Psoriasis: History and Discovery
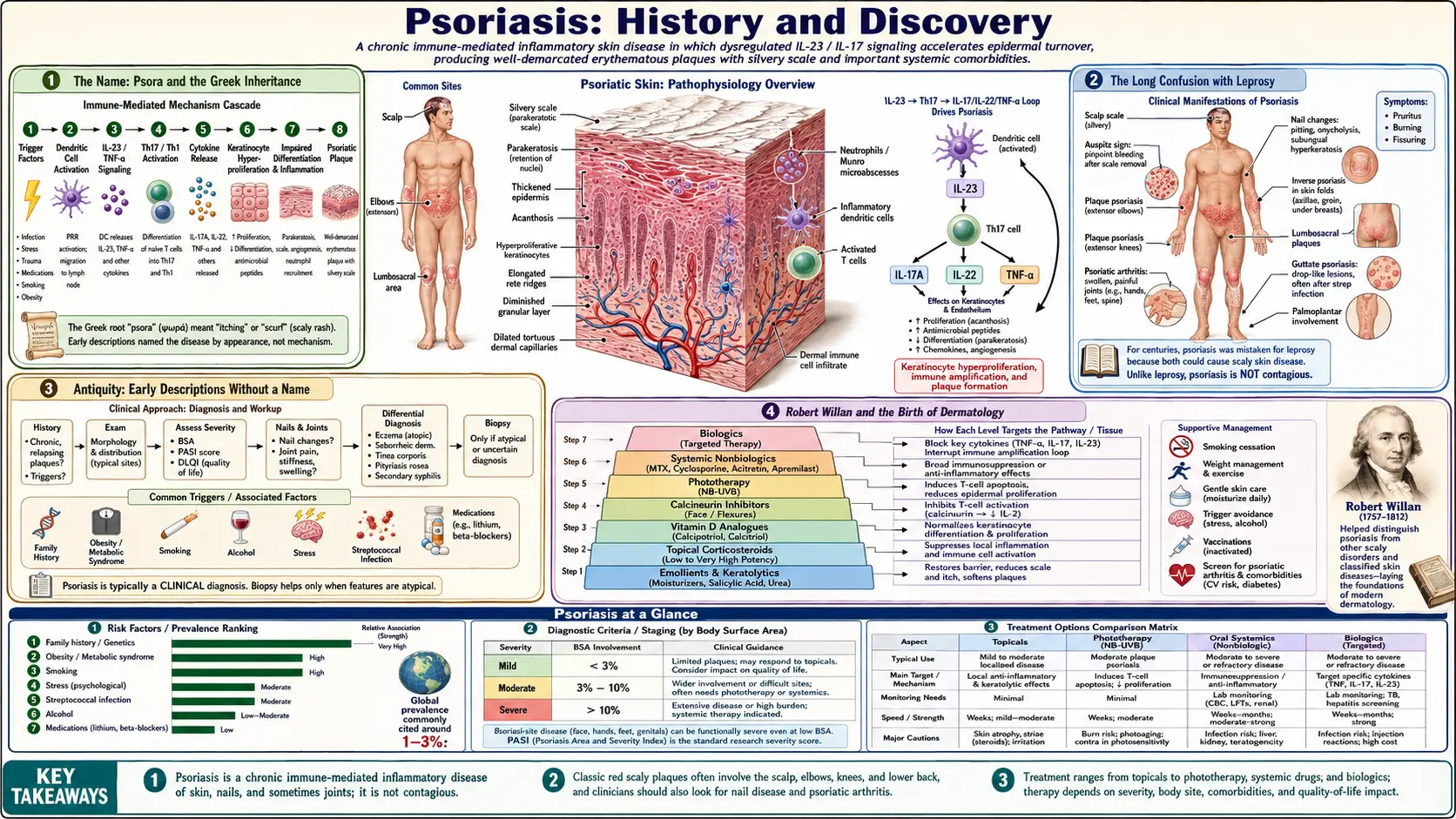
The word psoriasis comes from the Greek psora, meaning "itch." Yet for most of recorded history this scaly, lifelong skin disease had no settled identity of its own. It was repeatedly mistaken for leprosy, and the people who carried it were too often shunned, segregated, and condemned along with those who had Hansen's disease. The slow work of untangling psoriasis from leprosy — and of recognizing it as a distinct, non-contagious disorder — runs from the careful classifications of Robert Willan in London around 1808, through Ferdinand von Hebra's decisive separation of the two diseases in Vienna in 1841, to Heinrich Koebner's 1872 observation that trauma can seed new lesions, and finally to the modern understanding of psoriasis as a chronic, immune-mediated disease driven by the body's own T cells and the IL-23/IL-17 signalling axis. This page traces that two-thousand-year journey from confusion to clarity.
Table of Contents
- The Name: Psora and the Greek Inheritance
- The Long Confusion with Leprosy
- Antiquity: Early Descriptions Without a Name
- Robert Willan and the Birth of Dermatology
- Ferdinand von Hebra: Separating Psoriasis from Leprosy
- Heinrich Koebner and the Isomorphic Phenomenon
- A History of Treatments: Tar, Light, and Beyond
- The Modern Era: An Immune-Mediated Disease
- Legacy: From Stigma to Science
- Research Papers and References
- Connections
- Featured Videos
The Name: Psora and the Greek Inheritance
The modern term psoriasis is built from the ancient Greek psora (ψωρα), meaning "itch" or "the itch," combined with the suffix -iasis, which denotes a condition or diseased state. Rendered literally, the word means something like "the itching condition." In classical Greek medicine, however, psora was a broad, loose label applied to a whole range of rough, scaly, itchy skin complaints — it did not single out the disease we now call psoriasis. The Greek physician Galen (second century CE) is often credited with using the word psoriasis in a recognizable medical sense, but the conditions he and his contemporaries grouped under it almost certainly included eczema-like and other scaling disorders as well.
This matters because it explains a recurring theme in the history of the disease: for most of two thousand years, the name existed without a precise meaning attached to it. The same Greek root psora also fed into Latin and later European medical vocabulary, where it kept its vague sense of "scabby, itchy skin." Only in the nineteenth century, with the rise of systematic dermatology, did psoriasis finally come to denote one specific, well-defined disease rather than a fuzzy family of skin problems.
It is worth being honest about the limits of the ancient record. Because the terminology was imprecise, we cannot always be certain which historical "itch" or "scale" descriptions truly refer to psoriasis as a dermatologist would diagnose it today. Historians therefore distinguish the history of the word, the history of the clinical description, and the history of understanding the cause — three threads that, for psoriasis, converged only relatively recently.
The Long Confusion with Leprosy
The most consequential fact in the history of psoriasis is that, for most of recorded time, it was tragically confused with leprosy. To pre-modern eyes, both diseases produced visible, disfiguring changes to the skin, and the available vocabulary — Greek lepra (meaning "scaly"), Hebrew tzaraath, and a shifting collection of Latin terms — lumped many distinct conditions together under headings that crossed freely between what we now call leprosy, psoriasis, and other chronic skin diseases. A person with thick, silvery, scaling plaques could easily be classed among "lepers," with no clinical means to tell the diseases apart.
The consequences of this confusion were severe and often cruel. In medieval Europe, leprosy carried profound social and religious stigma; those judged to be lepers could be expelled from their communities, required to carry warning bells or clappers, barred from public life, and in some places subjected to formal ceremonies that declared them dead to society. People whose only affliction was psoriasis — a non-contagious disease that harms the skin but is not the bacterial infection of leprosy — were sometimes swept up in these measures, confined to leprosaria, or shunned as unclean. The biblical and ecclesiastical framing of scaly skin disease as a marker of ritual impurity deepened the suffering, attaching moral and spiritual judgment to a condition the sufferer could neither cause nor control.
It is important to state the historical claim carefully and not overreach: the surviving records rarely let us prove that any specific individual labeled a "leper" actually had psoriasis rather than Hansen's disease. What the record does establish is that the two diseases were not reliably distinguished, that the diagnostic categories were porous, and that this conflation caused real, documented harm. Untangling psoriasis from leprosy was therefore not merely an academic exercise in classification — it was the precondition for treating people who had it with dignity and for studying the disease on its own terms.
Antiquity: Early Descriptions Without a Name
Scaly skin disease compatible with psoriasis appears in the medical writings of classical antiquity, even though the disease was not isolated as a separate entity. Within the Hippocratic tradition (associated with Greek medicine from roughly the fifth and fourth centuries BCE), various dry, scaling, and itchy eruptions were grouped under terms such as lepra and psora. The Roman encyclopedist Cornelius Celsus, writing his medical compendium De Medicina in the first century CE, described several scaling skin conditions in enough detail that later commentators have argued some of his accounts correspond to psoriasis — though, as always with ancient sources, the identification cannot be made with certainty.
The deeper problem was conceptual rather than observational. Ancient physicians could see and describe scales, plaques, redness, and itching perfectly well; what they lacked was any framework that would let them separate one chronic scaling disease from another, or distinguish a non-contagious skin disorder from an infectious one. Disease was generally understood through the theory of the four humors, in which skin eruptions reflected an internal imbalance — an explanatory model that grouped conditions by appearance and supposed cause rather than by the specific mechanisms we now recognize.
As a result, antiquity bequeathed a rich vocabulary of scaly-skin terms but no stable disease called psoriasis — descriptive richness layered over diagnostic confusion, plus a persistent association between visible skin disease and impurity. That tangle would not be sorted out until medicine developed the systematic, observation-based classification of skin diseases that defines the modern field of dermatology.
Robert Willan and the Birth of Dermatology
The first major step toward recognizing psoriasis as a distinct clinical entity came from the English physician Robert Willan (1757–1812), often called the "father of dermatology." Working in London at the turn of the nineteenth century, Willan set out to do for skin disease what Linnaeus had done for plants: impose an orderly, observation-based classification. In his landmark work On Cutaneous Diseases (the first volume published in 1808), he sorted skin disorders into eight orders based on the appearance of the primary lesion — papules, scales (squamae), exanthemata, bullae, pustules, vesicles, tubercles, and maculae — and he pioneered the use of detailed colored illustrations to fix each disease's appearance for other physicians.
Within this system Willan gave what is generally regarded as the first proper clinical description and classification of psoriasis, placing it among the scaling diseases and distinguishing it from many other eruptions with which it had been muddled. This was a genuine advance: for the first time, the disease was being carefully characterized by its own features rather than absorbed into a vague mass of "scabby skin." Willan's work, continued and published after his death by his colleague Thomas Bateman, became the foundation of British and ultimately Western dermatology.
A crucial nuance must be preserved here, because it is easy to overstate Willan's achievement. Willan did not fully free psoriasis from its entanglement with leprosy. He described the condition under the old Greek-derived heading lepra Graecorum ("leprosy of the Greeks"), and in 1809 he in fact defined two related scaling entities — lepra Graecorum and psora leprosa — that were later shown to be the same disease. In other words, Willan supplied the first rigorous description and a powerful classifying method, and he began the separation of psoriasis from other diseases, but he still framed it within the language of "lepra." Completing the separation — and discarding the leprosy label outright — would fall to the next generation.
Ferdinand von Hebra: Separating Psoriasis from Leprosy
The decisive break came in 1841, when the Viennese dermatologist Ferdinand von Hebra (1816–1880) definitively distinguished psoriasis from leprosy and established the modern disease concept under the name we still use. Hebra recognized that Willan's two supposed entities, lepra Graecorum and psora leprosa, were in reality a single disease, and he gave it the consolidated name psoriasis, deliberately shedding the term lepra that had caused so much confusion and harm. From this point onward, psoriasis and leprosy were understood as two separate diseases — a separation that, after roughly two millennia of conflation, freed psoriasis to be studied and treated on its own terms.
Hebra was no isolated figure but a central founder of the New Vienna School of Dermatology, which became one of the principal sources of modern dermatology. He built his classification of skin diseases on pathological anatomy — that is, on the actual changes in the skin — rather than on humoral theory or superficial resemblance, and his framework was so durable that it shaped dermatological teaching for nearly a century. His insistence on grounding diagnosis in careful clinical and anatomical observation is precisely what allowed psoriasis finally to acquire a fixed, defensible identity.
It is worth holding the three milestones distinct, because they are often blurred together. The name psoriasis is ancient, descending from Greek psora. The first systematic clinical description and classification belongs to Willan around 1808, though still under the "lepra" heading. The definitive separation from leprosy and the establishment of the modern disease concept belongs to Hebra in 1841. Each step was necessary; none alone was sufficient. Recognizing the cause of the disease would take far longer still.
Heinrich Koebner and the Isomorphic Phenomenon
One of the most enduring observations in the history of psoriasis was made by the German dermatologist Heinrich Koebner (1838–1904). In 1872, Koebner described, and presented to the Silesian Society for National Culture, his observation that physical injury to otherwise healthy skin in a person with psoriasis could trigger new psoriatic lesions at the exact sites of trauma. He documented the appearance of fresh plaques following insults such as scratches, tattoos, and even a horse bite — new lesions that arose precisely where the skin had been damaged.
This is now known as the Koebner phenomenon, or the isomorphic response (from the Greek for "equal shape," because the trauma-induced lesions look identical to the patient's existing disease). A patient who develops new psoriasis along a line of injury is "Koebner-positive." The phenomenon is not unique to psoriasis — it is seen in other conditions such as vitiligo and lichen planus — but it is most classically associated with psoriasis and remains a standard clinical concept today.
A small point of historical accuracy is worth noting: Koebner presented the observation in 1872, and accounts of the formal publication of the finding cite dates in the years immediately following. The substance, however, is well established and uncontested — that as early as 1872 Koebner had clearly recognized and demonstrated the trauma-induced appearance of psoriatic lesions. Beyond its clinical usefulness, the phenomenon was an early hint that psoriasis is a reactive disease in which the skin responds abnormally to a stimulus — a clue whose full meaning would only become clear once the immune basis of the disease was understood, more than a century later.
A History of Treatments: Tar, Light, and Beyond
Long before anyone understood what caused psoriasis, physicians and patients accumulated treatments by trial and observation, and a surprising number of these old remedies anticipated approaches still in use. Coal tar applied to the skin was a mainstay for well over a century — Robert Willan himself recommended a topical tar preparation — and tar remains a recognized, evidence-supported topical treatment for psoriasis to this day. The benefit of sunlight was also noticed empirically: many patients improved in summer or with sun exposure, an observation that eventually matured into modern medical phototherapy.
The twentieth century turned these hints into deliberate therapies. In the 1920s, the Goeckerman regimen paired crude coal tar with ultraviolet light, and by the 1970s controlled phototherapy was a cornerstone of treatment — including PUVA (the drug psoralen plus ultraviolet A light) and, later, narrowband UVB. Anthralin (dithranol), high-potency topical corticosteroids (mid-twentieth century), and topical vitamin D analogues such as calcipotriol further expanded the toolkit.
For severe disease, the mid-to-late twentieth century introduced systemic drugs that suppress or modulate the immune response, including methotrexate and ciclosporin, along with oral retinoids. These were genuinely effective for many patients, but they acted broadly across the whole body and carried meaningful risks, which is part of why the eventual shift to precisely targeted therapy — described in the next section — was so significant. Throughout, it is honest to say that none of these treatments cured psoriasis; they controlled it. Psoriasis remains, to this day, a manageable but not curable chronic disease.
The Modern Era: An Immune-Mediated Disease
For most of its history, psoriasis was regarded primarily as a disorder of the skin itself — an abnormality of keratinocytes, the cells that make up the outer epidermis, which in psoriasis multiply far too quickly and pile up as scale. The great conceptual revolution of the late twentieth and early twenty-first centuries was the recognition that psoriasis is fundamentally an immune-mediated disease: the runaway skin growth is driven by an inappropriately activated immune system, in particular by T cells (a class of white blood cell) and the inflammatory signals they orchestrate. The skin changes, in this modern view, are the downstream result of an immune process, not the primary fault.
Research over the past two decades has mapped this process in remarkable detail and identified a central signalling pathway now known as the IL-23/IL-17 axis. In simplified terms, immune cells release the cytokine interleukin-23 (IL-23), which sustains a population of T-helper cells (the Th17 subset) that in turn release interleukin-17 (IL-17); IL-17 then drives keratinocytes to proliferate and to recruit yet more inflammation, producing the characteristic thick, red, scaly plaques. This pathway is the modern scientific explanation for the disease, and it is supported by a large and consistent body of immunological evidence. It is also why an old clue — the Koebner phenomenon — finally made sense: trauma can locally trip this primed immune circuit.
Understanding the pathway transformed treatment. Beginning in the early 2000s, the first biologic drugs — antibodies and engineered proteins designed to neutralize specific immune molecules — reached patients with psoriasis. The first biologic agents sanctioned for psoriasis in the United States, alefacept and efalizumab, were approved in 2003, and the first TNF-inhibitor biologic for psoriasis, etanercept, followed in 2004; later generations of biologics were designed to block IL-17 or IL-23 directly. For many patients with severe disease, these targeted therapies achieve degrees of skin clearance that earlier eras could scarcely imagine. Two points deserve emphasis for accuracy: psoriasis is not contagious — it cannot be caught or passed on — and despite these advances it still cannot be cured, only controlled, sometimes very well.
Legacy: From Stigma to Science
The history of psoriasis is, in large part, a history of misunderstanding slowly giving way to knowledge — and of the human cost exacted while that misunderstanding lasted. For nearly two thousand years the disease had a name borrowed from the Greek word for "itch" but no settled identity, and the people who carried it were repeatedly mistaken for lepers and made to bear the stigma, isolation, and moral judgment heaped upon leprosy. The arc from Willan's classification, through Hebra's separation of the disease from leprosy, to the discovery of its immune basis is therefore not only a scientific story but a moral one: each advance returned a measure of clarity and dignity to those affected.
That legacy of stigma has not vanished. Because psoriasis is visible, chronic, and still widely misunderstood by the public, many people with the disease continue to face social discomfort, mistaken fears of contagion, and a real psychological burden. Modern dermatology and patient-advocacy organizations now treat the emotional and social dimensions of psoriasis as part of proper care — a direct, conscious response to the centuries during which the disease was treated as a mark of shame rather than as the medical condition it is.
Seen as a whole, the long history of psoriasis offers an encouraging lesson: a disease can be carefully described (Willan), correctly distinguished from its mimics (Hebra), have its telltale behaviors observed (Koebner), and finally have its true cause uncovered (the immune-mediated, IL-23/IL-17 model) — each step building on the last across many generations. For a fuller account of how psoriasis is recognized, classified, and treated today, see the main Psoriasis article.
Research Papers and References
The references below combine peer-reviewed historical and scientific literature with curated PubMed topic-search links into the history, classification, and immunology of psoriasis. Historical primary sources — the works of Galen and Celsus, Robert Willan's On Cutaneous Diseases (1808), and the writings of Ferdinand von Hebra and Heinrich Koebner — are named in the article as historical sources rather than as modern citations. Each PubMed link opens at the National Library of Medicine in a new tab.
- Glickman FS. Lepra, psora, psoriasis. Journal of the American Academy of Dermatology. 1986;14(5 Pt 1):863–866. — PubMed: Lepra, psora, psoriasis
- Benedek TG. Psoriasis and psoriatic arthropathy: historical aspects. Journal of Clinical Rheumatology. — PubMed: psoriasis historical aspects
- Historical review — psoriasis from antiquity to the present (etymology, leprosy confusion, Willan, Hebra). — PubMed: psoriasis history antiquity to present
- Robert Willan and the classification of cutaneous disease (the founding of dermatology). — PubMed: Robert Willan classification of cutaneous diseases
- Ferdinand von Hebra and the New Vienna School of Dermatology. — PubMed: Ferdinand von Hebra and the Vienna school
- Sagi L, Trau H. The Koebner phenomenon. Clinics in Dermatology. 2011;29(2):231–236. — doi:10.1016/j.clindermatol.2010.09.014
- Weiss G, Shemer A, Trau H. The Koebner phenomenon: review of the literature. Journal of the European Academy of Dermatology and Venereology. 2002;16(3):241–248. — PubMed: Koebner phenomenon review
- Boehncke WH, Schon MP. Psoriasis. The Lancet. 2015;386(9997):983–994. — doi:10.1016/S0140-6736(14)61909-7
- Lowes MA, Suarez-Farinas M, Krueger JG. Immunology of psoriasis. Annual Review of Immunology. 2014;32:227–255. — doi:10.1146/annurev-immunol-032713-120225
- Girolomoni G, Strohal R, Puig L, et al. The role of IL-23 and the IL-23/TH17 immune axis in the pathogenesis and treatment of psoriasis. Journal of the European Academy of Dermatology and Venereology. 2017;31(10):1616–1626. — doi:10.1111/jdv.14433
- Hawkes JE, Chan TC, Krueger JG. Psoriasis pathogenesis and the development of novel targeted immune therapies. Journal of Allergy and Clinical Immunology. 2017;140(3):645–653. — doi:10.1016/j.jaci.2017.07.004
- History of biologic therapy and the targeted-treatment era in psoriasis (alefacept, efalizumab, etanercept). — PubMed: history of biologic therapy in psoriasis
- History of psoriasis treatment: coal tar, anthralin, phototherapy, and PUVA. — PubMed: history of psoriasis treatment
- The social stigma and psychological burden of psoriasis: historical and modern perspectives. — PubMed: psoriasis stigma and psychological burden