Tinea Versicolor (Pityriasis Versicolor)
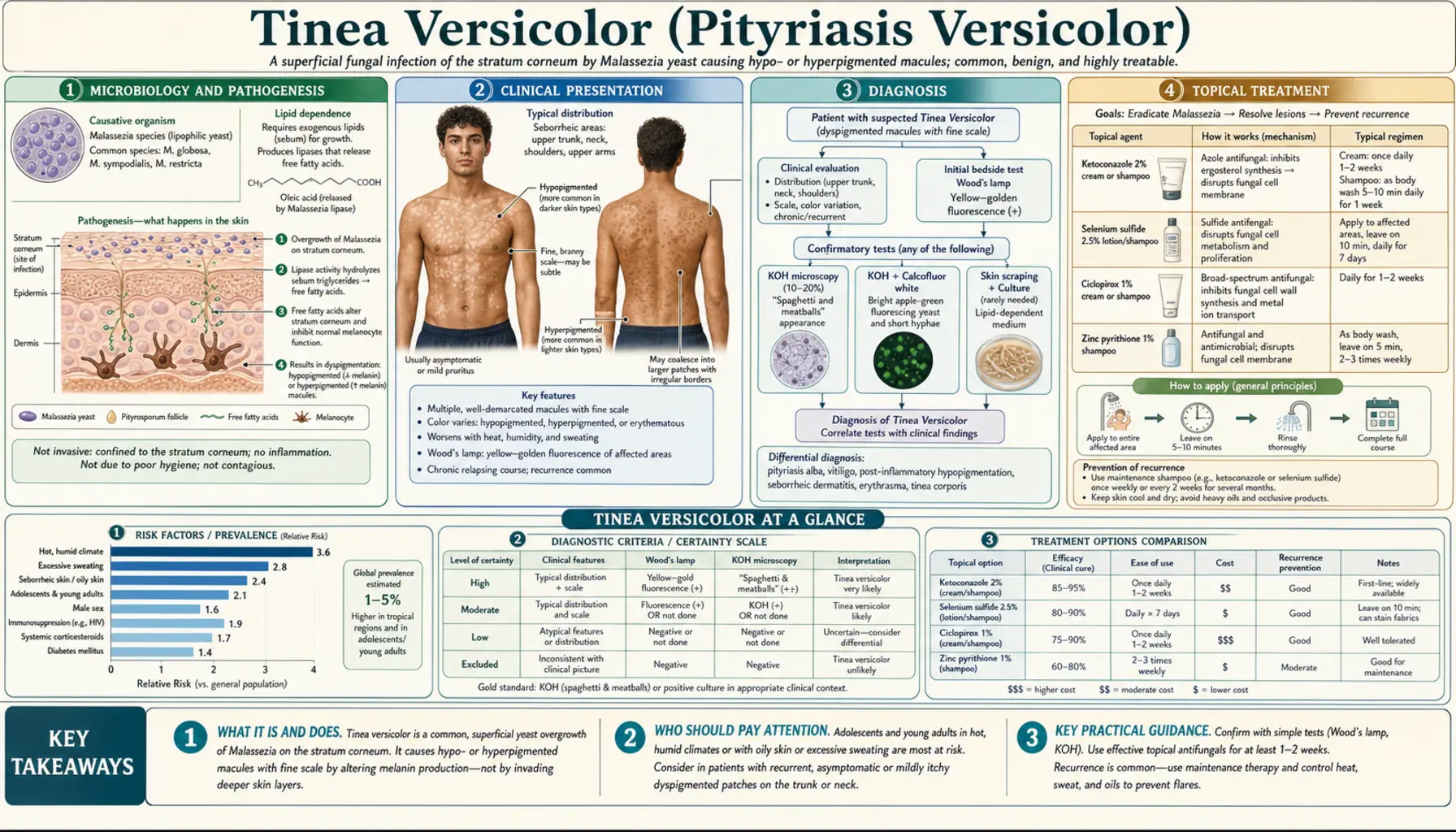
Tinea versicolor (pityriasis versicolor) is a common fungal infection of the skin caused by Malassezia yeast — a normal skin resident that converts to a pathogenic hyphal form under warm, humid conditions, causing distinctive patches of hypo- or hyperpigmented skin most commonly on the trunk, shoulders, and upper arms.
Table of Contents
- Microbiology and Pathogenesis
- Clinical Presentation
- Diagnosis
- Topical Treatment
- Oral Treatment
- Recurrence and Prophylaxis
- Special Populations
- Differential Diagnosis
- Key Research Papers
- PubMed Searches
- Connections
- Featured Videos
1. Microbiology and Pathogenesis
Tinea versicolor is caused by Malassezia species — lipophilic yeasts that are part of the normal human skin microbiome from infancy onward. Unlike most fungi, Malassezia cannot synthesize their own long-chain fatty acids and depend on host sebum for survival, which explains why the infection concentrates in sebaceous-rich areas of the body.
Multiple Malassezia species can cause tinea versicolor, with M. globosa being the most commonly isolated species in clinical cases worldwide. Other contributing species include M. furfur (historically considered the primary culprit), M. sympodialis, and M. restricta. Molecular typing has confirmed that M. globosa predominates in both tropical and temperate settings, though species distribution varies by region and skin type.
The central event in disease development is the conversion of the commensal yeast phase into a pathogenic hyphal or mycelial form. This morphological switch — from budding yeast to branching hyphae and pseudohyphae — is the hallmark of active infection and is what gives the KOH preparation its diagnostic "spaghetti and meatballs" appearance. The triggers for this phase transition include:
- Warm, humid environment: tropical and subtropical climates dramatically increase incidence; summer months in temperate zones drive seasonal outbreaks
- Sweating and exercise: perspiration raises surface humidity and alters the local pH and lipid composition of the skin
- Oily skin (hyperseborrhea): increased sebum provides more substrate for Malassezia proliferation
- Immunosuppression: HIV/AIDS, organ transplantation recipients, prolonged systemic corticosteroid use, and malnutrition all impair cutaneous immune surveillance
- Genetic predisposition: familial cases are well documented; some individuals appear prone to recurrence regardless of environmental factors
- Certain topical and systemic medications: corticosteroid creams, calcineurin inhibitors, and immunomodulators can promote local Malassezia overgrowth
The distinctive skin color changes result from two distinct mechanisms depending on which predominates in a given patient. Malassezia produces dicarboxylic acids — most importantly azelaic acid — as byproducts of fatty acid metabolism. Azelaic acid is a competitive inhibitor of tyrosinase, the rate-limiting enzyme in melanin synthesis. Reduced melanin production in the stratum corneum results in hypopigmented macules, the most recognized presentation. In some patients, perifollicular inflammation triggered by the host immune response to the hyphal form causes post-inflammatory hyperpigmentation, resulting in salmon-colored or tan macules instead.
Epidemiologically, tinea versicolor affects an estimated 2–8% of the global population under temperate conditions, rising to 30–40% in tropical and subtropical regions where heat and humidity prevail year-round. Peak incidence occurs between ages 15 and 30, corresponding closely with maximal sebaceous gland activity during and after puberty. The condition is roughly equally distributed between males and females. Tinea versicolor is distinctly uncommon in prepubertal children and the elderly, both groups having lower sebum production — further supporting the role of sebaceous activity in pathogenesis.
2. Clinical Presentation
The clinical appearance of tinea versicolor is defined by patches of altered skin color with a fine, easily detached scale. The color change — which can go in either direction, lighter or darker than the surrounding skin — is what leads most patients to seek care, often out of cosmetic concern rather than discomfort.
Color Variants
Hypopigmented macules are the most common presentation and the most distressing for patients with naturally darker or tanned skin, where pale patches stand in sharp contrast to surrounding pigmented skin. On lighter, untanned skin, these same lesions may appear as faint tan or off-white patches that are easy to miss. The hypopigmentation results from azelaic acid–mediated tyrosinase inhibition and persists for weeks to months after successful treatment while melanocytes gradually recover.
Hyperpigmented or salmon-colored macules are the characteristic finding on naturally fair, untanned skin. These lesions are tan-to-salmon-pink in color and may be more immediately noticeable than their hypopigmented counterparts. They reflect local perifollicular inflammation rather than depigmentation.
Brown hyperpigmented lesions occur in a subset of patients — particularly in darker skin phototypes — and can resemble other pigmentary disorders.
Scale
A defining feature is the fine "furfuraceous scale" (from Latin furfur, bran), a branny, flaky scale that lies flat on the skin surface and may not be obvious until the skin is gently scraped. Running the edge of a fingernail or a tongue depressor across a lesion dislodges the scale easily — this simple bedside maneuver can confirm the clinical diagnosis and distinguish tinea versicolor from vitiligo (which does not scale).
Distribution
The infection is confined to sebaceous-rich regions of the body. The most commonly affected sites are:
- Upper chest and sternum (most common)
- Upper back and shoulders
- Upper arms and proximal forearms
- Neck
- Face — more common in children, adolescents, and immunocompromised adults
- Axillae and groin (less common; involvement suggests more extensive disease)
Individual macules typically measure 1–3 cm in diameter, with irregular, well-defined borders. Lesions frequently coalesce into larger confluent patches covering broad areas of the trunk. The distribution spares the palms, soles, and mucous membranes.
Symptoms
Most patients are asymptomatic — the color change itself prompts the visit. Mild pruritus is occasionally reported, particularly with heat and sweating. There are no systemic symptoms (fever, lymphadenopathy, or constitutional signs), which helps distinguish tinea versicolor from more invasive fungal infections.
Effect of Sun Exposure
A hallmark diagnostic clue: tinea versicolor lesions fail to tan. After sun exposure, the surrounding normal skin darkens while the affected patches remain the same color — making hypopigmented lesions appear suddenly more prominent in summer. This seasonal unmasking is a common reason patients first notice or present with the condition.
3. Diagnosis
Tinea versicolor is primarily a clinical diagnosis confirmed by simple bedside tests. The combination of characteristic color changes, fine scale, and distribution in a young adult in a warm climate is usually sufficient. Laboratory confirmation is quick and inexpensive.
Wood's Lamp Examination
A Wood's lamp (longwave ultraviolet, 365 nm) is applied in a darkened room. Active tinea versicolor lesions fluoresce yellow-green to golden yellow — a reflection of pteridine metabolites produced by Malassezia. The test is positive in approximately 60% of cases; a negative result does not exclude the diagnosis. Wood's lamp is most useful for delineating disease extent in lightly pigmented patients and for differentiating tinea versicolor from erythrasma (coral-red fluorescence from Corynebacterium minutissimum).
KOH Preparation (Definitive)
The potassium hydroxide (KOH) preparation remains the gold standard for rapid in-office confirmation. A superficial scraping of a lesion is obtained with a blade or glass slide, placed on a microscope slide with a drop of 10–20% KOH solution, gently heated, and examined under light microscopy. The pathognomonic finding is the "spaghetti and meatballs" pattern:
- Spaghetti: short, stubby, curved hyphae and pseudohyphae
- Meatballs: clusters of thick-walled, round yeast cells
This combination of hyphae and yeast in the same preparation is unique to Malassezia among common dermatophytes and is diagnostic. Adding calcofluor white stain enhances visibility under fluorescence microscopy when available.
Culture
Culture is not routinely performed in clinical practice. Malassezia species require lipid-supplemented growth media (standard Sabouraud agar overlaid with olive oil or other long-chain fatty acid sources) and grow slowly. Culture is used in research settings for species identification and antifungal susceptibility testing.
Dermoscopy
Dermoscopy reveals a follicular distribution of white-yellow scaling and a "flour-like" surface pattern. It can help confirm the diagnosis in cases where scale is subtle and KOH is not immediately available.
Skin Biopsy
Biopsy is rarely needed but may be performed when the diagnosis is uncertain or when malignant causes of pigmentary change must be excluded. Periodic acid–Schiff (PAS) and Grocott–Gomori methenamine silver (GMS) stains reveal hyphae and yeast forms within the stratum corneum. Notably, the dermal inflammatory infiltrate is minimal, consistent with the largely superficial, non-invasive nature of the infection.
4. Topical Treatment
Topical antifungal agents are first-line treatment for tinea versicolor. They are effective, well tolerated, and inexpensive. Because the infection involves the entire sebaceous-zone skin surface — not just visible lesions — treatment should cover the entire trunk and affected areas, not merely the visible patches. This broader application reduces the reservoir of Malassezia and lowers recurrence risk.
Selenium Sulfide 2.5% (First-Line)
Selenium sulfide lotion or shampoo is one of the most effective and cost-accessible treatments. The standard regimen involves applying the product to all affected skin from the neck to the waist, allowing it to remain on the skin for 10–15 minutes, then rinsing in the shower. This is repeated daily for 1–2 weeks. The 2.5% prescription formulation is more potent; a 1% OTC formulation (e.g., Selsun Blue) has lower efficacy but is widely accessible. Mild skin irritation and a distinctive odor are the main tolerability concerns.
Ketoconazole 2% Shampoo
Ketoconazole 2% shampoo (e.g., Nizoral) used as a body wash is equally effective and is an alternative first-line option. The same leave-on technique applies: apply to wet skin, lather, leave for 5 minutes, rinse. A single application has demonstrated mycological cure in some trials; alternatively, once weekly for 4 weeks is prescribed for more extensive disease. It is well tolerated and odorless — an advantage over selenium sulfide.
Zinc Pyrithione Shampoo
Zinc pyrithione (available OTC in many anti-dandruff shampoos) has antifungal activity against Malassezia via copper ion chelation and membrane disruption. It is slightly less effective than ketoconazole or selenium sulfide but is inexpensive, widely available, and safe for long-term prophylactic use.
Ciclopirox 1% Gel or Shampoo
Ciclopirox is a broad-spectrum antifungal with a unique mechanism (chelates metal ions essential for fungal enzyme activity). Applied once daily for 2 weeks as a gel or shampoo, it achieves high mycological cure rates comparable to ketoconazole. It is an alternative for patients intolerant of selenium sulfide.
Azole Creams (Clotrimazole, Miconazole, Econazole)
Standard over-the-counter azole antifungal creams are effective when applied twice daily for 2–4 weeks. They work well for limited disease but are less practical for the large body surface areas typically involved in tinea versicolor — applying cream to the entire trunk twice daily for a month is burdensome compared to a once-daily shampoo technique.
Terbinafine
Terbinafine spray or cream is effective against most dermatophytes but has limited efficacy against Malassezia. Malassezia species possess a unique ergosterol biosynthesis pathway with low sensitivity to terbinafine's squalene epoxidase inhibition. Terbinafine is not recommended as first-line treatment for tinea versicolor.
Practical Application Note
Patients must be clearly informed that successful antifungal treatment — confirmed by resolution of scale and negative KOH — does not immediately restore normal skin color. Hypopigmented patches may persist for months as melanocytes gradually replenish melanin. Patients who are not counseled about this commonly assume treatment failed and discontinue unnecessarily.
5. Oral Treatment
Oral antifungal therapy is indicated when topical treatment has failed, when disease is extensive (covering large body surface area), when anatomical sites are difficult to reach with topicals, or when the patient has frequent, debilitating recurrences.
Fluconazole
Fluconazole is the most commonly used oral agent for tinea versicolor in current practice. Two regimens have been validated:
- Single dose: 300–400 mg as a one-time treatment. Highly convenient and effective for mild-to-moderate disease.
- Weekly dosing: 150 mg once weekly for 4 weeks for more extensive disease or higher recurrence risk.
A clinically documented trick to maximize efficacy: patients are instructed to exercise and sweat within 30–60 minutes of taking the oral dose. Fluconazole is secreted in sweat at fungicidal concentrations, and physical activity actively delivers the drug to the skin surface where Malassezia resides. This maneuver has been shown to improve mycological cure rates compared to the same dose without exercise.
Itraconazole
Itraconazole 200 mg/day for 5–7 days is highly effective and provides excellent tissue penetration. It is lipophilic and concentrates in the stratum corneum and sebum, making it particularly well suited for a lipid-loving pathogen like Malassezia. Food (especially a fatty meal) substantially increases itraconazole absorption and should be taken with the medication. Important considerations include multiple drug interactions through CYP3A4 inhibition; a thorough medication review is essential before prescribing.
Ketoconazole (Oral — No Longer First-Line)
Oral ketoconazole was historically the first-line systemic treatment but was subject to an FDA Drug Safety Communication in 2013 warning of significant risks: hepatotoxicity (including fatal liver failure), adrenal insufficiency, and extensive drug-drug interactions. Oral ketoconazole should be reserved for cases where other antifungals are unavailable or contraindicated, used with close monitoring of liver function and adrenal status. It is no longer recommended as a routine or first-line oral agent for tinea versicolor.
Important Caveat on Repigmentation
Oral antifungal therapy, like topical treatment, clears the fungal infection but does not accelerate pigmentary recovery. Color normalization depends on melanocyte recovery and is not influenced by the route or potency of antifungal used. Patients achieve mycological cure — confirmed by KOH — weeks before color returns to baseline. Sun exposure after treatment helps stimulate melanocyte activity and makes residual hypopigmented patches less noticeable by tanning the surrounding skin.
Antifungal Resistance
Clinically significant resistance to azoles in Malassezia species is rare and not a routine concern in the management of tinea versicolor. Treatment failure is far more commonly due to reinfection from the patient's own commensal reservoir than to true antifungal resistance.
6. Recurrence and Prophylaxis
Tinea versicolor is notorious for its high recurrence rate. Because Malassezia is a permanent resident of the normal skin microbiome — not an organism that can be permanently eliminated — any return of favorable conditions will permit the yeast to revert to the pathogenic hyphal form. Without prophylaxis, 60–80% of patients experience recurrence within one year of successful treatment.
Pharmacological Prophylaxis
Monthly maintenance regimens during warm-weather months (or year-round in tropical climates) are effective and widely recommended:
- Ketoconazole 2% shampoo: once monthly as a full-body wash (same 5-minute leave-on technique), used as a body wash rather than a shampoo. Simple, inexpensive, and well tolerated for long-term use.
- Selenium sulfide 2.5% lotion: applied once monthly to the trunk and allowed to remain for 10 minutes before rinsing.
- Fluconazole 300 mg once monthly (oral): convenient one-pill prophylaxis for patients who prefer systemic treatment or find topical application cumbersome.
Behavioral Modifications
Reducing skin surface humidity and sebum load lowers recurrence risk:
- Shower promptly after exercise — do not remain in damp, sweat-soaked clothing
- Use ketoconazole or zinc pyrithione shampoo as a weekly body wash during susceptible months
- Avoid heavy occlusive garments (synthetic materials that trap heat and moisture) during warm weather
- Manage hyperhidrosis — if excessive sweating is identified as a consistent trigger, discuss treatment options with a dermatologist
- Minimize the use of occlusive skin products and heavy emollients on the trunk
Counseling on Repigmentation Timeline
Perhaps the most important element of patient counseling concerns the timeline for color restoration. After successful antifungal treatment and confirmed mycological cure:
- Fair-skinned patients: residual hypopigmented patches may persist for 1–2 months
- Medium-to-dark skin phototypes: residual patches commonly persist for 3–12 months
- Darker skin phototypes: the contrast between treated patches and surrounding pigmented skin makes recovery subjectively slower; patients may require repeated reassurance that treatment is working
Sun exposure after confirmed cure can be helpful — moderate exposure accelerates melanocyte recovery and simultaneously darkens surrounding skin, making residual patches less conspicuous. This is one of the few clinical scenarios where modest, controlled sun exposure is actively encouraged.
7. Special Populations
Children
Tinea versicolor is uncommon in prepubertal children due to relatively low sebaceous gland activity before puberty. When it does occur in younger children, facial involvement — including forehead, cheeks, and hairline — is proportionally more common than in adults, likely because children's faces are among their most sebum-active skin zones before puberty. Topical azole creams and ketoconazole shampoo are appropriate treatments; selenium sulfide is generally considered safe in adolescents. Oral azoles should be used cautiously and only when topical therapy is insufficient.
Pregnancy
Topical treatments are generally preferred during pregnancy. Selenium sulfide and topical azole creams (clotrimazole, miconazole) are considered low-risk and are widely used. Zinc pyrithione OTC shampoos are also acceptable. Oral azoles require more caution: fluconazole at high doses (400–800 mg) has been associated with fetal cardiac and limb abnormalities in animal studies, and an FDA Drug Safety Communication (2016) flagged concern about even single 150-mg doses in the first trimester. Most guidelines recommend avoiding oral azoles in the first trimester and using them only when benefits clearly outweigh risks in later pregnancy. Itraconazole is also teratogenic in animal models and is generally avoided throughout pregnancy.
Immunocompromised Patients
Patients with HIV/AIDS (particularly with CD4 counts below 200 cells/mm³), solid organ transplant recipients on immunosuppression, and patients on prolonged systemic corticosteroids are prone to more extensive, treatment-resistant, and atypical tinea versicolor. Facial involvement, folliculitis variants (Malassezia folliculitis), and rapid recurrence are common features. These patients often require longer courses of oral azoles, combination topical and systemic therapy, and indefinite prophylaxis. Underlying immunosuppression management — where modifiable — is an important part of the overall approach.
Darker Skin Phototypes (Fitzpatrick IV–VI)
Patients with naturally darker skin experience hypopigmented patches as particularly striking and psychologically distressing, given the strong contrast against their surrounding skin. The repigmentation timeline is correspondingly longer (up to 12 months). For these patients, combination topical plus oral therapy — with prompt monthly prophylaxis to prevent recurrence during the long repigmentation period — is often the most practical approach to minimize the total duration of visible skin change.
Tropical and Subtropical Residents
In tropical regions with sustained heat and humidity year-round, the "warm months" prophylaxis strategy collapses into essentially continuous prophylaxis. Monthly ketoconazole shampoo body washes or monthly fluconazole indefinitely are appropriate in high-recurrence individuals living in tropical environments. Patient education about the chronic, recurrent nature of the condition — rather than treating each episode as a new infection — is especially important in these settings.
8. Differential Diagnosis
Several conditions share clinical features with tinea versicolor — particularly color change, scale, and trunk distribution. Accurate differentiation is important because treatments differ substantially.
Vitiligo
The most common source of diagnostic confusion with hypopigmented tinea versicolor. Key distinguishing features: vitiligo produces complete depigmentation (chalk-white, not merely lighter patches), is autoimmune in etiology, and shows no scale. Under Wood's lamp, vitiligo patches fluoresce brilliant blue-white rather than yellow-green. KOH preparation is negative. Vitiligo preferentially involves the face, hands, periorificial skin, and flexures — not the sebaceous trunk.
Pityriasis Rosea
Self-limiting inflammatory eruption that begins with a single "herald patch" followed by a secondary eruption of smaller oval salmon-colored plaques in a "Christmas tree" distribution along skin tension lines on the trunk and proximal extremities. Each lesion has a distinctive peripheral "collarette scale." The eruption resolves spontaneously in 6–12 weeks. KOH preparation is negative.
Seborrheic Dermatitis
Shares a Malassezia etiology with tinea versicolor and responds to the same antifungals, but presents differently: erythema with greasy, yellowish scale predominating on the scalp, nasolabial folds, eyebrows, and central chest. Pruritus is more prominent. The two conditions can coexist in the same patient.
Contact Dermatitis
Allergic or irritant contact dermatitis produces erythema, pruritus, and sometimes vesiculation with clear demarcation corresponding to the site of allergen or irritant contact. Scale, if present, is coarser. Patch testing (allergic) or exposure history (irritant) distinguishes the cause. KOH is negative.
Erythrasma
Superficial bacterial infection with Corynebacterium minutissimum presenting as well-demarcated, reddish-brown to brown patches in intertriginous areas (axillae, groin, toe webs). The critical distinguishing feature is Wood's lamp examination: erythrasma shows brilliant coral-red fluorescence (from porphyrin produced by Corynebacterium), whereas tinea versicolor shows yellow-green fluorescence. Treatment differs: erythrasma responds to topical erythromycin or clindamycin, not antifungals.
Hypopigmented Mycosis Fungoides
A rare variant of cutaneous T-cell lymphoma that can present as persistent hypopigmented patches on the trunk, especially in younger patients with darker skin. Clinically it may be nearly identical to tinea versicolor. Key distinctions: lesions are persistent and refractory to antifungal treatment; KOH is negative. Skin biopsy with immunohistochemistry reveals the diagnostic atypical CD8+ lymphocytic infiltrate. A biopsy should be performed in any patient with persistent "tinea versicolor" that fails to respond to appropriate antifungal therapy.
9. Key Research Papers
- Crespo-Erchiga V, Florencio VD. "Malassezia yeasts and pityriasis versicolor." Curr Opin Infect Dis. 2006;19(2):139–147. — Search PubMed
- Faergemann J, Bernander S. "Micro-aerophilic and anaerobic growth of Pityrosporum orbiculare and Pityrosporum ovale." Br J Dermatol. 1986;115(3):305–312. — Search PubMed
- Gupta AK, Bluhm R, Summerbell R. "Pityriasis versicolor." J Eur Acad Dermatol Venereol. 2002;16(1):19–33. — Search PubMed
- Schwartz RA. "Superficial fungal infections." Lancet. 2004;364(9440):1173–1182. PMID: 15451228
- Assaf RR, Weil ML. "The superficial mycoses." Dermatol Clin. 1996;14(1):57–67. PMID: 8821165
- Faergemann J. "Pityriasis versicolor." Dermatol Clin. 1996;14(1):41–47. — Search PubMed
- Vena GA, Chieco P, Posa F, Garofalo A, Boscia A, Cassano N. "Pityriasis versicolor." Int J Dermatol. 1994;33(12):848–851. — Search PubMed
- Hu SW, Bigby M. "Pityriasis versicolor: a systematic review of interventions." Arch Dermatol. 2010;146(10):1132–1140. — Search PubMed
- Negroni R. "Pityriasis versicolor: etiología, patogenia y tratamiento." Rev Argent Microbiol. 2010;42(1):67–74. — Search PubMed
- Gupta AK, et al. "Systematic review of topical treatments for tinea versicolor." J Am Acad Dermatol. 2014. PubMed search: tinea versicolor topical treatment systematic review
- Gupta AK, Foley KA. "Antifungal treatment for pityriasis versicolor." J Fungi (Basel). 2015;1(1):13–29. PubMed search: Gupta Foley pityriasis versicolor antifungal 2015
- Borelli D, Jacobs PH, Nall L. "Tinea versicolor: epidemiologic, clinical and therapeutic aspects." J Am Acad Dermatol. 1991;25(2):300–305. PubMed search: Borelli tinea versicolor epidemiologic 1991
10. PubMed Searches
- Pityriasis versicolor treatment
- Tinea versicolor and Malassezia
- Tinea versicolor selenium sulfide
- Pityriasis versicolor fluconazole
- Pityriasis versicolor recurrence prophylaxis
11. Connections
- Dermatology
- Fungal Infections
- Seborrheic Dermatitis (Malassezia connection)
- Vitiligo (key differential)
- Pityriasis Rosea
- Folliculitis (Malassezia folliculitis variant)
- Contact Dermatitis
- Eczema
- Acne (Malassezia acne)