Hyperparathyroidism: History and Discovery
The story of hyperparathyroidism is unusual in medicine because it begins not with a disease but with the discovery of an organ that almost everyone had missed. The four parathyroid glands — each about the size of a grain of rice, tucked behind the thyroid — were the last major organ in the human body to be described, identified by a Swedish medical student named Ivar Viktor Sandström in 1880. Only afterward did physicians slowly connect these tiny glands to brittle bones, kidney stones, and a strange constellation of complaints, and only in 1925 did a surgeon in Vienna first cure the disease by removing an overactive gland. This page traces that history: who found the glands, who worked out what they do, who first named the bone disease, who performed the first operation, and how a single famous patient pushed an entire field forward. Throughout, care is taken to separate the discovery of the gland from the characterization of the disease and from the first surgery — three distinct milestones that are easy to blur together.
Table of Contents
- The Last Organ to Be Discovered
- Ivar Sandström and the Glandulae Parathyroideae (1880)
- Working Out the Function: Tetany and Calcium
- Naming the Bone Disease: von Recklinghausen (1891)
- The First Parathyroidectomy: Felix Mandl (1925)
- The Case of Captain Charles Martell
- Fuller Albright and the Modern Understanding
- Isolating the Hormone and the Modern Era
- "Stones, Bones, Groans, and Moans"
- Research Papers and References
- Connections
- Featured Videos
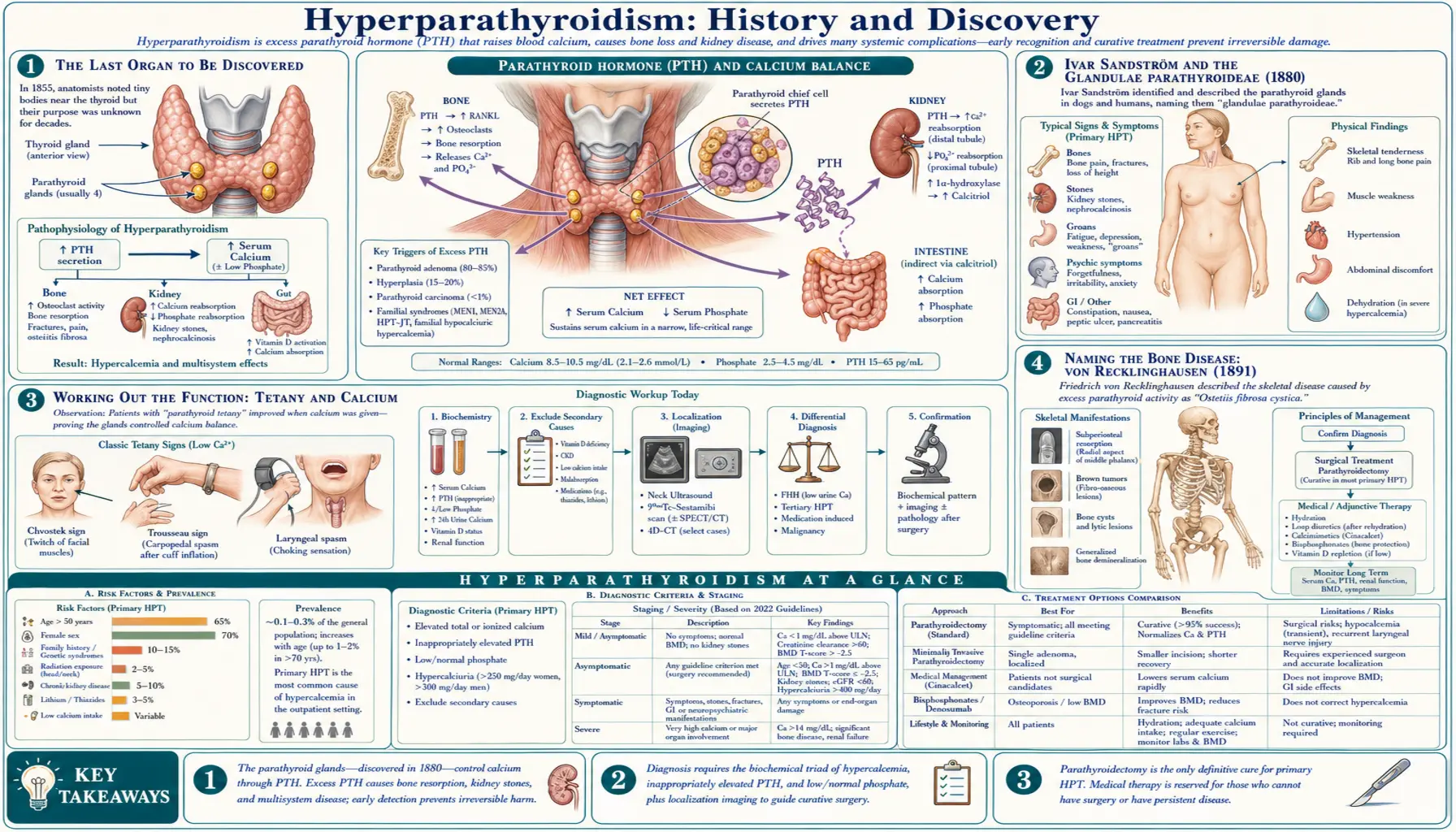
The Last Organ to Be Discovered
By the second half of the nineteenth century, anatomists believed they had mapped the human body in full. The heart, brain, liver, kidneys, thyroid, and the rest had been described, dissected, and drawn for centuries. It is therefore remarkable that one set of organs — small, pale, and easily mistaken for fat or for stray bits of thyroid tissue — escaped systematic notice until 1880. The parathyroid glands are usually four in number, two pairs riding on the back surface of the thyroid in the neck, and each is only a few millimetres across. Their size, their inconstant position, and their close resemblance to surrounding tissue all conspired to keep them hidden in plain sight.
There is one earlier sighting worth crediting honestly. The eminent English comparative anatomist Sir Richard Owen encountered the gland not in a human but in a Great Indian rhinoceros (Rhinoceros unicornis) that had died at the Zoological Society of London in November 1849. Dissecting the animal over the following winter, Owen described "a small compact yellow glandular body attached to the thyroid at the point where the vein emerged" — a recognizable parathyroid. His account, however, was not published until 1862, was buried in a long monograph on the rhinoceros, and was never connected to human anatomy or to any disease. For that reason historians of medicine treat Owen's note as the first recorded observation of the gland in an animal, while reserving the credit for its true discovery — a deliberate, systematic description in humans — for the man who came three decades later.
Ivar Sandström and the Glandulae Parathyroideae (1880)
Ivar Viktor Sandström (1852–1889) was a Swedish medical student at the University of Uppsala when he made the discovery that secured his small but permanent place in the history of medicine. Working as an assistant in the Anatomical Department, he noticed, around 1877, a small glandular structure attached to the thyroid in a dog. Rather than dismiss it, he pursued it methodically: he repeated the dissection in many animals — rabbits, cats, oxen, horses, and others — and finally in human cadavers, establishing that these little bodies were a consistent, normal feature of the anatomy and not a chance anomaly. This systematic, comparative confirmation is exactly what distinguishes a genuine discovery from a passing observation.
Sandström published his findings in 1880 in a Swedish journal, Upsala Läkareförenings Förhandlingar, in a paper whose title translates as "On a New Gland in Man and Several Animals." Believing the structures might be embryonic remnants related to the thyroid, he proposed the name they still carry today: glandulae parathyroideae — the parathyroid glands, literally "the glands beside the thyroid." Because he published in Swedish, in a regional journal, his work attracted little immediate international attention, and he did not live to see its importance recognized; he died in 1889. Yet his careful descriptions and his enduring name make the parathyroid glands, by common reckoning, the last major organ of the human body to be discovered.
Working Out the Function: Tetany and Calcium
Discovering an organ is not the same as understanding what it does, and the function of the parathyroids took another generation to unravel. The crucial early clues came from surgery on the neighbouring thyroid. As thyroid operations became more common in the late nineteenth century, surgeons sometimes saw patients develop a frightening complication afterward: tetany — painful muscle spasms, cramping of the hands and feet, and in severe cases convulsions and death. At first this was blamed on loss of the thyroid itself, but the picture did not quite fit.
The French physiologist Eugène Gley is generally credited with the decisive insight, published in 1891. Through careful animal experiments he showed that tetany followed not from removing the thyroid but specifically from removing or damaging the small glands Sandström had described; if the parathyroids were spared, the animals did not develop tetany even after thyroidectomy. This pinned the dangerous post-operative tetany on the parathyroids and revealed that these tiny structures were not vestigial at all but vital to life. Over the following decades, investigators connected parathyroid function to the regulation of calcium in the blood — the parathyroids raise calcium when it falls too low — establishing the glands as the body's master controller of calcium balance. The full mechanism, mediated by a hormone, would not be confirmed until the twentieth century, but by the 1890s the essential role was clear: too little parathyroid activity causes tetany, and, as would later be understood, too much causes the opposite problem — the calcium excess at the heart of hyperparathyroidism.
Naming the Bone Disease: von Recklinghausen (1891)
While physiologists were working out what the parathyroids do, pathologists were independently describing a destructive bone disease whose cause was still a mystery. In 1891 — the same year as Gley's work — the German pathologist Friedrich Daniel von Recklinghausen gave a detailed description of a condition in which bone is progressively softened, replaced by fibrous tissue, and riddled with cysts and brown tumours, leaving the skeleton weak, deformed, and prone to fracture. The disease became known as osteitis fibrosa cystica, and in the older literature it is sometimes called von Recklinghausen's disease of bone (a separate entity from the more famous neurofibromatosis that also bears his name).
It is historically important to be precise here: von Recklinghausen described the bone disease, but he did not connect it to the parathyroid glands. At the time, no one suspected that an overactive gland in the neck could be dissolving the bones of the skeleton. The two threads — the gland and its function on one side, the wasting bone disease on the other — ran in parallel for more than thirty years before anyone tied them together. That missing link, the realization that osteitis fibrosa cystica is caused by an overactive parathyroid gland releasing too much hormone and stripping calcium out of bone, is what set the stage for the first attempt at a surgical cure.
The First Parathyroidectomy: Felix Mandl (1925)
The decisive surgical milestone came in Vienna. By the early 1920s the Viennese pathologist Jakob Erdheim and others had begun to suspect a relationship between parathyroid tissue and the destructive bone disease, though Erdheim interpreted the enlarged glands he saw at autopsy as a compensatory reaction to the bone disease rather than its cause. A young surgeon, Felix Mandl (1892–1957), reasoned the other way: if an overactive gland was driving the bone destruction, then removing it might reverse the disease.
In July 1925, at the surgical clinic in Vienna, Mandl operated on Albert Jahne, a 34-year-old Viennese streetcar conductor whose bones had become so fragile from osteitis fibrosa cystica that he could barely stand. Working under local anaesthesia, Mandl exposed the neck, identified the parathyroid glands, and removed a single enlarged one. The result was striking and, for its time, almost miraculous: the patient's bone pain eased, his strength returned, his blood calcium fell toward normal, and X-rays showed his bones beginning to heal and re-mineralize. This was the first parathyroidectomy performed to treat hyperparathyroidism, and it proved the central principle — that the disease originates in the gland and can be cured by removing it. The story has an honest, sobering coda: the patient's disease returned several years later and he ultimately died of uncontrolled high calcium. Even so, Mandl's operation is rightly regarded as the founding moment of modern parathyroid surgery.
The Case of Captain Charles Martell
If Mandl's operation proved the principle in Europe, it was a single American patient who drove the disease into the awareness of medicine in the United States. Captain Charles Martell was a merchant-marine officer who became, by the usual reckoning, the first recorded patient diagnosed with hyperparathyroidism in North America. A tall man — over six feet when he went to sea — he was progressively crippled over the 1920s by the same osteitis fibrosa cystica: he suffered repeated fractures, his limbs deformed, and he lost roughly half a foot of height as his softened skeleton collapsed in on itself. After an initial work-up in New York, he became the most famous patient of Ward 4, the metabolic research ward at the Massachusetts General Hospital in Boston, where physicians studied his calcium chemistry in unprecedented detail.
Martell's case became a landmark partly because of how hard-won his diagnosis and treatment were. Surgeons explored his neck again and again searching for the overactive gland, without lasting success. Only in 1932, after some seven neck explorations and finally a chest operation — his roughly ninth surgery in all — was the culprit found in an unexpected place: a parathyroid tumour located not in the neck but down in the mediastinum, the central compartment of the chest. The tumour was removed, but Martell did not ultimately survive; he died soon afterward of complications, with kidney stones and infection contributing to his death. His ordeal taught a generation of surgeons two enduring lessons: that parathyroid tumours can hide in ectopic locations such as the chest, and that the metabolic study of such patients could illuminate the disease. The work done on Ward 4 around his case helped make the Massachusetts General Hospital a centre of parathyroid surgery for decades to come.
Fuller Albright and the Modern Understanding
No single physician did more to convert these scattered discoveries into a coherent science of calcium and bone than Fuller Albright (1900–1969), an endocrinologist at the Massachusetts General Hospital whose meticulous metabolic studies — carried out in the same institution that cared for Charles Martell, often in its renal-stone clinic — defined the modern field. Albright pioneered the careful "balance study," measuring how much calcium and phosphorus a patient took in and excreted, and from these painstaking observations he built much of the framework still used today.
Among his lasting contributions, Albright showed that primary hyperparathyroidism could arise either from a single benign tumour (an adenoma) or from enlargement of all the glands (hyperplasia) — a distinction that still guides surgeons. He recognized kidney-stone disease as a distinct manifestation of the disorder, clarified the renal handling of calcium and phosphorus, described what is now called the "hungry bone" state that can follow successful surgery, and articulated the then-radical idea that target tissues can fail to respond to a hormone even when the hormone is present. His 1948 monograph, written with Edward C. Reifenstein, The Parathyroid Glands and Metabolic Bone Disease, became the standard reference for a generation. Albright's later career was tragically cut short by Parkinson's disease, but his work transformed hyperparathyroidism from a rare surgical curiosity into a well-understood disorder of mineral metabolism.
Isolating the Hormone and the Modern Era
Understanding that the parathyroids control calcium raised an obvious question: how? The answer was a hormone — parathyroid hormone (PTH) — but proving its existence and then capturing it in pure form took decades of effort. An important early step came in 1925, the very year of Mandl's operation, when the biochemist James B. Collip (well known for his earlier role in the purification of insulin) prepared an acid extract of parathyroid tissue that could relieve the tetany of animals whose glands had been removed. This demonstrated, chemically, that the glands released an active substance that raised blood calcium.
Purifying that substance, however, proved stubbornly difficult, and a truly pure preparation of parathyroid hormone was not obtained until 1959, through the work of investigators including Gerald Aurbach, Howard Rasmussen, and Lyman Craig, who used gentler extraction and separation methods than earlier attempts. With pure hormone in hand, the field advanced quickly: the complete amino-acid sequence of the hormone — a chain of 84 residues — was worked out around 1970 by the group of John T. Potts and colleagues (and independently by others). These chemical advances made it possible to develop blood tests that measure PTH directly, which together with reliable calcium measurement turned hyperparathyroidism from a disease recognized only when it had already wrecked the bones into one that can be caught early, often when a routine blood test simply shows a high calcium level. The history of the disease thus runs from a hidden organ, through a cure proven by surgery, to a hormone measured in a few drops of blood.
"Stones, Bones, Groans, and Moans"
No account of hyperparathyroidism's history is complete without the classic teaching mnemonic that has been handed down through generations of medical students: "stones, bones, abdominal groans, and psychiatric moans." The phrase is a compact summary of how the disease's hallmark feature — hypercalcaemia, too much calcium in the blood — tends to make itself known across the body. The longer form sometimes adds "thrones" (frequent urination) and "fatigue overtones," but the four-part version is the one most often recited.
Each element maps onto real pathology that the historical figures on this page helped to identify. Stones are the kidney stones that crippled Charles Martell and that Fuller Albright recognized as a distinct manifestation of the disease. Bones are the painful, fracturing osteitis fibrosa cystica that von Recklinghausen first described and that Mandl's surgery reversed. Abdominal groans capture the constipation, nausea, peptic ulcers, and (in some cases) pancreatitis that high calcium can provoke. And psychiatric moans — sometimes rendered as "psychiatric overtones" — describe the depression, anxiety, brain fog, irritability, and lethargy that often shadow the disease and that patients today still report as among its most troubling effects. The mnemonic endures because it is genuinely useful: it reminds clinicians that a single abnormal blood-calcium value can explain symptoms scattered across the kidneys, the skeleton, the gut, and the mind. For the practical, present-day side of all this — symptoms, diagnosis, and treatment — see the main Hyperparathyroidism page.
Research Papers and References
The references below combine peer-reviewed historical and biographical articles — with real DOIs and PMIDs where a specific paper is cited — with curated PubMed topic-search links into the broader literature on the discovery of the parathyroid glands and the history of hyperparathyroidism. Where a milestone is named in the text (Sandström, Gley, von Recklinghausen, Mandl, Albright), the dating reflects the consensus of these sources. Each link opens at the National Library of Medicine in a new tab.
- Eknoyan G. A history of the parathyroid glands. American Journal of Kidney Diseases. 1995;26(5):801-807. — PMID: 7485136
- DuBose J, Ragsdale T, Morvant J. "Bone, stones, and groans": Felix Mandl and the discovery of the parathyroid glands. The American Surgeon. 2005;71(9):794-797. — Search PubMed
- Modarai B, Sawyer A, Ellis H. The glands of Owen. Journal of the Royal Society of Medicine. 2004;97(10):494-495. — doi:10.1258/jrsm.97.10.494
- Carney JA. The glandulae parathyroideae of Ivar Sandström. Contributions from two continents. The American Journal of Surgical Pathology. 1996;20(9):1123-1144. — PMID: 8764749
- Eriksson B. The Uppsala anatomist Ivar Sandström and the parathyroid gland. Upsala Journal of Medical Sciences. 2015;120(2):71-77. — PMC4463479
- Casper S. Inexplicable patients: the case of Charles Martell and Ward 4 at the Massachusetts General Hospital. CMAJ. 2016;188(17-18):1263-1264. — doi:10.1503/cmaj.160111
- Cope O. The story of hyperparathyroidism at the Massachusetts General Hospital. New England Journal of Medicine. 1966;274(21):1174-1182. — Search PubMed
- Reilly BM. Fuller Albright and our current understanding of calcium and phosphorus regulation and primary hyperparathyroidism. Nefrología. 2011;31(3):346-349. — PMID: 21629339
- Potts JT. Parathyroid hormone: past and present. Journal of Endocrinology. 2005;187(3):311-325. — doi:10.1677/joe.1.06057
- The discovery of the parathyroid glands — Sandström and Owen PubMed: Sandström parathyroid discovery history
- Eugène Gley, parathyroid function, and the cause of tetany PubMed: Gley parathyroid tetany history
- von Recklinghausen and osteitis fibrosa cystica PubMed: von Recklinghausen osteitis fibrosa cystica history
- James Collip and the isolation of parathyroid hormone PubMed: Collip parathyroid hormone isolation history
- History of primary hyperparathyroidism — milestones and surgical management PubMed: primary hyperparathyroidism history and milestones
External Authoritative Resources
- NIDDK (NIH) — Primary Hyperparathyroidism
- MedlinePlus — Parathyroid Disorders
- PubMed — All research on the history of hyperparathyroidism
Connections
- Endocrinology
- Hyperparathyroidism (main page)
- All Conditions
- Osteoporosis
- Kidney Stones
- Thyroid Disorders
- Calcium
- Vitamin D3