Laryngeal Cancer
Laryngeal cancer is a malignancy of the larynx — the voice box — situated at the junction of the upper and lower respiratory tracts. Approximately 95% are squamous cell carcinomas (SCC) arising from the mucosal lining. It is the second most common head and neck cancer and a disease strongly linked to tobacco smoking and alcohol use. Unlike oropharyngeal cancer, laryngeal SCC is HPV-negative in the overwhelming majority of cases. Hoarseness persisting beyond three weeks in a current or former smoker is a red flag symptom that mandates urgent laryngoscopy.
Table of Contents
- Anatomy and Subsites
- Epidemiology
- Risk Factors
- Symptoms by Subsite
- Diagnosis and Workup
- Staging
- Early Glottic Cancer (T1–T2)
- Advanced Disease and Organ Preservation
- The RTOG 91-11 Landmark Trial
- Total Laryngectomy and Voice Rehabilitation
- Supraglottic and Subglottic Cancers
- References & Research
- Featured Videos
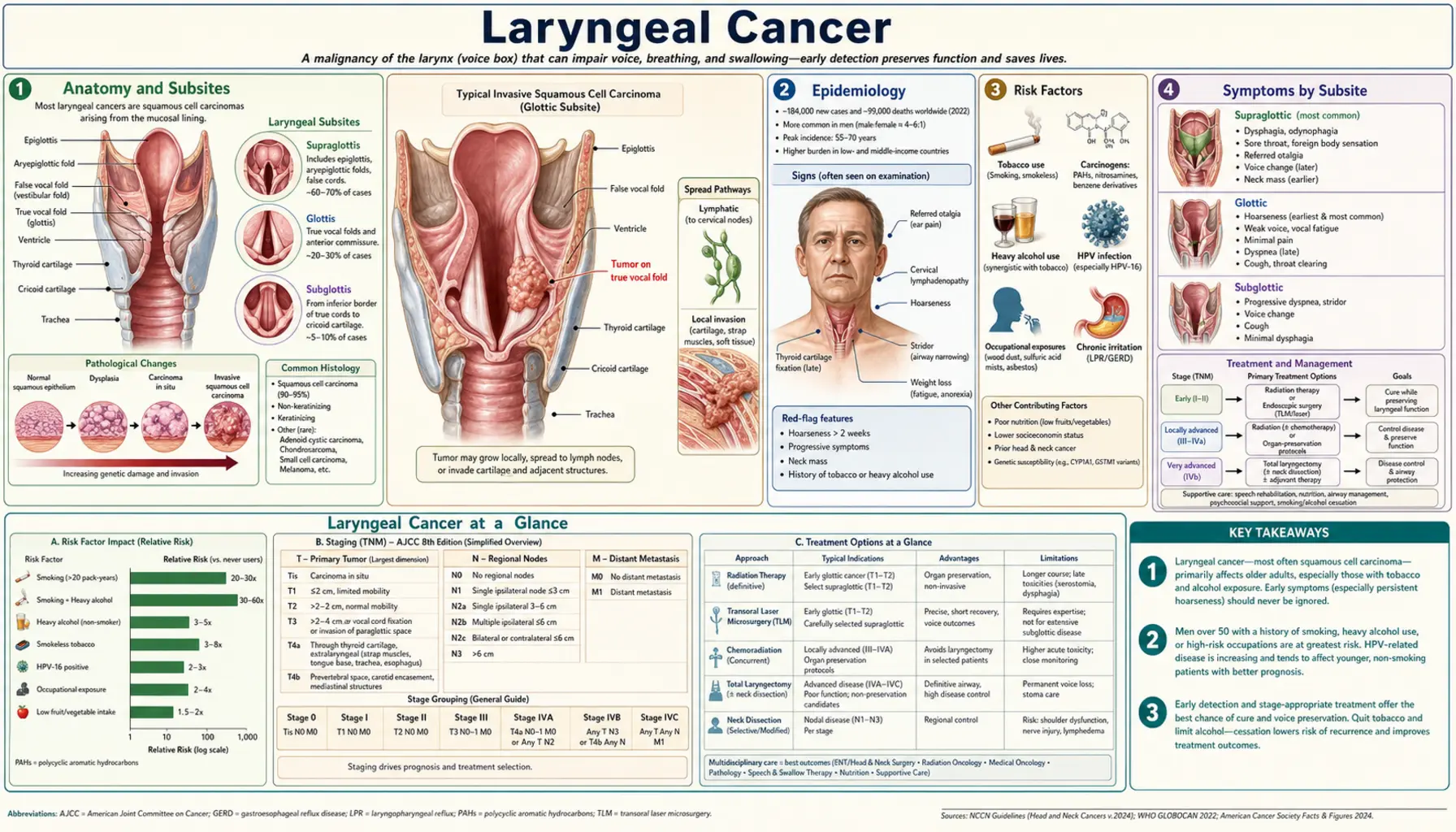
Anatomy and Subsites
The larynx is divided into three anatomical subsites, each with distinct lymphatic drainage, clinical behavior, and prognosis:
Glottis
The glottis comprises the true vocal cords (vocal folds) and the anterior and posterior commissures. It is the most common subsite for laryngeal cancer (approximately 60–65% of cases). The vocal cords are unique in having an extremely sparse lymphatic supply, which means that early-stage glottic cancers have a very low rate of lymph node metastasis and can be cured with high rates of success. Any lesion of the vocal cord produces hoarseness at an early stage — a biological advantage because it drives early presentation.
Supraglottis
The supraglottis includes the epiglottis, aryepiglottic folds, arytenoids, and false vocal cords. It accounts for approximately 30–35% of laryngeal cancers. In stark contrast to the glottis, the supraglottis has a rich bilateral lymphatic drainage. Supraglottic cancers therefore tend to present late — often with bulky nodal disease — because they produce no early functional symptom (hoarseness is a late sign when the tumor has extended to the true cords). Patients may first notice dysphagia, odynophagia, a referred otalgia, or a neck mass.
Subglottis
The subglottis is the least common site (<5% of cases), extending from below the true cords to the inferior margin of the cricoid cartilage. Subglottic cancers are rare, spread early to paratracheal and lower jugular lymph nodes, and carry a poorer prognosis because they are often not detected until they obstruct the airway or extend into the trachea.
Epidemiology
Laryngeal cancer accounts for approximately 2–5% of all cancers in developed countries. In the United States, approximately 12,000 new cases and 3,700 deaths occur annually. The incidence has declined significantly over the past three decades, largely reflecting reductions in tobacco smoking rates. The male-to-female ratio is approximately 4:1, though the gap is narrowing as smoking rates equalize between genders.
Squamous cell carcinoma accounts for 95–98% of laryngeal malignancies. Rare histologies include adenocarcinoma, neuroendocrine carcinoma (including small cell variants), chondrosarcoma, and lymphoma. Verrucous carcinoma — a well-differentiated, locally invasive variant of SCC — has a distinct biology: it rarely metastasizes but may undergo anaplastic transformation after radiation therapy.
Risk Factors
Tobacco Smoking
Tobacco is the overwhelmingly dominant risk factor, present in approximately 85–90% of patients with laryngeal cancer. Both cigarettes and cigars confer risk proportional to pack-year history. The relative risk of laryngeal cancer in heavy smokers is 10–30 times that of non-smokers. Even light smoking doubles the baseline risk.
Alcohol
Alcohol is an independent risk factor and acts synergistically with tobacco. Heavy alcohol consumption alone (3–4+ drinks per day) increases laryngeal cancer risk approximately 2–3 fold. The combination of heavy smoking and heavy drinking produces a multiplicative risk — estimated at 100-fold relative to non-using controls in some studies — through mechanisms including local acetaldehyde carcinogenesis, impaired folate metabolism, and reduced detoxification of tobacco carcinogens.
Gastroesophageal Reflux Disease (GERD)
Chronic acid and peptic reflux causes laryngopharyngeal irritation and may contribute to malignant transformation, particularly at the posterior commissure and subglottis. The association between laryngopharyngeal reflux and laryngeal cancer risk is supported by epidemiological studies and mechanistic data showing acid-induced upregulation of oncogenic pathways.
Radiation Exposure
Prior therapeutic radiation to the head and neck increases the risk of second primary laryngeal cancers. The latency period is typically 5–20 years after exposure.
Plummer-Vinson Syndrome
This syndrome (iron deficiency anemia, esophageal webs, dysphagia) is associated with increased risk of upper aerodigestive tract squamous cell carcinomas, including larynx and hypopharynx. The mechanism involves mucosal atrophy from nutritional deficiency.
HPV Status
In contrast to oropharyngeal SCC, where HPV (particularly HPV-16) drives a distinct biological subset with favorable prognosis, laryngeal SCC is HPV-positive in only approximately 5% of cases. HPV does not play a significant etiological role in laryngeal cancer, and the dramatic rise in HPV-positive oropharyngeal cancer seen over the past two decades has not been mirrored in the larynx.
Symptoms by Subsite
Glottic Cancer
Hoarseness is the cardinal and earliest symptom, arising because even small tumors on the vibratory margin of the vocal cord disrupt normal phonation. Any unexplained hoarseness lasting more than 3 weeks — particularly in a current or former smoker — mandates urgent laryngoscopy. This diagnostic imperative is critical because glottic cancers detected at T1 stage have cure rates exceeding 90%, while cure rates fall substantially for T3–T4 disease. Late symptoms of glottic cancer include stridor (airway narrowing), dysphagia (deep invasion), and, rarely, a palpable neck mass (late nodal involvement).
Supraglottic Cancer
Supraglottic cancers are silent until large. Early symptoms are non-specific: a persistent sore throat, odynophagia, or dysphagia. Referred otalgia (ear pain from the auricular branch of CN X, Arnold's nerve) is a classic but often overlooked symptom. A painless neck mass may be the first sign of nodal disease. Hoarseness appears late when the tumor extends down to the cords. Voice change + dysphagia + unilateral otalgia is a triad that should trigger immediate investigation.
Subglottic Cancer
Subglottic cancers are typically asymptomatic until they produce stridor or airway compromise from tracheal encroachment. Hoarseness occurs late when the tumor extends superiorly to involve the cords. Subglottic tumors may present with stridor that mimics asthma, leading to diagnostic delay.
Diagnosis and Workup
Laryngoscopy and Biopsy
Office-based flexible laryngoscopy (using a thin fiberoptic or digital chip endoscope passed through the nostril) provides immediate visualization of the entire larynx and piriform sinuses. Suspicious lesions appear as white (leukoplakia), red (erythroplakia), or exophytic mucosal abnormalities. Definitive diagnosis requires tissue biopsy under general anesthesia via direct laryngoscopy (microlaryngoscopy), which also permits precise mapping of tumor extent.
Stroboscopy
Stroboscopic examination assesses the mucosal wave of the vocal cords. Loss of the mucosal wave over a suspicious lesion suggests subepithelial invasion, which carries higher T-stage implications even when the lesion appears superficially limited.
CT Neck and Chest
Contrast-enhanced CT of the neck defines tumor extent, cartilage invasion (critical for staging), and cervical lymph node involvement. CT chest is essential to exclude pulmonary metastases and synchronous primary lung cancer — a clinical scenario occurring in approximately 3–5% of patients with laryngeal SCC given the shared tobacco carcinogen exposure.
PET-CT
FDG-PET/CT is recommended for staging of locoregionally advanced laryngeal cancer (T3–T4 or N+) to detect occult distant metastases (lung, liver, bone) and identify synchronous primary tumors. PET-CT detects distant metastases in approximately 10–15% of patients with advanced head and neck cancer, influencing treatment intent (curative vs. palliative).
MRI
MRI provides superior soft-tissue contrast for assessing pre-epiglottic space invasion, paraglottic space involvement, and cartilage marrow invasion — factors that upstage disease and influence surgical eligibility. It complements CT rather than replacing it.
Staging
Laryngeal cancer is staged by the AJCC/UICC TNM system (8th edition). Key staging determinants differ by subsite:
- Glottic T1: limited to vocal cord(s) with normal mobility; T1a = one cord, T1b = both cords
- Glottic T2: extension to supra- or subglottis, or impaired cord mobility
- Glottic T3: vocal cord fixation and/or invasion of paraglottic space, minor thyroid cartilage erosion
- Glottic T4a: invasion through thyroid cartilage or extension beyond larynx (trachea, esophagus, strap muscles); T4b = prevertebral space or encases carotid artery
- Supraglottic T1: limited to one subsite with normal mobility
- Supraglottic T2: extends to adjacent supraglottic subsite(s) or glottis or outside supraglottis
Regional lymph node involvement is the single most important prognostic factor, halving 5-year survival in most series. The cervical lymph nodes are classified by level (I–VI), with glottic cancers primarily draining to levels II–IV and supraglottic cancers draining bilaterally.
Early Glottic Cancer (T1–T2)
Early-stage glottic cancer is one of the most curable solid tumors. Two treatment modalities offer equivalent oncological control with different trade-offs:
Radiation Therapy (Definitive)
External beam radiation therapy (RT) delivers approximately 63–70 Gy in 30–35 fractions to the larynx over 6–7 weeks. Local control rates for T1 glottic cancer are 85–94% with RT alone. The key advantage is voice preservation with normal vocal cord anatomy — many patients retain near-normal voice quality. The larynx is irradiated as the primary organ, and radiation reactions (edema, mucositis) are manageable. Late complications include laryngeal fibrosis (<5%), hypothyroidism (from incidental thyroid irradiation), and a low risk of carotid stenosis and secondary malignancy over decades.
Transoral Laser Microsurgery (TLM)
CO2 laser resection of vocal cord tumors through a microlaryngoscope provides excellent local control (85–95% for T1 lesions) with minimal morbidity, same-day or overnight hospital stay, and rapid recovery. Voice quality after TLM depends on the depth of resection: superficial lesions can be resected with excellent voice outcomes, while deep resection involving the vocal ligament produces a hoarse or rough voice.
The choice between RT and TLM for early glottic cancer is made in multidisciplinary tumor board discussion, weighing the patient's baseline voice quality, tumor location (anterior commissure involvement is a risk factor for worse outcomes with both modalities), need for preservation of surgical options, and patient preference. Both options offer high cure rates exceeding 90% for T1N0 disease.
Advanced Disease and Organ Preservation
Locally advanced laryngeal cancer (T3–T4a, or any T with node-positive disease) historically required total laryngectomy. The pivotal VA Laryngeal Cancer Study Group trial (1991) and subsequent studies established that organ-preservation strategies using chemoradiation can achieve equivalent survival with larynx preservation in approximately 60–70% of patients.
Current standard of care for T3–T4a laryngeal cancer without frank cartilage destruction or airway compromise is organ-preservation chemoradiation, with total laryngectomy reserved as salvage for treatment failure or for patients with disease not amenable to organ preservation (e.g., extensive cartilage invasion, poor baseline laryngeal function).
The RTOG 91-11 Landmark Trial
The RTOG 91-11 trial is the most influential randomized controlled trial in laryngeal cancer management. It enrolled 547 patients with stage III–IV resectable laryngeal cancer and compared three arms:
- Induction chemotherapy (cisplatin + 5-FU) followed by RT (sequential)
- Concurrent chemoradiation (cisplatin 100 mg/m² every 3 weeks during RT)
- Radiation therapy alone
Key results from the 2003 update:
- Larynx preservation at 2 years: concurrent chemoRT 88% vs sequential 75% vs RT alone 70% (p <0.001)
- Locoregional control was significantly superior with concurrent chemoRT
- Overall survival was similar across all three arms — the trial was not powered to detect survival differences
- Toxicity was highest in the concurrent arm, including mucositis and dysphagia
RTOG 91-11 established concurrent cisplatin-based chemoradiation as the standard of care for larynx-preserving treatment of locoregionally advanced resectable laryngeal cancer. The induction chemotherapy arm (sequential) remained an acceptable alternative, particularly in patients where downstaging before RT is desired.
Long-term follow-up (10 years) of RTOG 91-11 revealed a concerning finding: increased non-cancer mortality in the concurrent chemoRT arm, possibly related to late treatment toxicity including dysphagia, aspiration, and laryngeal dysfunction. This has tempered enthusiasm for concurrent chemoRT in elderly patients or those with pre-existing dysphagia, and reinforced the need for careful patient selection and long-term functional monitoring.
Total Laryngectomy and Voice Rehabilitation
Total laryngectomy (TL) removes the entire larynx — including the epiglottis, thyroid cartilage, cricoid, and several tracheal rings — and creates a permanent tracheostoma in the neck. The pharynx is reconstructed primarily or with a free flap. TL permanently separates the respiratory and digestive tracts; the patient breathes through the stoma and has no risk of aspiration.
Despite the functional implications, total laryngectomy provides excellent locoregional control (90%+ for appropriately selected disease) and may be the best choice for:
- T4a tumors with frank cartilage destruction through the outer cortex
- Tumors invading the thyroid gland or cricoid cartilage
- Patients with pre-treatment aspiration or poor laryngeal function
- Salvage after failed chemoradiation (post-radiation TL carries a 20–30% pharyngocutaneous fistula rate)
Voice Rehabilitation After Total Laryngectomy
Loss of the larynx eliminates phonation. Three main voice rehabilitation options exist:
- Tracheoesophageal prosthesis (TEP/voice prosthesis): a one-way silicone valve inserted in a surgically created tracheoesophageal puncture (TEP), placed at the time of laryngectomy or as a secondary procedure. The patient occludes the stoma and diverts pulmonary air through the prosthesis into the esophagus, generating a pseudo-voice. This produces the best voice quality (conversational-level volume, natural inflection) and is the preferred method when feasible. Prosthesis maintenance (cleaning, replacement every 3–6 months) requires ongoing commitment.
- Electrolarynx: a battery-powered device held against the neck or cheek that vibrates the pharyngeal soft tissues. Produces a robotic, monotone quality but is easy to use immediately post-operatively. Valuable as a backup or primary option in patients unable to use TEP.
- Esophageal speech: the patient learns to inject air into the esophagus and expel it in a controlled belch, vibrating the pharyngoesophageal (PE) segment. The best-quality hands-free voice, but very difficult to learn and achieved by only 20–30% of patients.
Supraglottic and Subglottic Cancers
Supraglottic Cancer Management
For early supraglottic cancer (T1–T2, N0), both supraglottic laryngectomy (partial laryngectomy preserving the true cords) and radiation therapy offer comparable local control. Supraglottic laryngectomy requires a functioning larynx and an ability to tolerate aspiration during swallowing rehabilitation; it is contraindicated in patients with poor pulmonary reserve. Elective bilateral neck treatment (irradiation or selective neck dissection of levels II–IV) is standard given the bilateral lymphatic drainage.
For advanced supraglottic cancer (T3–T4), concurrent chemoradiation (following RTOG 91-11 principles) or total laryngectomy with neck dissection and adjuvant (chemo)radiation are the primary options.
Subglottic Cancer Management
Subglottic cancers are rare and carry a poor prognosis due to late presentation and early paratracheal nodal spread. Treatment typically requires total laryngectomy with paratracheal and superior mediastinal lymph node dissection, followed by adjuvant radiation. The role of concurrent chemoradiation alone is less well-defined due to small patient numbers.
References & Research
Key Research Papers
- The Department of Veterans Affairs Laryngeal Cancer Study Group. Induction chemotherapy plus radiation compared with surgery plus radiation in patients with advanced laryngeal cancer. N Engl J Med. 1991;324(24):1685–1690. PMID: 2034244
- Forastiere AA, Zhang Q, Weber RS, et al. Long-term results of RTOG 91-11: a comparison of three nonsurgical treatment strategies to preserve the larynx in patients with locally advanced larynx cancer. J Clin Oncol. 2013;31(7):845–852. PMID: 23182993
- Mendenhall WM, Werning JW, Hinerman RW, Amdur RJ, Villaret DB. Management of T1-T2 glottic carcinomas. Cancer. 2004;100(9):1786–1792 — Search PubMed
- Steiner W, Ambrosch P, Rödel RM, Kron M. Impact of anterior commissure involvement on local control of early glottic carcinoma treated by laser microresection. Laryngoscope. 2004;114(8):1485–1491 — Search PubMed
- Bussu F, Paludetti G, Almadori G, et al. Comparison of total laryngectomy with surgical (laryngeal-preserving) and nonsurgical organ-preservation protocols in resectable locally advanced (T3 and T4a) squamous cell carcinomas of the larynx. Head Neck. 2013;35(4):554–561 — Search PubMed
- Sjögren EV, Wiggenraad RG, Le Cessie S, Snijder S, Baatenburg de Jong RJ. Outcome of radiotherapy in T1 glottic carcinoma: a population-based analysis of prognostic factors. Eur Arch Otorhinolaryngol. 2009;266(5):735–744 — Search PubMed
- Hoffman HT, Porter K, Karnell LH, et al. Laryngeal cancer in the United States: changes in demographics, patterns of care, and survival. Laryngoscope. 2006;116(9 Pt 2 Suppl 111):1–13. PMID: 16946667
- Ang KK, Harris J, Wheeler R, et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N Engl J Med. 2010;363(1):24–35. PMID: 20530316
- Patel SG, Jäckel MC, Shah JP. Voice rehabilitation following total laryngectomy: current options and outcomes. Curr Opin Otolaryngol Head Neck Surg. 2003;11(2):100–107 — Search PubMed
- Ferris RL, Blumenschein G Jr, Fayette J, et al. Nivolumab for recurrent squamous-cell carcinoma of the head and neck. N Engl J Med. 2016;375(19):1856–1867. PMID: 27718784
- Bier-Laning CM, Duraes Camargo ZA, Messing BP, et al. Hypopharyngeal and laryngeal cancer: staging, treatment, and prognosis. Oral Maxillofac Surg Clin North Am. 2006;18(4):495–509 — Search PubMed
- Pfister DG, Spencer S, Adelstein D, et al. Head and neck cancers, version 2.2020, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2020;18(7):873–898 — Search PubMed
Research Papers
The following PubMed topic searches retrieve current peer-reviewed literature on Laryngeal Cancer.
- Laryngeal cancer treatment outcomes
- Laryngeal organ preservation chemoradiation
- Glottic cancer radiation vs laser
- Total laryngectomy voice prosthesis
- RTOG 91-11 larynx cisplatin trial
- Supraglottic cancer surgery radiation
- Laryngeal cancer tobacco alcohol risk
- Laryngeal cancer staging cartilage invasion
Connections
- ENT
- Vocal Cord Disorders
- Head and Neck Cancer
- Tobacco
- GERD
- Sinusitis
- Lung Cancer
- Dysphagia
- Tinnitus
- Acoustic Neuroma