Fungal Infections: History and Discovery
The history of fungal infections holds a strange honor: the diseases caught by the skin were among the very first illnesses ever proven to be caused by a living germ. Long before Louis Pasteur and Robert Koch built the germ theory of disease around bacteria, a young Hungarian-born physician working in Paris — David Gruby — took the scaly, ring-shaped patches that country people had always blamed on "worms" and showed, under the microscope and in deliberate experiments, that they were really gardens of fungus. This page traces that story: from the ancient misnomer "ringworm" (there is no worm), through the 1830s and 1840s discoveries of favus and ringworm fungi that quietly opened the door to modern microbiology, through Raymond Sabouraud's great cataloguing of the dermatophytes and the culture jelly that still bears his name, to griseofulvin and the antifungal drugs that finally gave physicians a cure — and the modern, sobering rise of deadly fungal infections in people whose immune systems are weakened.
Table of Contents
- "Ringworm" Is a Misnomer: The Names and the Diseases
- Ancient Records: Thrush, Tinea, and the Honeycomb Scalp
- Bassi, Schonlein, and Remak: The 1830s Breakthrough
- David Gruby: Proving a Fungus Causes Human Disease
- Raymond Sabouraud and the Birth of Medical Mycology
- Candida, Thrush, and the Yeast Within
- The Search for a Cure: Griseofulvin and the Antifungals
- The Modern Era: Fungi and the Weakened Immune System
- Research Papers and References
- Connections
- Featured Videos
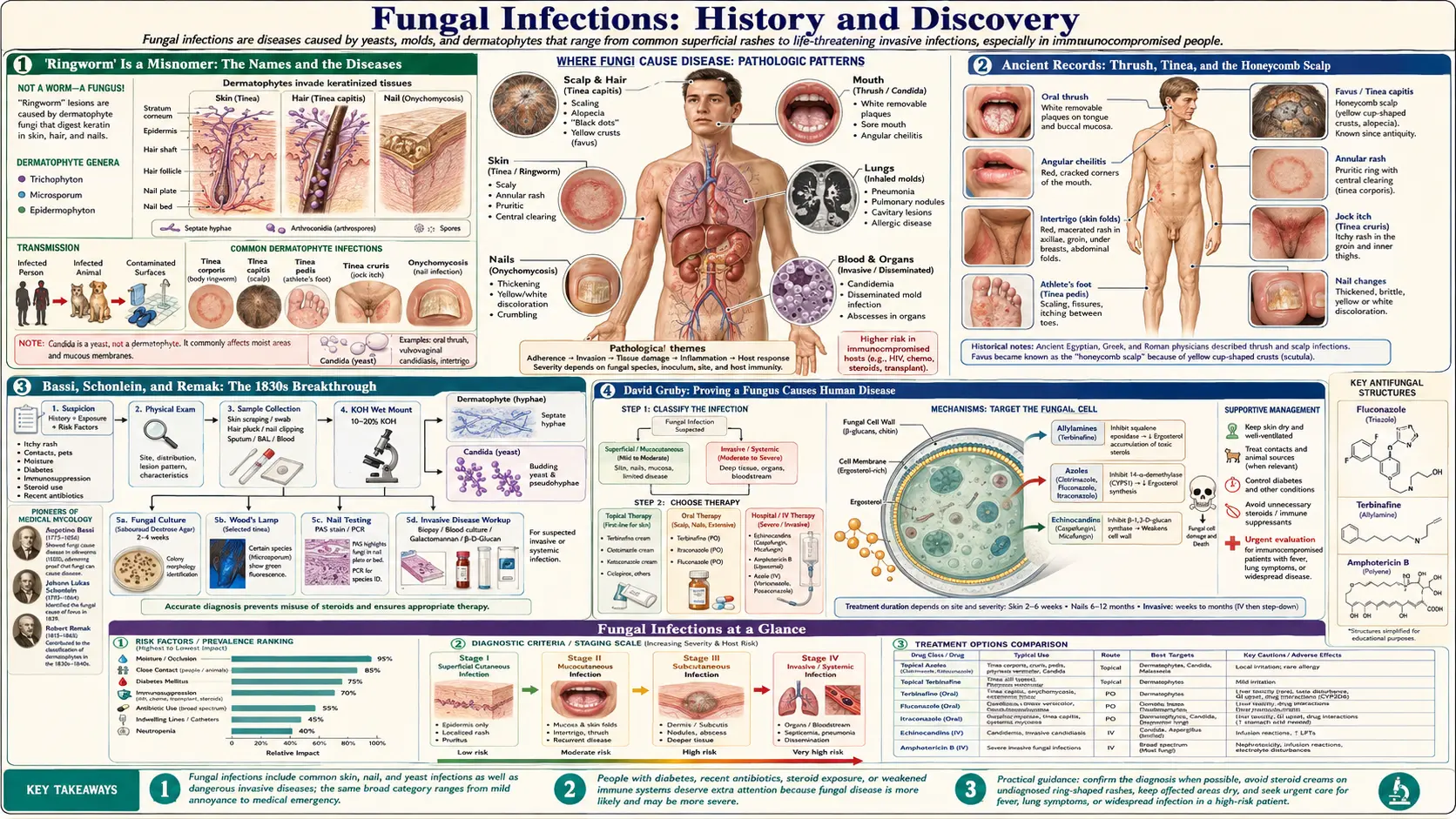
"Ringworm" Is a Misnomer: The Names and the Diseases
The single most important thing to understand about the history of these infections is that the most familiar name for them is wrong. Ringworm is not a worm. There is no parasite burrowing under the skin, no creature to pull out — the round, red, scaly, slowly-expanding patch that earned the name is caused entirely by microscopic fungi. The name survives only because, to the unaided eye of a medieval observer, the ring-shaped rash with its raised, advancing border and clearer healing center genuinely looked as though a small worm were coiled beneath the surface, crawling outward in a circle. That visual guess, made centuries before anyone could see a fungus, became fixed in everyday language and has never let go.
The medical name carries the same ancient confusion. Tinea is the Latin word for a gnawing grub or clothes-moth larva — the little creature whose feeding leaves rounded holes in stored wool. Early writers saw a resemblance between those moth-eaten circles in cloth and the rounded, eaten-away patches on infected skin, and so the skin disease inherited the insect's name. To this day physicians label these infections by body site using that 2,000-year-old word: tinea corporis (ringworm of the body), tinea capitis (scalp), tinea pedis (the feet — athlete's foot), tinea cruris (the groin — "jock itch"), and tinea unguium (the nails). The fungi that cause them are collectively the dermatophytes — from the Greek for "skin plants" — molds that feed on keratin, the tough protein of skin, hair, and nail.
A second great family of fungal infection has an equally old and equally misleading common name: thrush, the creamy-white coating of the mouth (or other moist surfaces) caused by the yeast Candida. And a third historical entity, now rare in wealthy countries, is favus — a severe, scarring scalp infection whose crusts were said to resemble a honeycomb (Latin favus, "honeycomb"). It was favus, of all things, that gave science its first clear proof that a germ could cause a human disease.
Ancient Records: Thrush, Tinea, and the Honeycomb Scalp
Fungal infection is as old as humanity, and the written record reaches back to the dawn of medicine. The white mouth-patches of oral thrush appear in the Hippocratic writings of ancient Greece around the fourth century BCE, described under the term aphthae — small white sores of the mouth — in the collection known as the Epidemics. Roughly five centuries later the great physician Galen, writing in the second century CE, again recorded the white oral lesions of infants and the sick. Neither man could have known a yeast was responsible, but their careful clinical descriptions are recognizable to any modern clinician who has seen thrush in a newborn or a frail patient.
Ringworm and the other tineas were likewise familiar to ancient and medieval physicians, who grouped them among the many disfiguring scaly and bald-patch diseases of the scalp and skin without any notion of their cause. The Roman encyclopedist Celsus, in the first century CE, described a boggy, pus-studded scalp inflammation that dermatologists still call by his name — a kerion — which we now know to be an intense reaction to a ringworm fungus. Throughout the medieval and early-modern centuries these conditions were lumped together, confused with one another and with non-fungal diseases, and treated with an enormous and largely useless pharmacopeia of ointments, plasters, and the brutal "pitch-cap" method of tearing out infected hairs.
What all of this pre-modern medicine lacked was any way to see the cause. The compound microscope existed from the seventeenth century, and Antonie van Leeuwenhoek had glimpsed microbes in the 1670s, but the idea that a specific, visible, living organism might be the cause — not merely a companion — of a specific human disease had not yet been demonstrated for anything. That demonstration, when it finally came in the 1830s and 1840s, came not from the study of plague or fever but from the unglamorous diseases of the skin and scalp.
Bassi, Schonlein, and Remak: The 1830s Breakthrough
The story of proof begins not with a human patient but with a silkworm. In 1835 the Italian naturalist Agostino Bassi published the result of years of patient work showing that muscardine, a devastating disease that turned silkworms into stiff, white, mummified husks, was caused by a microscopic fungus (later named Beauveria bassiana in his honor) — and that the disease could be transmitted from a sick worm to a healthy one. This is widely regarded as the first time anyone demonstrated that a microorganism causes an infectious disease in any animal. Bassi's work predates Pasteur's germ-theory experiments by roughly a generation, and it established the crucial principle that a living, transmissible germ could be a cause of disease rather than a mere byproduct of it.
The leap to human disease followed almost immediately, and it centered on favus, the honeycomb scalp infection. In 1839 the German physician Johann Lukas Schonlein published a famously brief note — reportedly only about twenty lines, in the journal known as Muller's Archiv — reporting that the yellow crusts of favus contained a fungus. Favus is generally credited as the first human disease in which a fungal cause was clearly identified, and the organism was eventually named Achorion schoenleinii in Schonlein's honor (it is known today as Trichophyton schoenleinii).
The picture is complicated, and historians have argued about it for over a century, by the parallel work of Robert Remak — better remembered today as a pioneering neurologist and embryologist. Remak saw the microscopic structures inside favus crusts as early as the mid-1830s but did not at first recognize them as a fungus. He later became Schonlein's assistant, cultivated the favus organism on apple slices, and is credited with first proposing the name Achorion schoenleinii — generously assigning the honor of the discovery to his teacher Schonlein rather than claiming priority for himself. The exact division of credit between the two men remains one of the classic priority puzzles in the history of medicine; what is not in dispute is that, by the end of the 1830s, favus had become a fungal disease in the eyes of science.
David Gruby: Proving a Fungus Causes Human Disease
If Schonlein and Remak opened the door, it was David Gruby (1810–1898) who walked through it and turned the observation into rigorous, repeatable proof. Born in a poor Jewish family in what is now Hungary, Gruby studied medicine in Vienna and settled in Paris, where in the early 1840s — working largely on his own and demonstrating his findings before the French Academy of Sciences — he produced a remarkable series of papers on the fungi of skin disease. Across roughly 1841 to 1844 he described the fungus of favus, the fungus of common ringworm of the scalp, the organism of the beard infection now called Trichophyton, and the yeast of oral thrush.
What sets Gruby apart is the completeness of his method. He did not merely note that fungi were present in diseased tissue; he isolated the favus fungus from a patient, grew it on slices of potato, and then deliberately inoculated it onto healthy skin and reproduced the disease — a logical sequence (find the organism, culture it, reproduce the disease with the culture) that anticipates by decades the formal "postulates" later associated with Robert Koch. In demonstrating this, Gruby's experiments are frequently described as among the first ever to prove that a specific microorganism is the cause of a specific human disease. He did this in the early 1840s — roughly two decades before Pasteur's decisive germ-theory work and a full generation before Koch's famous studies of anthrax and tuberculosis.
Gruby's genius went strangely unrewarded in his own time. Much of the medical establishment was slow to accept that a humble mold could cause disease, and Gruby himself, an eccentric who eventually drifted away from mycology into a fashionable Paris medical practice and into wide-ranging experiments, did little to press his claims. His discoveries were neglected and in some cases re-discovered by others later in the century. Only in retrospect did historians recognize that the foundations of medical mycology — and one of the earliest demonstrations of the germ theory of disease itself — had been laid by this overlooked physician working on the diseases of the scalp. Several dermatophyte species he first described, such as Microsporum audouinii (a major cause of childhood scalp ringworm), still carry forward the work he began.
Raymond Sabouraud and the Birth of Medical Mycology
For half a century after Gruby, the study of skin fungi was a confusing tangle. Different observers described what seemed to be different organisms, gave them different names, and could not agree on how many kinds of "ringworm fungus" actually existed, because they had no reliable, standardized way to grow the molds and compare them. The man who brought order to the chaos was the French dermatologist Raymond Jacques Adrien Sabouraud (1864–1938), working at the Hopital Saint-Louis in Paris — the great Parisian center of skin medicine — from the 1890s onward.
Sabouraud's achievement was twofold. First, he undertook a vast, systematic study of the dermatophytes, cultivating them in pure culture, drawing and photographing their microscopic structures, and sorting them into a rational classification. His monumental 1910 book on the ringworm diseases, Les Teignes ("The Tineas"), grouped the causative fungi into the genera Trichophyton, Microsporum, Epidermophyton, and Achorion — three of which remain the working categories mycologists use today. This work is so foundational that it is often described as the true starting point of medical mycology as a science.
Second — and this is the part every clinical microbiology laboratory still relies on — Sabouraud developed a culture medium specifically suited to growing these fungi. A nutrient jelly of peptone and sugar (glucose/dextrose) at an acidic pH that favors fungi while discouraging many bacteria, it is known to this day as Sabouraud dextrose agar (or Sabouraud glucose agar), abbreviated SDA. More than a century after he formulated it, "Sab agar" remains a first-line medium for culturing dermatophytes, Candida, and many other medically important fungi — an unusually direct line from a single nineteenth-century dermatologist's bench to the modern hospital lab. Sabouraud also pioneered the careful clinical and microscopic distinctions between the various tineas and developed early treatments for scalp ringworm, including the use of controlled X-ray epilation to shed infected hairs in an era before any antifungal drug existed.
Candida, Thrush, and the Yeast Within
Running alongside the story of the dermatophytes is the parallel history of Candida, the yeast of thrush. As noted above, the white oral patches were recorded by Hippocrates and Galen in antiquity, but the modern understanding began in the nineteenth century. After Gruby observed the thrush organism in the 1840s, a series of investigators worked out that the white plaques of the mouth, the diaper area, and the female genital tract were all caused by a budding yeast. The organism passed through a long parade of names — including Oidium albicans and Monilia albicans — before twentieth-century mycologists settled on the genus name Candida (from the Latin for "glowing white," the same root as "candid" and "candle"), with the principal species being Candida albicans (albicans meaning "whitening").
What makes Candida historically and medically distinct from the dermatophytes is that it is not really an invader from outside at all. Candida albicans is a normal, quiet resident of the mouth, gut, and skin in a large fraction of perfectly healthy people — a commensal. It causes disease only when the balance tips: when antibiotics wipe out competing bacteria, when hormones shift in pregnancy, when blood sugar runs high in diabetes, when dentures or moisture change the local environment, or — most dramatically — when the immune system is suppressed. This made candidiasis the original "disease of opportunity," and it is the reason thrush has always tracked the vulnerable: the newborn, the elderly, the diabetic, the cancer patient, and, in the late twentieth century, a wholly new and tragically large population.
The Search for a Cure: Griseofulvin and the Antifungals
For all the brilliance of the nineteenth-century discoveries, they did not produce a cure. Through the first half of the twentieth century, ringworm of the scalp — a common, contagious, and disfiguring affliction of schoolchildren — was still treated with the crude methods of an earlier age: topical antiseptics, sulfur and tar, the manual or chemical removal of hairs, and X-ray epilation, none of which reliably killed the fungus inside the hair shaft. The arrival of a true cure for the dermatophyte infections is the story of griseofulvin.
Griseofulvin was first isolated in 1939 by the British scientist Harold Raistrick and colleagues (commonly credited to "Oxford and co-workers") from the mold Penicillium griseofulvum — but at the time no one realized it could treat human ringworm. Its antifungal activity against molds was studied in the 1940s (Brian, Hemming, and colleagues observed that it stunted and distorted fungal growth), and through the 1950s its chemical structure was worked out. The decisive moment came in 1958, when J. C. Gentles, working in Scotland, showed that griseofulvin taken by mouth could cure ringworm infections in guinea pigs — proving that the drug was absorbed, carried in the body, and deposited into the keratin of skin and hair where it poisoned the fungus from within. Human trials followed rapidly, and griseofulvin was introduced as an oral medicine for ringworm around 1959. For the first time in history, a child with scalp ringworm could simply swallow a pill and be cured. It works by binding fungal tubulin and jamming the microtubule machinery of cell division.
Griseofulvin was the beginning, not the end. The mid-twentieth century also produced amphotericin B (from a soil bacterium, introduced in the 1950s), a powerful but toxic intravenous drug that for decades was the mainstay against severe internal fungal infections, and nystatin, a topical anti-yeast agent. From the 1960s and 1970s onward came the great class of the azoles — beginning with topical agents such as clotrimazole and miconazole, then the orally active ketoconazole, and in the 1980s and 1990s the safer, widely used fluconazole and itraconazole that transformed the treatment of both thrush and deeper infections. Later still came terbinafine (an allylantifungal highly effective for nail and skin dermatophytes) and, around the turn of the millennium, the echinocandins for serious invasive disease. In the span of a single human lifetime, fungal infection went from essentially untreatable to broadly curable.
The Modern Era: Fungi and the Weakened Immune System
The triumph of antifungal drugs coincided, cruelly, with the emergence of whole new populations of severely susceptible patients — and so the late twentieth century saw fungal infections become, if anything, a larger and deadlier problem than before, even as the common skin infections grew easy to treat. Modern medicine itself created much of the vulnerability: cancer chemotherapy that wipes out the immune cells, organ and bone-marrow transplants that require lifelong immune suppression, long stays in intensive care with intravenous lines and broad-spectrum antibiotics, and the wide use of corticosteroids all open the body to fungi that a healthy immune system shrugs off.
Above all, the HIV/AIDS epidemic, which emerged in the early 1980s, brought fungal infection to global prominence in a way nothing had before. In a person whose immune defenses have collapsed, organisms that are ordinarily harmless turn lethal: stubborn oral and esophageal thrush from Candida became a hallmark of advancing AIDS, and other fungi — the lung-and-brain yeast Cryptococcus, the pneumonia organism Pneumocystis, and regional molds such as Histoplasma — became defining opportunistic infections of the disease. Invasive fungal disease carries a high mortality even today, and worldwide it still causes an enormous toll of illness and death, concentrated among people with weakened immunity. The arrival of effective antiretroviral therapy, which restores immune function, has sharply reduced these infections in people with well-treated HIV — a reminder that the body's own defenses remain the most important antifungal of all.
The history of fungal infection, then, runs full circle. It began with diseases of the skin so visible and so common that ancient people invented a worm to explain them; it produced, almost by accident, one of the first proofs that a germ can cause human disease; it matured into the science of medical mycology and finally into real cures; and it now confronts, with that hard-won knowledge, the serious fungal threats faced by the growing number of people whose immune systems — through disease or through the very treatments that keep them alive — can no longer hold these ancient organisms in check. The story is far from finished: drug-resistant fungi such as Candida auris, and the broader recognition of fungi as a neglected global health threat, are writing its newest chapters now.
Research Papers and References
The references below combine peer-reviewed historical reviews with curated PubMed topic-search links into the history of medical mycology, dermatophytes, and candidiasis. Historical primary sources (the Hippocratic Epidemics; Schonlein's 1839 note in Muller's Archiv; Gruby's papers before the French Academy of Sciences in the early 1840s; and Sabouraud's Les Teignes, 1910) are named in the article as historical sources rather than as modern citations. Each link opens at the publisher or at PubMed (National Library of Medicine) in a new tab.
- Homei A, Worboys M. Fungal Disease in Britain and the United States 1850–2000: Mycoses and Modernity. Palgrave Macmillan; 2013. (Open-access monograph, NCBI Bookshelf) — NCBI Bookshelf: Fungal Disease in Britain and the United States
- Seeliger HPR. The discovery of Achorion schoenleinii: facts and "stories." Mycoses. 1985;28(4):161–182. — doi:10.1111/j.1439-0507.1985.tb02110.x
- Homolka S, et al. Robert Remak (1815–1865): discoverer of the fungal character of dermatophytoses. Clinics in Dermatology. 2013;31(6):797–800. — PubMed 24312990
- Etymologia: Dermatophyte. Emerging Infectious Diseases. 2020;26(9):2289. — doi:10.3201/eid2609.ET2609
- Hay RJ. Cutaneous, subcutaneous and systemic mycology (history and overview). (PMC) — PMC7122059
- Aris P, et al. Griseofulvin: an updated overview of old and current knowledge. Molecules. 2022;27(20):7034. — doi:10.3390/molecules27207034
- Gentles JC. Experimental ringworm in guinea pigs: oral treatment with griseofulvin. Nature. 1958;182(4633):476–477. — PubMed: Gentles griseofulvin guinea pigs ringworm (1958)
- Vila T, et al. Oral candidiasis: a disease of opportunity. Journal of Fungi. 2020;6(1):15. — doi:10.3390/jof6010015
- Barnett JA. A history of research on yeasts 12: medical yeasts part 1, Candida albicans. Yeast. 2008;25(6):385–417. — doi:10.1002/yea.1595
- Revisiting the history of candidiasis (historical review, PMC, 2024). — PMC11909613
- Agostino Bassi, muscardine, and the origins of the germ theory of disease — PubMed: Agostino Bassi muscardine germ theory history
- David Gruby and the history of medical mycology — PubMed: David Gruby history of medical mycology
- Raymond Sabouraud and the taxonomy of the dermatophytes — PubMed: Sabouraud dermatophyte taxonomy history
- Invasive fungal infection in immunocompromised and HIV/AIDS patients (epidemiology and history) — PubMed: invasive fungal infection in immunocompromised and HIV/AIDS
External Authoritative Resources
- CDC — Fungal Diseases
- MedlinePlus — Fungal Infections
- PubMed — History of medical mycology (Gruby, Sabouraud, dermatophytes)
Connections
- Dermatology
- Fungal Infections (overview)
- All Conditions
- Eczema
- Psoriasis
- Cellulitis
- HIV / AIDS
- Tuberculosis