.fertnstert.2003.10.004
- Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Human Reproduction. 2004;19(1):41–47. (Companion publication; PMID 14711538.) — PubMed: Rotterdam 2003 consensus
- Kotlyar AM, Seifer DB. The polycystic ovary syndrome: the first 150 years of study. F&S Reports. 2023. (Scholarly history covering Vallisneri, Chereau, Stein-Leventhal, and after.) — PubMed: PCOS the first 150 years of study
- History of discovery of polycystic ovary syndrome. Advances in Clinical and Experimental Medicine. 2017;26(3):555–558. — doi:10.17219/acem/61987
- Azziz R, Adashi EY, et al. Stein and Leventhal: 80 years on. American Journal of Obstetrics and Gynecology. 2016. (Historical retrospective; PMID 26704896.) — PubMed: Stein and Leventhal 80 years on
- NIH/NICHD 1990 diagnostic criteria for PCOS (Zawadski and Dunaif; hyperandrogenism + chronic anovulation, with exclusions) — PubMed: NIH 1990 PCOS criteria
- Diagnostic criteria for polycystic ovary syndrome: a reappraisal (comparison of NIH 1990 and Rotterdam 2003 criteria) — PubMed: PCOS diagnostic criteria reappraisal
- Androgen Excess and PCOS Society criteria / phenotypes of PCOS — PubMed: Androgen Excess and PCOS Society criteria
- Insulin resistance and hyperinsulinemia in the pathogenesis of PCOS (mechanism reviews) — PubMed: insulin resistance in PCOS pathogenesis
- Metformin and insulin-sensitizing therapy in PCOS — PubMed: metformin in PCOS
- Ovarian wedge resection and laparoscopic ovarian drilling in PCOS (history and outcomes) — PubMed: ovarian wedge resection and drilling
- Renaming polycystic ovary syndrome — the "cyst" misnomer and proposed new nomenclature — PubMed: renaming polycystic ovary syndrome
External Authoritative Resources
- NICHD (NIH) — Polycystic Ovary Syndrome
- MedlinePlus — Polycystic Ovary Syndrome
- PubMed — History of polycystic ovary syndrome
Connections
- Endocrinology
- PCOS (Polycystic Ovary Syndrome)
- Insulin Resistance
- Metabolic Syndrome
- Obesity
- Infertility
- Ovarian Cysts
- All Conditions