Thromboangiitis Obliterans (Buerger's Disease)
- Overview
- Epidemiology and Geographic Distribution
- Pathophysiology — Tobacco-Driven Inflammatory Vasculitis
- Clinical Presentation — The Classic Triad
- Diagnosis and Angiographic Findings
- Differential Diagnosis
- Treatment — Tobacco Cessation as the Cornerstone
- Advanced and Experimental Therapies
- Prognosis and Amputation Risk
- Research Papers
- Connections
- Featured Videos
Overview
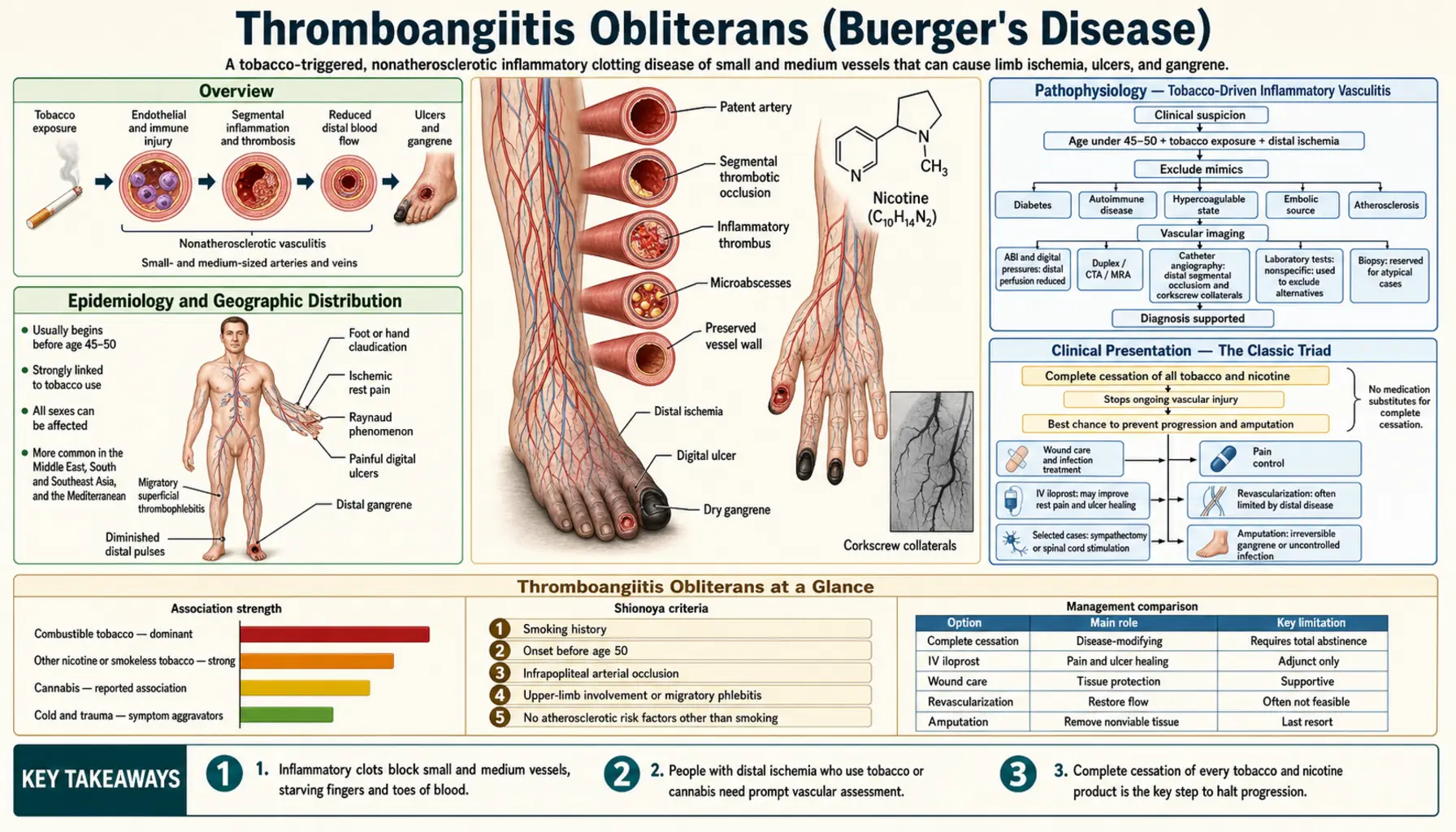
Thromboangiitis obliterans, commonly known as Buerger's disease, is a nonatherosclerotic segmental inflammatory vasculitis that affects the small and medium-sized blood vessels of the hands and feet. Unlike the vast majority of vascular diseases, it has one single overwhelmingly dominant cause: tobacco use. Every confirmed case involves a patient who currently or formerly used tobacco in some form — cigarettes, cigars, pipes, chewing tobacco, or smokeless products. The disease does not require any of the classic cardiovascular risk factors such as diabetes, high blood pressure, or elevated cholesterol. It strikes young people who otherwise appear healthy, except for their tobacco habit.
The disease was described definitively by Leo Buerger, a New York surgeon, in 1908. He recognized a pattern of premature gangrene of the extremities in young male immigrants from Eastern Europe and identified the unique pathological features — an inflammatory thrombus inside the vessel with a relatively preserved vessel wall architecture — that distinguished this condition from ordinary hardening of the arteries.
What makes Buerger's disease both tragic and treatable is that complete cessation of all tobacco products is the only effective treatment. Patients who stop completely typically halt the disease in its tracks. Those who continue smoking face a relentless march of vessel closure, digital ulcers, gangrene, and progressive amputations. Even resuming tobacco use after a period of abstinence can trigger immediate relapse. The message in Buerger's disease is unusually clear: the tobacco is the disease.
Epidemiology and Geographic Distribution
Buerger's disease predominantly affects young male smokers, with onset typically between ages 20 and 45. The classic patient is a young man who has been a heavy smoker since adolescence and presents with foot pain, toe ulcers, or digital gangrene at an age when most people have no vascular disease at all. This young age of onset is itself a diagnostic clue — peripheral artery disease from atherosclerosis rarely presents before age 50.
Historically, the male-to-female ratio has been reported as high as 3:1. However, as smoking rates among women have risen globally, the proportion of female patients has increased. In some modern series, women now account for 20 to 30 percent of cases, and the disease in women often presents with upper extremity involvement more prominently than in men.
The disease shows striking geographic variation that directly mirrors heavy tobacco use patterns. In Western Europe and North America, where smoking rates have been declining for decades, Buerger's disease accounts for only 0.5 to 5.6 percent of peripheral vascular disease cases in most series. In contrast, in Southeast Asia, India, the Middle East, and Eastern Europe — regions with historically higher smoking rates and where tobacco cessation programs are less established — Buerger's disease can account for 45 to 63 percent of all peripheral vascular disease in some hospital series. This enormous geographic difference is not a genetic phenomenon; it reflects the local prevalence of tobacco use.
The incidence of Buerger's disease in Western countries has declined significantly over the past several decades, a direct consequence of falling smoking rates. This natural experiment provides some of the strongest indirect evidence that tobacco is the sole cause. When a population smokes less, Buerger's disease becomes rarer.
Pathophysiology — Tobacco-Driven Inflammatory Vasculitis
Buerger's disease is driven by a cellular immune response to tobacco antigens. Something in tobacco — the exact molecule or molecules remain under investigation — triggers the body's immune system to attack the walls of small and medium blood vessels in the extremities. This is not the same process as atherosclerosis, where cholesterol plaques gradually build up inside vessel walls over decades. In Buerger's disease, the vessels themselves remain architecturally intact even as they fill with inflammatory clot material from the inside.
This preserved vessel wall architecture is one of the key pathological features that distinguishes Buerger's disease from every other form of peripheral vascular disease. When a pathologist examines an affected vessel under the microscope, the layers of the vessel wall — the intima, media, and adventitia — remain recognizable and relatively undamaged. What fills the inside of the vessel is a highly cellular inflammatory thrombus containing lymphocytes, giant cells, and collections of inflammatory cells forming microabscesses. This is completely unlike the dead, calcified, cholesterol-laden vessel walls seen in advanced atherosclerosis.
The disease evolves through three overlapping pathological phases. In the acute phase, the vessel lumen fills with this cellular inflammatory thrombus while the vessel wall architecture remains preserved. In the subacute phase, the thrombus begins to organize, and fibroblasts start to replace the inflammatory cells. In the chronic phase, the thrombus recanalizes — small channels form through the organized clot material — and fibrosis gradually replaces the inflammatory tissue. Unfortunately, recanalization in Buerger's disease is often incomplete, and the newly formed channels are too small to restore adequate blood flow.
The disease selects for distal vessels — the tibial and peroneal arteries in the legs, and the radial and ulnar arteries in the arms. The proximal vessels, such as the femoral, popliteal, and brachial arteries, are characteristically spared. This distal distribution is the opposite of what happens in atherosclerosis, which tends to involve the larger, more proximal vessels. The result is ischemia in the most distal parts of the body: the toes, feet, fingers, and hands. Blood cannot reach the digits even though the main arteries of the thigh and upper arm remain open.
As vessels close, the body attempts to build collateral circulation — small new pathways around the blocked segments. In Buerger's disease, these collaterals form in a distinctive coiled, tortuous pattern that resembles a corkscrew when seen on imaging. These corkscrew collaterals are pathognomonic of Buerger's disease and are one of the most characteristic angiographic findings in medicine.
Venous involvement is also part of the disease. The same tobacco-driven inflammatory process can attack superficial veins, causing migratory superficial thrombophlebitis — a painful, red, nodular inflammation that travels from one venous segment to another over time. This venous involvement is seen in about 40 percent of patients and is a distinctive feature that is almost never seen in ordinary atherosclerotic peripheral artery disease.
Clinical Presentation — The Classic Triad
Buerger's disease is characterized by three clinical features that together form a pattern unlike any other vascular disease. Recognizing this triad in a young tobacco user is the key to early diagnosis.
1. Distal Limb Ischemia
The first and most prominent feature is ischemia — inadequate blood supply — in the most distal parts of the limbs. The pattern of ischemia in Buerger's disease is different from what is seen in typical peripheral artery disease. In atherosclerotic PAD, the most common symptom is calf claudication — cramping pain in the calf muscle that occurs during walking and resolves with rest, caused by inadequate blood flow through the diseased femoral or popliteal artery.
In Buerger's disease, the blocked vessels are more distal — in the foot and ankle rather than the thigh. This produces instep claudication: pain in the arch of the foot during walking. Instep claudication is more characteristic of Buerger's disease than calf claudication and should immediately raise suspicion in a young smoker. As the disease progresses, patients develop rest pain — constant pain in the foot or hand at rest, typically worse at night — digital ischemia with color changes and loss of sensation in the toes and fingers, digital ulcers at the fingertips and toe tips, and eventually frank gangrene with tissue death.
Upper extremity involvement is common and characteristic. Both the hands and the feet may be affected, sometimes simultaneously. This bilateral and multi-limb pattern is highly unusual in atherosclerotic PAD, which tends to be more asymmetric and lower extremity-predominant. A young patient with toe and finger ulcers at the same time should be evaluated for Buerger's disease.
2. Migratory Superficial Thrombophlebitis
The second feature is migratory superficial thrombophlebitis — episodes of painful, red, tender inflammation along superficial veins. The affected vein feels like a hard cord under the skin. Episodes develop, resolve over one to three weeks, and then recur in a different venous segment — hence the term "migratory." This pattern of superficial venous inflammation occurring in a young smoker with foot problems is almost pathognomonic of Buerger's disease. It is present in approximately 40 percent of patients and is essentially never seen in atherosclerotic peripheral artery disease.
3. Raynaud's Phenomenon
The third feature is Raynaud's phenomenon — cold-triggered episodic vasospasm of the digital vessels causing a characteristic sequence of color changes: the finger or toe turns white (pallor from vessel spasm cutting off blood flow), then blue (cyanosis from deoxygenated blood pooling in the capillaries), then red (reactive hyperemia as blood flow returns). Raynaud's phenomenon occurs in approximately 40 percent of patients with Buerger's disease. Although Raynaud's phenomenon has many causes, its presence alongside distal ischemia and migratory phlebitis in a young tobacco user creates a very specific clinical picture.
The profile of the typical Buerger's patient brings these features together: a man or woman under age 45, a heavy tobacco user since adolescence, presenting with foot or hand pain, toe or finger ulcers or gangrene, episodes of painful superficial vein inflammation, and Raynaud's phenomenon — with no diabetes, no high blood pressure, no elevated cholesterol, and no family history of premature atherosclerosis. This combination should prompt immediate evaluation and the cessation conversation.
Diagnosis and Angiographic Findings
Buerger's disease is primarily a clinical diagnosis. There is no single blood test or scan that definitively confirms it. Instead, the diagnosis rests on satisfying a set of criteria that include the right clinical picture plus the exclusion of other diseases that can look similar.
The most widely used diagnostic framework is the Olin criteria (2000), which require all of the following:
- Age under 45 at onset
- Current or recent tobacco use
- Distal limb ischemia — claudication, rest pain, ischemic ulcers, or gangrene confirmed by non-invasive vascular testing
- Exclusion of proximal atherosclerosis (normal proximal vessels on imaging)
- Exclusion of a hypercoagulable state (normal coagulation testing)
- Exclusion of an embolic source (normal echocardiogram and proximal arterial imaging)
- Consistent angiographic findings in affected and clinically uninvolved limbs
Angiography and CT angiography are the key imaging tests. The findings in Buerger's disease are distinctive and include: distal vessel occlusion in the tibial, peroneal, and digital arteries of the legs, and in the radial, ulnar, and digital arteries of the hands; sparing of proximal vessels with no atherosclerotic plaque; and most importantly, the corkscrew collaterals — coiled, tortuous small vessels forming around occluded segments. These corkscrew collaterals are the pathognomonic angiographic sign of Buerger's disease. They represent the body's failed attempt to route blood around blocked segments, and their distinctive shape is caused by the fact that the occluded vessel itself is otherwise structurally preserved, so collaterals form along the outside of the vessel in a helical pattern.
Duplex ultrasound can confirm distal vessel involvement and document preserved proximal flow, but lacks the resolution to show the corkscrew collaterals that angiography reveals.
Laboratory testing is used primarily for exclusion. The following tests are standard:
- Lipid panel and fasting glucose — to exclude atherosclerosis risk factors (these are typically normal in Buerger's)
- ANA, ANCA, anti-cardiolipin antibodies, complement levels — to exclude other vasculitides such as lupus, granulomatosis with polyangiitis, or antiphospholipid syndrome (these are typically negative in Buerger's)
- Hypercoagulable panel (protein C, protein S, factor V Leiden, antithrombin III) — to exclude inherited clotting disorders
- Echocardiogram — to exclude a cardiac source of emboli
- Urine cotinine — cotinine is a metabolite of nicotine that persists in the urine for days after tobacco or nicotine exposure; it confirms current use and is essential for verifying the tobacco exposure that defines the diagnosis
The exclusion of other vasculitides is particularly important because some of them — especially granulomatosis with polyangiitis and polyarteritis nodosa — can also cause distal vessel inflammation in young patients. Negative ANCA testing, the absence of systemic features such as kidney disease or sinus involvement, and the specific pattern of distal involvement combined with a heavy tobacco history point away from these alternative diagnoses.
Differential Diagnosis
Several conditions can mimic Buerger's disease and must be actively excluded before the diagnosis is confirmed.
Atherosclerotic peripheral artery disease is the most common alternative diagnosis. It typically occurs in older patients (over 50), with the classic cardiovascular risk factors — smoking, diabetes, hypertension, hyperlipidemia. Atherosclerotic PAD involves the proximal vessels (aorta, iliac, femoral, popliteal) rather than the distal ones, produces calf claudication rather than instep claudication, does not cause migratory phlebitis, rarely involves the upper extremities, and shows vessel wall calcification and plaque on imaging rather than the clean walls seen in Buerger's.
Arterial thromboembolism from a cardiac or aortic source can cause acute limb ischemia resembling Buerger's. The key distinguishing features are an identifiable embolic source on echocardiogram or aortic imaging, acute rather than gradual onset, and positive hypercoagulable testing in some cases. Buerger's disease evolves gradually over months to years, not acutely over hours.
Granulomatosis with polyangiitis (formerly Wegener's) and polyarteritis nodosa are systemic vasculitides that can affect small and medium vessels. They are distinguished from Buerger's by positive ANCA testing (granulomatosis with polyangiitis), systemic involvement of kidneys and sinuses, lack of the specific tobacco connection, and different histological findings on biopsy.
Antiphospholipid syndrome causes recurrent arterial and venous thrombosis and can produce digital ischemia. It is diagnosed by the presence of anti-cardiolipin antibodies, lupus anticoagulant, or anti-beta-2-glycoprotein I antibodies, which are absent in Buerger's disease.
Cryoglobulinemia, often associated with hepatitis C infection, can cause distal vessel inflammation and digital ischemia. Hepatitis C serology and cryoglobulin levels are the distinguishing tests.
Vibration white finger (hand-arm vibration syndrome) is an occupational disease caused by prolonged use of vibrating tools. It produces Raynaud's-like color changes in the fingers but lacks the inflammatory thrombus, migratory phlebitis, and progressive ischemia of Buerger's.
Treatment — Tobacco Cessation as the Cornerstone
The treatment of Buerger's disease begins and ends with one intervention: complete and permanent cessation of all tobacco and nicotine-containing products. This is not a supportive measure or a lifestyle recommendation made alongside drug therapy. It is the only treatment that halts the disease. No medication, no procedure, and no surgery can stop Buerger's disease in a patient who continues to use tobacco. Conversely, complete cessation can arrest the disease, allow ulcers to heal, and prevent progression to major amputation in the majority of patients.
The cessation requirement is absolute. Even a single cigarette can trigger relapse. Patients who believe they have "cut down" substantially but have not stopped completely continue to progress. The mechanism likely involves ongoing tobacco antigen exposure sustaining the cellular immune response that drives the inflammatory thrombus formation.
The role of nicotine replacement therapy in Buerger's disease is debated. Some experts argue that any nicotine perpetuates the disease and that nicotine replacement patches or gum should be avoided. Others contend that nicotine replacement is far safer than continued smoking and that a strategy of gradual reduction using replacement therapy is better than continued cigarette use. The safest and most broadly recommended approach is complete nicotine abstinence — stopping tobacco AND nicotine replacement simultaneously. The role of vaping and electronic cigarettes is unclear; given that e-cigarettes deliver nicotine and contain other potentially inflammatory compounds, avoidance is generally recommended until more data are available.
Wound care for digital ulcers and gangrenous tissue is a critical component of management. Digital wounds require meticulous local care — gentle cleaning, infection surveillance, antibiotic treatment if infection develops, and conservative debridement of necrotic tissue. Aggressive debridement or surgical amputation of non-gangrenous tissue is avoided; the goal is limb salvage with careful wound management while cessation arrests the underlying disease. Patients must also protect their extremities from cold exposure, trauma, and pressure that could worsen ischemia.
Iloprost, an intravenous prostacyclin analog, is the best-studied pharmacological treatment for Buerger's disease. Iloprost causes vasodilation and inhibits platelet aggregation, improving blood flow to ischemic digits. It has been shown in clinical trials, including the landmark TAO Study published in The Lancet in 1990, to reduce the rate of amputation compared to aspirin alone in patients with critical limb ischemia from Buerger's disease. It is approved in Europe specifically for this indication and is typically administered as an intravenous infusion over 5 to 28 days in a hospital or clinic setting. An inhaled form is also available. Iloprost does not cure Buerger's disease and does not replace cessation, but it can provide meaningful benefit during critical ischemia while the patient undertakes cessation.
Calcium channel blockers such as nifedipine or amlodipine are used for the Raynaud's component of Buerger's disease. They reduce vasospasm triggered by cold exposure and can help manage episodic color changes and cold sensitivity in the fingers and toes.
Anticoagulation with heparin or warfarin has not been shown to benefit Buerger's disease specifically. The inflammatory thrombus in Buerger's is not an ordinary blood clot that anticoagulants can dissolve or prevent; it is an organized inflammatory process. Anticoagulation may be used in individual patients with documented thrombotic complications, but it is not a standard treatment for Buerger's disease itself.
Antiplatelet therapy with aspirin or clopidogrel is commonly prescribed but lacks definitive evidence of benefit specific to Buerger's disease. It is often used pragmatically given the low risk of these medications and the possibility of some benefit through platelet inhibition in the microcirculation.
Surgical revascularization — bypass surgery or angioplasty — is limited by the distal, small-vessel nature of the disease. The vessels that need to be bypassed or reopened are often too small and too diffusely involved to be amenable to standard surgical techniques. Endovascular recanalization has been attempted in some centers with selected patients and can provide temporary benefit, but results are generally poor compared to those achieved in atherosclerotic PAD.
Advanced and Experimental Therapies
For patients whose disease progresses despite cessation, or who present with severe critical ischemia threatening major limb loss, several advanced and experimental approaches have been developed.
Spinal cord stimulation involves implanting an electrical stimulation electrode at the thoracic level of the spinal cord. The electrical stimulation modulates the sympathetic nervous system, reducing the sympathetic tone that contributes to vasoconstriction and microvascular spasm. In patients with Buerger's disease, spinal cord stimulation has been shown to reduce ischemic rest pain, improve wound healing in some ulcers, and reduce the need for analgesics. It is particularly useful for refractory rest pain when other measures have failed and amputation is being considered. The device is implanted by a pain specialist or neurosurgeon and can be adjusted externally.
Chemical sympathectomy — ablation of the sympathetic ganglia controlling blood vessel tone — has been used for decades in Buerger's disease. Lumbar sympathectomy improves blood flow to the legs and feet; cervical or thoracic sympathectomy improves flow to the hands and arms. Chemical ablation using alcohol or phenol injection under fluoroscopic guidance avoids open surgery. The benefit is often temporary, lasting months to a year, but can provide meaningful relief of pain and improved digital perfusion during a critical window while cessation takes effect.
Stem cell therapy using autologous bone marrow mononuclear cells is one of the most promising emerging approaches. The patient's own bone marrow is harvested, the mononuclear cells — which include stem cells capable of forming new blood vessels — are concentrated, and then injected directly into the ischemic muscle of the affected limb. The injected cells promote angiogenesis, the formation of new small blood vessels, and can partially restore perfusion to ischemic tissue. Clinical trials, including a study by Durdu and colleagues published in the Journal of Vascular Surgery in 2006, have shown improvements in rest pain, wound healing, and digital ulcers in patients with Buerger's disease treated with this approach. It remains experimental and is not universally available, but the results are encouraging for patients who have failed conventional therapy.
Gene therapy targeting vascular endothelial growth factor (VEGF) — a protein that promotes the growth of new blood vessels — has been studied in Buerger's disease. Intramuscular injection of a gene vector encoding VEGF stimulates local angiogenesis and has shown improvement in rest pain and perfusion in early trials. This approach remains investigational and is only available at specialized research centers.
Omentoplasty is a surgical procedure in which the omentum — a richly vascularized fold of abdominal tissue — is mobilized and wrapped around the ischemic limb. The omentum brings its blood supply with it and promotes neovascularization of the ischemic tissue over time. It is used at some centers in Asia and Europe for severe cases where other therapies have failed and the alternative is major amputation.
Bosentan, an endothelin receptor antagonist used primarily for pulmonary hypertension and systemic sclerosis, has been studied in small series of Buerger's disease patients with digital ulcers. Some reports have shown reduction in ulcer number and improved digital blood flow, but the evidence base is limited.
Amputation remains a last resort. Minor amputations — removing a single gangrenous toe or fingertip — are performed to control necrotic tissue, prevent spreading infection, and allow wound healing with limb preservation. The goal is always the most conservative amputation that achieves adequate wound control. Major limb amputations — below-knee, above-knee, below-elbow — become necessary when gangrene has spread extensively or when uncontrolled infection threatens the patient's life. The rate of major amputation is directly related to tobacco cessation: patients who stop completely have a low rate; those who continue smoking face progressive and repeated amputations.
Prognosis and Amputation Risk
The prognosis in Buerger's disease is almost entirely determined by whether the patient achieves complete and sustained tobacco cessation. This creates an unusual situation in medicine where the doctor can deliver a clear, unambiguous message: stop all tobacco permanently and the disease will very likely stop with it. Continue, and progressive amputation is likely.
Patients who achieve complete and sustained cessation have an excellent prognosis for limb salvage. The disease arrests, existing ulcers heal with wound care, and the vast majority do not progress to major amputation. Existing vessel occlusions do not reverse — the closed vessels remain closed — but the disease stops creating new occlusions, and the body's collateral circulation often provides enough blood flow to maintain limb viability once the inflammatory process is no longer active.
Patients who continue to smoke face a dismal trajectory. Long-term follow-up studies, including the landmark series by Cooper and colleagues published in the Journal of the American College of Cardiology in 2004, have documented major amputation rates of 40 to 45 percent over 8 years in patients who continue tobacco use. This means nearly half of all patients who keep smoking will lose a foot, a leg, a hand, or an arm within 8 years. Serial minor amputations are even more common — a toe, then the forefoot, then the ankle — as ischemia extends progressively proximally in the absence of cessation.
One important and somewhat reassuring feature of Buerger's disease is that it affects the distal small vessels and does not involve the coronary arteries or the carotid and cerebral vessels. Unlike atherosclerotic peripheral artery disease, where patients are also at high risk for heart attack and stroke, patients with Buerger's disease do not have elevated risk of myocardial infarction or stroke from the disease itself. The mortality directly attributable to Buerger's disease is low. The disabling consequences — amputation, loss of functional limbs, chronic pain — are the primary burden of the disease. This makes the decision to stop smoking even more straightforward: the patient is trading amputation risk for limb preservation, not simply exchanging one set of symptoms for another.
Psychosocial support and addiction medicine involvement are essential. Tobacco use disorder is a genuine addiction with neurobiological underpinnings, and telling a patient to simply stop is rarely sufficient. Comprehensive cessation support — behavioral therapy, pharmacotherapy with varenicline or bupropion where appropriate, and follow-up — dramatically improves cessation rates and must be integrated into the care plan for every Buerger's patient.
Research Papers
- Olin JW. Thromboangiitis obliterans (Buerger's disease). N Engl J Med. 2000;343(12):864–869. PMID: 10995867
- Piazza G, Creager MA. Thromboangiitis obliterans. Circulation. 2010;121(14):1858–1861. — Search PubMed
- Fazeli B, Ravari H. Definition of Buerger's disease for a new millennium: an ongoing dilemma. Curr Atheroscler Rep. 2011;13(3):237–242. — Search PubMed
- Cooper LT, Tse TS, Mikhail MA, McBane RD, Stanson AW, Ballman KV. Long-term survival and amputation risk in thromboangiitis obliterans (Buerger's disease). J Am Coll Cardiol. 2004;44(12):2410–2411. — Search PubMed
- Cacione DG, Macedo CR, do Carmo Novaes F, Baptista-Silva JC. Pharmacological treatment for Buerger's disease. Cochrane Database Syst Rev. 2020;5(5):CD011033. — Search PubMed
- De Haro J, Acin F, Bleda S, Varela C, Esparza L. Treatment of thromboangiitis obliterans (Buerger's disease) with bosentan. BMC Cardiovasc Disord. 2012;12:5. — Search PubMed
- Fiessinger JN, Schafer M. Trial of iloprost versus aspirin treatment for critical limb ischaemia of thromboangiitis obliterans. The TAO Study. Lancet. 1990;335(8689):555–557. — Search PubMed
- Durdu S, Akar AR, Arat M, Sancak T, Eren NT, Unal EU, et al. Autologous bone-marrow mononuclear cell implantation for patients with Rutherford grade II-III thromboangiitis obliterans. J Vasc Surg. 2006;44(4):732–739. — Search PubMed
- Buerger L. Thrombo-angiitis obliterans: a study of the vascular lesions leading to presenile spontaneous gangrene. Am J Med Sci. 1908;136:567–580. (Historical reference PubMed search)
- Graziani L, Morelli L, Parini F, et al. Clinical outcome after extended endovascular recanalization in Buerger's disease in 20 consecutive cases. Ann Vasc Surg. 2012;26(3):387–395. — Search PubMed
- Brodmann M, Hafner F, Gary T, et al. Iloprost and spinal cord stimulation in a patient with Buerger's disease and digital necrosis. Vasc Endovascular Surg. 2010;44(8):690–691. — Search PubMed
- Mohler ER 3rd, Jaeger MC, Moore KA, et al. The treatment of peripheral arterial diseases: a review. J Am Coll Cardiol. 2001;37(4 Suppl B):89S–94S. (PubMed search)
Connections
- Cardiology
- Raynaud's Phenomenon
- Peripheral Artery Disease
- Atherosclerosis
- Varicose Veins
- Cardiovascular Disease
- Coronary Artery Disease
- Carotid Artery Stenosis
- Rheumatoid Arthritis