Mitral Stenosis
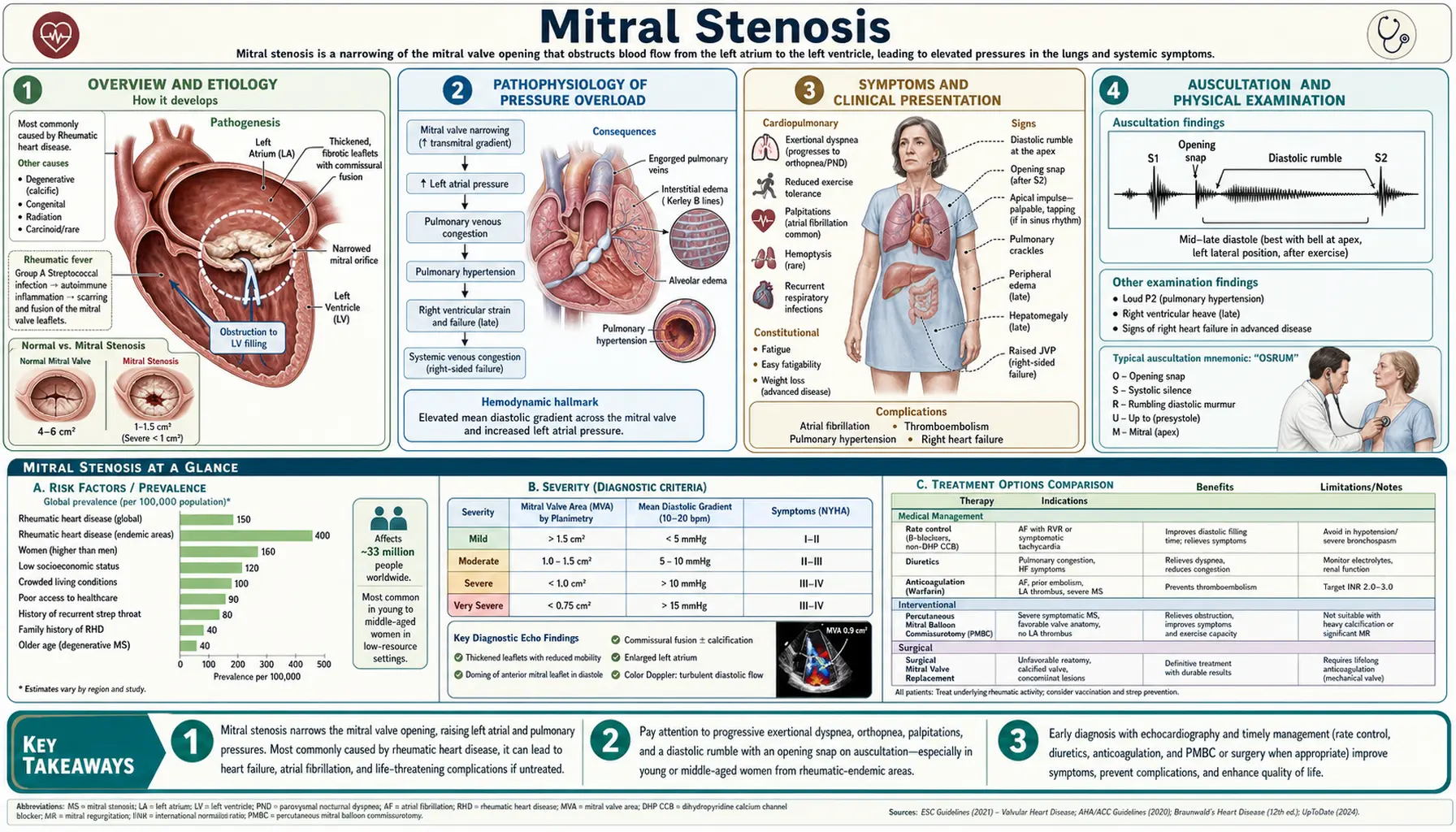
Table of Contents
- Overview and Etiology
- Pathophysiology of Pressure Overload
- Symptoms and Clinical Presentation
- Auscultation and Physical Examination
- Diagnosis: ECG, Echocardiography, and Scoring
- Medical Treatment
- Percutaneous Mitral Balloon Commissurotomy (PMBC)
- Surgical Treatment
- Prognosis
- Research Papers
- Connections
- Featured Videos
1. Overview and Etiology
Mitral stenosis (MS) is a mechanical obstruction of left ventricular inflow caused by narrowing of the mitral valve orifice. The normal mitral valve area (MVA) is 4–6 cm². Symptoms typically begin when MVA falls below 2 cm², hemodynamically significant stenosis is defined as MVA <1.5 cm², and severe stenosis as MVA <1.0 cm². The disease was once the most common valvular lesion in the developed world; declining rates of rheumatic fever have substantially reduced its prevalence in high-income countries, though it remains a leading cause of valvular morbidity globally.
Rheumatic Mitral Stenosis
Rheumatic fever — triggered by group A streptococcal (GAS) pharyngitis — causes an autoimmune valvulitis that damages mitral leaflets over years. The immune response to streptococcal M-protein cross-reacts with valve glycoproteins (molecular mimicry), producing recurrent episodes of leaflet inflammation and scarring. The pathological sequence is:
- Leaflet thickening and fibrosis: Recurrent inflammation deposits fibrous tissue along the leaflet surfaces. The tips of the leaflets fuse at the commissures (commissural fusion), converting the normal elliptical orifice into a narrow, funnel-shaped opening.
- Chordae tendineae involvement: The subvalvular apparatus thickens, shortens, and fuses — subvalvular fusion further restricts leaflet motion and compounds the mechanical obstruction.
- Calcification: In long-standing disease, the leaflets and commissures calcify, rendering them rigid and immobile. Heavily calcified valves are less amenable to balloon commissurotomy and usually require surgical replacement.
The latent period between the acute rheumatic episode and the onset of symptomatic MS is typically 20–40 years, explaining why MS classically presents in the third to fifth decade of life. Recurrent streptococcal infections accelerate progression; secondary prophylaxis with penicillin is critical in endemic regions.
Degenerative (Calcific) Mitral Stenosis
In elderly populations in developed countries, mitral annular calcification (MAC) extending into the leaflet bases can produce functionally significant stenosis. Unlike rheumatic MS, calcific MS does not involve commissural fusion — calcium deposits thicken the annulus and base of the leaflets, restricting the annular area without fusing the commissure tips. This distinction is critical: the absence of commissural fusion means that balloon commissurotomy is ineffective and potentially dangerous (it cannot split non-fused commissures, and aggressive balloon inflation risks leaflet laceration). The condition progresses slowly and is often managed medically until symptomatic, then surgically.
Congenital Mitral Stenosis
Congenital MS is rare, most commonly caused by parachute mitral valve — a malformation in which all chordae tendineae insert into a single papillary muscle (instead of the normal two), creating a funnel-shaped subvalvular obstruction. It is often part of Shone's complex (multiple left-sided obstructive lesions including supravalvular mitral ring, aortic coarctation, and subaortic stenosis). Congenital MS typically presents in infancy or childhood and requires surgical repair or replacement.
2. Pathophysiology of Pressure Overload
The fundamental hemodynamic consequence of mitral stenosis is obstruction of blood flow from the left atrium (LA) into the left ventricle (LV) during diastole. This creates a pressure gradient across the mitral valve — the transmitral gradient — that drives an escalating series of upstream pressure elevations with progressively severe downstream consequences.
Left Atrial Hypertension
As the mitral valve area narrows, the LA must generate increasing pressure to push blood across the obstructed orifice. Left atrial pressure (LAP) rises above the normal 5–12 mmHg, often reaching 20–30 mmHg in moderate MS and exceeding 35–40 mmHg in severe MS during exertion. Elevated LAP is transmitted backward through the pulmonary veins — the pulmonary venous system has no valves — causing pulmonary venous hypertension.
Pulmonary Congestion and Edema
When pulmonary venous pressure exceeds the plasma oncotic pressure (approximately 25 mmHg), fluid is forced across the pulmonary capillary membrane into the alveolar interstitium, producing pulmonary edema. The cardinal symptom is dyspnea — initially exertional, then at rest in advanced disease. Because heart rate is the key determinant of diastolic filling time, any physiological or pathological tachycardia — exercise, fever, anemia, atrial fibrillation — dramatically shortens diastole, reduces transmitral flow, and acutely raises LAP, precipitating acute decompensation.
Reactive Pulmonary Arterial Hypertension
Chronic pulmonary venous hypertension triggers a reactive rise in pulmonary arteriolar resistance through three mechanisms: (1) passive backward transmission of elevated venous pressure, (2) hypoxic vasoconstriction, and (3) structural remodeling (medial hypertrophy and intimal proliferation in pulmonary arterioles). Pulmonary arterial hypertension (PAH) in severe MS can reach systemic levels. PAH substantially increases right ventricular afterload.
Right Heart Failure
Sustained pressure overload from PAH causes right ventricular (RV) hypertrophy, followed by RV dilatation and failure. RV failure produces: tricuspid regurgitation (from annular dilatation), elevated right atrial and central venous pressure, jugular venous distension, hepatomegaly, ascites, and peripheral edema — the classic signs of right heart failure. In the late stages of MS, the left-sided obstruction that caused the entire cascade paradoxically produces a low-output state (reduced LV filling reduces cardiac output) combined with right heart failure — a hemodynamically devastating combination.
Left Atrial Dilatation, Atrial Fibrillation, and Thromboembolism
Chronically elevated LAP distends and remodels the left atrium. LA dilatation is almost universal in significant MS and leads to two critical complications:
- Atrial fibrillation (AF): LA dilatation disrupts atrial electrical conduction and promotes reentry circuits, causing AF in 30–40% of patients with significant MS. AF is doubly harmful: the loss of atrial contractile function reduces LV filling by an additional 20–30%, and the rapid ventricular rate during AF — by shortening diastole — acutely increases the transmitral gradient. AF is the most common precipitant of acute hemodynamic decompensation in MS patients.
- Left atrial thrombus: Blood stasis in the dilated LA — particularly in the left atrial appendage (LAA), where flow is lowest — promotes thrombus formation. LAA thrombus is the source of systemic arterial embolism in MS, with an annual embolic event rate of 1–5% in patients with AF and MS. Cerebral embolism (stroke) is the most feared consequence, accounting for significant long-term morbidity and mortality.
3. Symptoms and Clinical Presentation
The natural history of mitral stenosis is a prolonged asymptomatic latent period (reflecting the slow progression of rheumatic scarring over decades), followed by gradually increasing symptoms once the valve area falls below approximately 2 cm². Once significant dyspnea develops, the clinical course accelerates — average survival without intervention is 2–5 years from the onset of severe symptoms in untreated patients, and as low as 3 months once pulmonary hypertension is established.
Dyspnea
Dyspnea is the dominant and earliest symptom, initially occurring only with vigorous exertion — climbing stairs, lifting, sexual activity. As stenosis progresses, dyspnea occurs with lesser effort, and eventually with activities of daily living. The mechanism is straightforward: exertion raises heart rate, which shortens diastolic filling time and raises the transmitral gradient, acutely elevating LAP and causing pulmonary venous congestion. Any condition that increases heart rate — fever, infection, anemia, pregnancy, hyperthyroidism, atrial fibrillation — can similarly unmask or worsen symptoms.
Orthopnea and Paroxysmal Nocturnal Dyspnea
Orthopnea (dyspnea worsened by lying flat) and paroxysmal nocturnal dyspnea (sudden awakening with breathlessness) reflect redistribution of venous blood into the pulmonary circulation when recumbent. These symptoms indicate significant pulmonary venous hypertension and signal a more advanced stage of disease.
Hemoptysis
Hemoptysis — coughing blood — occurs in two distinct forms: (1) frank hemoptysis from rupture of dilated bronchial veins engorged by pulmonary venous hypertension (a relatively rare but dramatic presentation); and (2) pink frothy sputum from acute pulmonary edema, where alveolar fluid mixes with blood from ruptured alveolar capillaries. Hemoptysis in a patient with rheumatic heart disease should strongly suggest significant MS.
Atrial Fibrillation and Palpitations
Palpitations from atrial fibrillation are often the first symptom that prompts patients to seek medical care. The onset of AF in a patient with MS is frequently accompanied by acute hemodynamic deterioration — patients experience sudden breathlessness and sometimes collapse, reflecting the abrupt loss of atrial contraction and the rapid ventricular rate. Stroke may be the presenting event in patients with undiagnosed MS and AF.
Fatigue and Reduced Exercise Tolerance
Reduced cardiac output — from limited LV filling — manifests as easy fatigability and decreased exercise capacity. As disease advances, a fixed low cardiac output state predominates: patients have cool extremities, reduced urine output, and poor effort tolerance despite the absence of dramatic pulmonary congestion.
Symptoms of Right Heart Failure
In advanced MS with established pulmonary hypertension, right heart failure produces ankle swelling, abdominal distension from ascites, right upper quadrant discomfort from hepatic congestion, and anorexia. At this stage the prognosis is poor without intervention.
4. Auscultation and Physical Examination
The auscultatory findings of mitral stenosis are among the most classic in clinical cardiology. They require careful technique: the patient must be examined in the left lateral decubitus position, using the bell of the stethoscope applied lightly at the cardiac apex. Low-pitched diastolic sounds are best heard with the bell (which emphasizes low frequencies) rather than the diaphragm.
Loud First Heart Sound (S1)
In rheumatic MS with pliable, non-calcified leaflets, the mitral valve closure sound (S1) is characteristically loud. The leaflets remain widely open throughout diastole due to elevated LA-to-LV pressure gradient, and close with great velocity when the LV begins to contract — producing an accentuated S1. As the valve calcifies and leaflet mobility decreases, S1 softens. A soft S1 in MS therefore implies advanced calcification and reduced candidacy for balloon commissurotomy.
Opening Snap (OS)
The opening snap is a high-pitched extra sound immediately following A2 (aortic component of the second heart sound), caused by the abrupt deceleration of the mitral leaflets as they open rapidly under the elevated LA pressure and then are suddenly arrested by the fused, thickened chordae and leaflet tips. The timing of the OS after A2 — the A2-OS interval — inversely correlates with stenosis severity:
- Mild MS (higher LA pressure): longer A2-OS interval (70–110 ms) — the valve opens later relative to A2 because a longer LV relaxation time is needed to equalize pressures.
- Severe MS (markedly elevated LAP): shorter A2-OS interval (<60–70 ms) — the persistently high LAP forces the valve open almost immediately after aortic valve closure.
The OS is heard best at the lower left sternal border and radiates to the apex. As valve calcification progresses, the OS disappears — the stiffened leaflets no longer snap open.
Low-Pitched Mid-Diastolic Rumble
The pathognomonic murmur of MS is a low-pitched, rumbling mid-diastolic murmur heard best at the cardiac apex in the left lateral decubitus position with the bell of the stethoscope. It begins immediately after the opening snap and decrescendos through mid-diastole, then — in patients in sinus rhythm — intensifies again in late diastole due to atrial contraction (presystolic accentuation). This presystolic component disappears in atrial fibrillation (no atrial contraction). The murmur is accentuated by maneuvers that increase cardiac output and transmitral flow — exercise, turning to the left lateral position — making it important to auscultate the patient immediately after mild exertion when the murmur is subtle.
Additional Findings
- Malar flush (mitral facies): Bilateral pinkish-purple discoloration of the cheeks, caused by chronic low cardiac output and cutaneous vasodilation — a classic but now rarely seen sign of advanced MS.
- Signs of pulmonary hypertension: Loud P2, right ventricular heave (parasternal lift), palpable P2, and — in right heart failure — signs of tricuspid regurgitation (pansystolic murmur at the lower left sternal border that increases with inspiration).
- Jugular venous distension, hepatomegaly, peripheral edema: In advanced disease with right heart failure.
5. Diagnosis: ECG, Echocardiography, and Scoring
The diagnosis of mitral stenosis rests on echocardiography, which provides both anatomical characterization and hemodynamic quantification. The electrocardiogram and chest radiograph provide supporting evidence and assess downstream consequences.
Electrocardiography
ECG findings in MS are indirect markers of LA and RV remodeling:
- P-mitrale: In sinus rhythm, LA enlargement produces a broad, notched P wave (>0.12 seconds) in leads I and II, with a biphasic P wave in V1 (prominent negative terminal deflection). This pattern is called P-mitrale and is the ECG signature of significant LA dilatation.
- Atrial fibrillation: Replaces P waves with irregular fibrillatory baseline; irregular RR intervals. Present in 30–40% of patients with significant MS.
- Right axis deviation and right ventricular hypertrophy (RVH): In established pulmonary hypertension — dominant R in V1, deep S in V5–V6, right axis deviation.
Chest Radiography
Classic chest X-ray findings include: straightening of the left heart border (LA appendage enlargement), double density at the right heart border (LA body enlargement visible through the right atrium), elevation of the left mainstem bronchus (from LA enlargement pushing it upward), and Kerley B lines (short horizontal lines at the lung bases, representing fluid in interlobular septa). In advanced disease: upper lobe pulmonary venous dilatation, pulmonary edema, and right heart enlargement.
Echocardiography — Anatomical Assessment
Transthoracic echocardiography (TTE) is the first-line diagnostic modality. Key anatomical findings in rheumatic MS include: leaflet thickening, restricted opening (characteristic "hockey stick" appearance of the anterior mitral leaflet on parasternal long-axis view as the tip bows toward the LV while the base remains tethered), commissural fusion, subvalvular thickening and fusion, and calcification. The degree of calcification and subvalvular disease is critical for procedural planning.
Echocardiography — Hemodynamic Quantification
Doppler echocardiography quantifies stenosis severity through two primary methods:
- Pressure half-time (PHT) method: The time required for the transmitral gradient to fall to half its peak value. PHT reflects the rate at which the LA-to-LV pressure gradient equalizes — the slower the equalization (longer PHT), the more obstructed the valve. PHT ≥220 ms correlates with severe stenosis (MVA <1.0 cm²). MVA is estimated as: MVA = 220 / PHT. Limitations: PHT is unreliable when LA compliance is abnormal (e.g., after commissurotomy), in significant aortic regurgitation, or in elevated LV end-diastolic pressure.
- Planimetry: Direct measurement of the MVA by tracing the valve orifice on a parasternal short-axis 2D image. Considered the most accurate method but requires optimal imaging quality and technical expertise.
- Mean transmitral gradient: Measured by continuous-wave Doppler. A mean gradient >10 mmHg at rest indicates severe stenosis; even a gradient of 5–10 mmHg may be functionally significant during exertion.
Wilkins Echocardiographic Score
The Wilkins score grades four anatomical variables on a 1–4 scale each (total score 4–16), predicting the suitability and likely outcome of percutaneous mitral balloon commissurotomy (PMBC):
- Leaflet mobility: 1 = highly mobile, only tip restriction; 4 = minimal or no leaflet movement in diastole.
- Leaflet thickening: 1 = near-normal (4–5 mm); 4 = marked thickening of all leaflet tissue (>8–10 mm).
- Subvalvular thickening: 1 = minimal just below leaflets; 4 = extensive thickening and shortening of chordae extending into the papillary muscles.
- Calcification: 1 = single area of increased echogenicity; 4 = extensive calcification across both leaflets.
A Wilkins score ≤8 predicts a favorable response to PMBC (post-procedure MVA typically >1.5 cm²) with low procedural complication rates. Scores >8 — especially when driven by calcification or severe subvalvular disease — indicate poor PMBC candidacy and favor surgical referral. Commissural calcification (calcium specifically at the commissures) carries particularly poor PMBC outcomes and is a relative contraindication even with an otherwise favorable total Wilkins score.
6. Medical Treatment
Medical therapy in mitral stenosis does not alter the structural abnormality or reverse the obstruction. Its goals are to control symptoms, reduce heart rate, prevent thromboembolic complications, and manage secondary consequences such as atrial fibrillation and pulmonary hypertension. Definitive therapy — balloon commissurotomy or surgery — remains the only intervention that reliably improves hemodynamics and long-term outcomes.
Rate Control in Atrial Fibrillation
Heart rate control is the single most impactful medical intervention in MS patients with AF. Slowing the ventricular rate prolongs diastolic filling time, reduces the transmitral pressure gradient, and lowers LAP — translating directly into symptom relief. Target resting heart rate is 60–80 bpm; during exercise, rate should remain below 100–110 bpm. First-line agents:
- Beta-blockers (metoprolol, bisoprolol, atenolol): most commonly used; effective at rest and during exertion; well tolerated in most patients. Avoid in significant decompensated heart failure and reactive airway disease.
- Non-dihydropyridine calcium channel blockers (diltiazem, verapamil): effective alternatives when beta-blockers are contraindicated.
- Digoxin: Less effective for rate control during exertion; primarily useful as adjunctive therapy in patients with concurrent systolic dysfunction or when other agents are contraindicated.
Anticoagulation
Anticoagulation is mandatory in rheumatic MS with any of the following: current AF (paroxysmal, persistent, or permanent), prior thromboembolism, or documented left atrial thrombus. The annual stroke risk in rheumatic MS with AF is approximately 3–8%, making anticoagulation a high-benefit intervention. Key considerations:
- Vitamin K antagonists (warfarin): The recommended anticoagulant for rheumatic MS with AF. Target INR is 2.0–3.0. The 2021 ESC and 2020 AHA/ACC guidelines state that direct oral anticoagulants (DOACs) are not approved for rheumatic MS — the INVICTUS trial (2022) demonstrated that rivaroxaban was significantly inferior to warfarin for rheumatic MS with AF (higher combined rate of stroke, systemic embolism, MI, and death), confirming that DOACs should not be substituted for warfarin in this specific population.
- LA thrombus: If detected on TEE, anticoagulation should be maintained for at least 3 months (or until thrombus resolution is confirmed) before any planned intervention.
- Even patients in sinus rhythm with significant MS and markedly enlarged LA (>55 mm) are sometimes anticoagulated given stroke risk, though evidence is less clear-cut; this decision is individualized.
Diuretics
Loop diuretics (furosemide) reduce pulmonary venous congestion and alleviate symptoms of dyspnea and orthopnea by lowering circulating blood volume and LA filling pressure. They provide symptom relief but do not slow disease progression. Use the minimum effective dose to avoid volume depletion, which can reduce cardiac output and cause prerenal azotemia.
Rheumatic Fever Prophylaxis
In patients from endemic regions who have documented rheumatic fever history, long-term secondary prophylaxis with penicillin (benzathine penicillin G 1.2 million units IM every 3–4 weeks) prevents recurrent streptococcal pharyngitis, thereby slowing the progression of rheumatic valve disease. Prophylaxis is recommended for at least 10 years after the last documented episode of rheumatic fever, or until age 40 (whichever is longer), per WHO guidelines.
7. Percutaneous Mitral Balloon Commissurotomy (PMBC)
Percutaneous mitral balloon commissurotomy — also called percutaneous mitral balloon valvuloplasty (PMBV) or percutaneous transvenous mitral commissurotomy (PTMC) — is the procedure of choice for symptomatic patients with significant MS who have favorable valve anatomy. It is equivalent in efficacy to surgical closed commissurotomy and approaches the outcomes of open commissurotomy in carefully selected patients, without the risks of open-heart surgery.
Mechanism
PMBC is performed under fluoroscopic and echocardiographic guidance via femoral venous access. The procedure involves:
- Transseptal puncture: a needle is passed through the interatrial septum from the right atrium into the LA under fluoroscopic guidance.
- A guidewire is advanced across the stenotic mitral valve into the LV.
- An Inoue balloon catheter (or double-balloon technique) is positioned across the mitral orifice with the distal half in the LV and the proximal half in the LA.
- Rapid balloon inflation splits the fused commissures, enlarging the valve area. Success depends on the fused commissures separating cleanly — which requires pliable, non-calcified tissue at the commissures specifically.
A successful PMBC doubles MVA on average (from ~1.0 to ~2.0 cm²) and reduces mean transmitral gradient by 50–60%. The improvement in LAP translates into immediate symptom relief.
Patient Selection
Ideal candidates for PMBC are:
- Symptomatic MS (NYHA Class II–IV) with MVA <1.5 cm²
- Wilkins score ≤8
- No significant mitral regurgitation (>grade 2+ MR is a contraindication — balloon inflation risks worsening MR)
- No LA thrombus on TEE (anticoagulate and repeat imaging)
- Favorable commissural anatomy (non-calcified commissures)
PMBC is also appropriate for asymptomatic patients with very severe MS (MVA <1.0 cm²) and favorable anatomy, or for patients with significant MS who cannot tolerate surgery.
Outcomes
In experienced centers with optimal patient selection, PMBC achieves a procedural success rate (MVA >1.5 cm² without significant MR) of 80–95%. Event-free survival (freedom from death, repeat intervention, or NYHA Class III–IV) at 10 years is 50–70% in favorable anatomy groups. Long-term outcomes are determined primarily by restenosis — valve area progressively narrows again as scarring recurs, with approximately 40–50% of patients requiring repeat intervention within 10 years. Repeat PMBC is feasible if restenosis occurs without significant calcification or MR. The landmark Iung et al. long-term registry data demonstrated that PMBC provides excellent 15-year outcomes in patients with optimal anatomy.
Complications
- Severe mitral regurgitation: The most important procedural complication, occurring in 2–10% of cases. Results from leaflet tear rather than commissural splitting, typically in calcified or fibrosed leaflets. Severe procedural MR requires emergency surgical valve replacement.
- Systemic embolism: Risk of LA thrombus dislodgement; minimized by TEE screening and anticoagulation before the procedure.
- Atrial septal defect: The transseptal puncture leaves a small iatrogenic ASD; the vast majority close spontaneously within 6 months.
- Cardiac tamponade: From transseptal puncture or perforation; rare (<1%) in experienced hands.
- Procedural mortality: <1% at experienced centers.
8. Surgical Treatment
Surgical intervention for mitral stenosis is indicated when PMBC is contraindicated by unfavorable anatomy (high Wilkins score, commissural calcification, significant MR, LA thrombus unresolved by anticoagulation) or when commissurotomy has failed or restenosed in a patient with anatomy unsuitable for repeat balloon procedure.
Closed Mitral Commissurotomy
Closed commissurotomy — performed without cardiopulmonary bypass, splitting the commissures manually or with a mechanical dilator through a purse-string incision in the LV apex — was the historical surgical approach and remains widely used in developing countries where rheumatic MS is prevalent and cardiopulmonary bypass resources are limited. In experienced hands it yields results comparable to PMBC for favorable anatomy, but carries the disadvantage that direct valve inspection and subvalvular repair under cardiopulmonary bypass are not possible.
Open Mitral Commissurotomy
Open commissurotomy on cardiopulmonary bypass allows direct visualization of the valve, precise separation of fused commissures, debridement of calcium, and repair of subvalvular fusion. It is preferred over the closed technique when available. Open commissurotomy preserves the native valve, avoiding the long-term complications of prosthetic valves, and yields favorable results in patients with pliable leaflets and manageable subvalvular disease. MVA after open commissurotomy exceeds that achieved by PMBC in heavily involved subvalvular apparatus cases.
Mitral Valve Replacement (MVR)
MVR is necessary when valve anatomy is too distorted by calcification, thickening, or subvalvular fusion to permit successful commissurotomy or repair. Choice of prosthesis:
- Mechanical prostheses (St. Jude Medical bileaflet, tilting-disc valves): durable (decades), but require lifelong anticoagulation with warfarin. Preferred in younger patients (<60–65 years) who have no contraindication to anticoagulation.
- Bioprosthetic (tissue) valves (porcine, bovine pericardial): do not require long-term anticoagulation beyond 3 months post-implant, but degenerate over time (mean durability 10–15 years in the mitral position). Preferred in elderly patients (>65–70 years), patients with anticoagulation contraindications, and women of childbearing age who desire pregnancy (though valve durability may be compromised by pregnancy-associated hemodynamic stress).
The subvalvular apparatus should be preserved during MVR whenever possible — removing the chordae abolishes their tethering function and impairs LV geometry and contractility, contributing to post-operative LV dysfunction.
Surgical Risk and Outcomes
Operative mortality for isolated MVR is approximately 3–8% in the current era. Risk increases with age, poor LV function, pulmonary hypertension severity, and comorbidities. Long-term survival after successful MVR is substantially better than the natural history of untreated severe MS, though prosthesis-related complications (valve thrombosis, endocarditis, structural deterioration, anticoagulation-related bleeding) require lifelong surveillance.
9. Prognosis
Untreated mitral stenosis follows a predictable trajectory shaped by the rate of progression and the hemodynamic consequences of each complication. With timely intervention — PMBC or surgical — outcomes are substantially improved, though the underlying rheumatic disease process continues and residual LA enlargement, AF, and pulmonary vascular remodeling may persist.
Natural History Without Intervention
Once symptoms develop, the prognosis of untreated MS is poor. In the historical pre-intervention era, 10-year survival after onset of symptoms was approximately 50–60% in patients with mild-to-moderate disability; however, once significant pulmonary hypertension or right heart failure supervened, 10-year survival fell to 0–15%. Mean survival after onset of severe symptoms was 2–5 years. Key prognostic milestones:
- Onset of AF: Marks acceleration of disease — associated with a 2–4-fold increased risk of embolism and hemodynamic deterioration.
- Systemic embolism: Stroke significantly increases mortality and long-term disability.
- Pulmonary hypertension: Severe PAH (mean PA pressure >55 mmHg) is associated with very poor prognosis without intervention.
Outcomes After PMBC
In patients with optimal anatomy (Wilkins ≤8, non-calcified commissures), PMBC yields 10-year event-free survival of 50–70%, with functional improvement sustained in most patients. Restenosis is the primary long-term challenge, occurring in approximately 40–50% at 10 years; repeat PMBC is feasible in approximately 30–40% of restenosis cases. Predictors of poor long-term PMBC outcome include higher Wilkins score, AF at baseline, and older age.
Outcomes After Surgery
Operative mortality for isolated MVR is 3–8%. Long-term survival after MVR is substantially better than the natural history but lower than age-matched controls, reflecting underlying cardiac remodeling, persistent AF, anticoagulation-related complications, and prosthesis-related events. Patients who undergo successful intervention before the development of severe pulmonary hypertension or right heart failure have the best long-term outcomes — emphasizing the importance of timely referral when MVA reaches 1.0–1.5 cm² and symptoms progress.
Pregnancy in Mitral Stenosis
Pregnancy imposes a 30–50% increase in cardiac output and heart rate — a combination that dramatically increases the transmitral gradient and LAP. Significant MS (MVA <1.5 cm²) is poorly tolerated in pregnancy and carries substantial maternal and fetal risk. Women with significant MS who wish to become pregnant should be referred for PMBC before conception if anatomy is suitable. During pregnancy, MS can decompensate rapidly in the second and third trimesters as blood volume and heart rate peak; beta-blockers are first-line for rate control; PMBC can be performed during pregnancy (with appropriate shielding) if medical management fails.
10. Research Papers
- Search PubMed
- Search PubMed
- Vahanian A et al. Guidelines on the management of valvular heart disease (version 2012). Eur Heart J. 2012;33(19):2451–2496.
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
Connections
- Cardiology
- Mitral Regurgitation
- Aortic Stenosis
- Aortic Regurgitation
- Infective Endocarditis
- Valvular Heart Disease
- Atrial Fibrillation
- Heart Failure
- All Conditions