Diagnosing Cholera: Rapid Tests, Stool Culture, and Field Diagnosis
- Clinical Diagnosis During Outbreaks
- Rapid Dipstick Immunochromatographic Test
- Darkfield Microscopy: Shooting Stars
- Stool Culture on TCBS Agar
- PCR for Serogroup and Biotype Typing
- Distinguishing Cholera from Other Watery Diarrheas
- When Lab Confirmation Is Needed vs. Just Treating
- Antibiotic Susceptibility Testing
- Key Research
- Connections
Clinical Diagnosis During Outbreaks
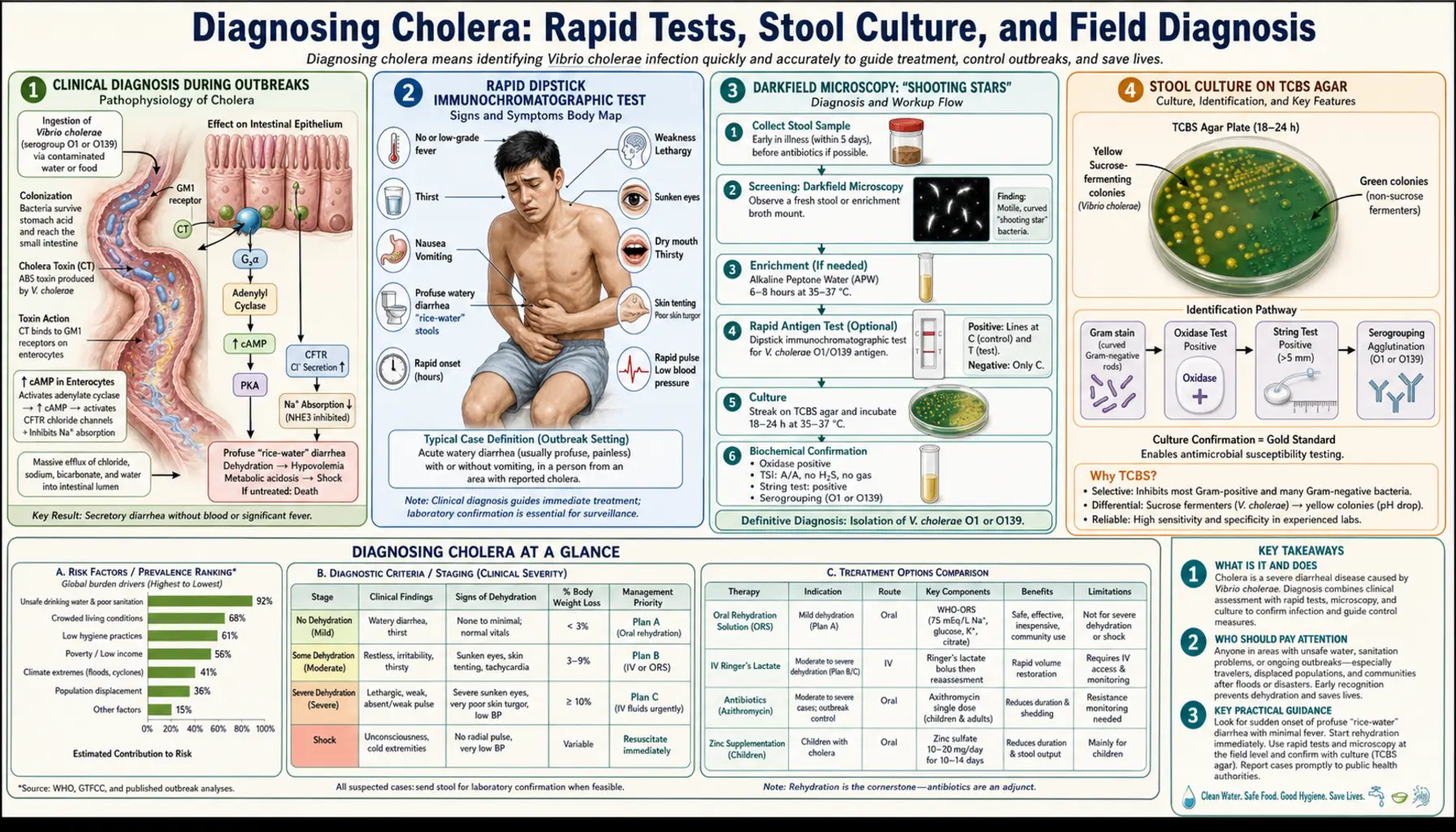
During a cholera outbreak, the most important diagnostic act is often a clinical one — recognizing the disease by its appearance and treating it immediately, without waiting for laboratory tests that may take hours to days. In cholera treatment settings, this is not a shortcut: it is the standard of care that saves lives.
The WHO defines a suspected cholera case as: any patient aged 2 years or older with acute watery diarrhea, with or without vomiting. In an area where cholera is known to be circulating, this definition is sufficient to begin treatment. The distinctive features that raise clinical suspicion include the rice-water appearance of stool, the extreme rapidity of fluid loss (producing the dehydration signs within hours), the absence of blood or visible pus in the stool (which would suggest a different bacterial cause), and the clinical alertness of even severely dehydrated patients.
The logic of treating without confirmation is straightforward: the treatment (oral rehydration salts) is safe, effective, cheap, and appropriate for any cause of severe watery diarrhea. Beginning ORS while waiting for test results costs nothing and saves the patient's life if cholera is the diagnosis. Waiting 24–48 hours for culture results while withholding rehydration is not appropriate medical practice in a cholera setting.
For health workers in endemic or outbreak areas, learning to recognize cholera on clinical grounds — the appearance, smell, speed of onset, and dehydration signs — is far more practically valuable than relying on any diagnostic test. Diagnostic tests matter for outbreak surveillance and antibiotic resistance monitoring, not for the individual treatment decision in most cases.
Rapid Dipstick Immunochromatographic Test
The most widely used point-of-care diagnostic tool for cholera is the Crystal VC rapid immunochromatographic test (manufactured by Span Diagnostics), which can detect V. cholerae O1 and O139 antigens directly in a stool sample within 15 minutes, with no laboratory equipment, electricity, or technical training beyond a brief orientation.
The Crystal VC test works by running liquid stool sample across a nitrocellulose strip coated with antibodies specific to the O1 and O139 antigens of V. cholerae. If the antigens are present, they bind to the antibodies and produce a visible colored line — similar in principle to a home pregnancy test. Two lines appear (one control, one test line) for a positive result; only the control line appears for negative.
Performance characteristics from field validation studies:
- Sensitivity: approximately 80–85% for O1 serogroup — meaning the test correctly identifies about 4 out of 5 true cholera cases, missing about 1 in 5
- Specificity: approximately 95% — meaning about 1 in 20 positive results is a false positive (not actually cholera)
- Result time: 15 minutes from sample application
- No cold chain required for storage (important in resource-limited field settings)
- Sensitivity is higher when samples are taken early in the illness (before antibiotic treatment) and when the bacterial load is high — which it typically is in severe cholera
The Crystal VC is primarily used not for individual treatment decisions (which are made clinically) but for outbreak investigation — determining whether a cluster of watery diarrhea cases in a new area is actually cholera, to trigger the appropriate public health response. A positive rapid test from a new area warrants immediate confirmation by culture, while outbreak response measures (water treatment, cholera kits, alert systems) begin simultaneously.
False negatives can occur because the test detects surface antigens but does not detect all strains equally. Variant El Tor strains with altered O-antigen expression may give weaker or negative results. Because of this, the WHO recommends that rapid test results should always be confirmed by stool culture when possible, particularly for the first cases in a suspected new outbreak.
Darkfield Microscopy: Shooting Stars
Before rapid tests existed, and still today in laboratories with the equipment, darkfield microscopy of fresh stool was one of the fastest ways to make a presumptive diagnosis of cholera — producing a result in minutes from a fresh stool sample.
Darkfield microscopy illuminates specimens from the side rather than from below, making objects against a dark background appear bright — like stars in a night sky. When a drop of fresh, undiluted rice-water stool from a cholera patient is examined under darkfield, the observer sees tiny, extremely rapidly moving curved rods shooting in all directions across the field of view. The characteristic darting, rapid, "shooting star" motility of V. cholerae — driven by its single polar flagellum — is quite distinctive from the motility patterns of most other gut bacteria.
The technique takes only a few minutes: collect fresh stool (ideally within 2 hours of passage, before bacteria begin to die), place a small drop on a glass slide, apply a cover slip, and examine under darkfield illumination at 400x magnification. Experienced microscopists can recognize the distinctive V. cholerae motility immediately.
The sensitivity of this technique depends heavily on the bacterial load in the sample (which is highest early in infection, before antibiotic treatment) and the experience of the microscopist. It is most useful in reference laboratories and research settings. Motility can be inhibited by adding antiserum specific to the O1 serogroup — if the shooting motion stops when O1 antiserum is added (immobilization test), it confirms O1 identity.
The technique has largely been superseded by rapid antigen tests in field settings, but remains a useful rapid tool in well-equipped laboratories and is sometimes used for teaching because the visual impression is so distinctive.
Stool Culture on TCBS Agar
The gold standard for laboratory confirmation of cholera is culture of stool (or rectal swab) on thiosulfate-citrate-bile-sucrose (TCBS) agar, a selective medium specifically designed to grow Vibrio species while inhibiting most gut flora. TCBS results take 18–24 hours of incubation, placing it in the "confirmation" rather than "rapid diagnosis" category.
On TCBS agar, V. cholerae O1 produces characteristic flat, yellow colonies (from sucrose fermentation) that appear after overnight incubation at 35–37°C. The yellow color distinguishes them from V. parahaemolyticus, which produces blue-green colonies on TCBS (it does not ferment sucrose), a useful internal control. The yellow colonies are then tested with polyvalent O1 antiserum using agglutination to confirm serogroup.
The full diagnostic process on TCBS involves:
- Inoculate the TCBS plate with stool or rectal swab; also inoculate an alkaline peptone water (APW) enrichment broth
- After 6–8 hours, subculture the APW broth to a second TCBS plate (enrichment increases yield from low-inoculum samples)
- Examine plates after 18–24 hours of incubation; pick suspicious yellow colonies
- Test picked colonies for O1 agglutination with polyvalent and monovalent (Ogawa/Inaba) antisera
- Confirm biochemical identity (oxidase positive, rapid fermentation of glucose)
- Send confirmed isolates to reference laboratory for biotyping (El Tor vs Classical) and toxigenic genotyping
Culture is essential for surveillance purposes — confirming the serogroup, biotype, and antibiotic susceptibility pattern of the circulating strain. This information guides treatment protocols across an outbreak and tracks the evolution of the pathogen over time. Individual patient outcomes, however, do not depend on culture results.
PCR for Serogroup and Biotype Typing
When reference laboratory capacity is available, polymerase chain reaction (PCR) testing provides rapid, highly sensitive, and highly specific identification of V. cholerae and its key characteristics — typically within 3 to 6 hours from sample to result.
PCR tests can simultaneously detect and differentiate:
- Species identity: genes specific to V. cholerae (e.g., the ompW gene, present in all V. cholerae)
- O1 serogroup: genes encoding O1 antigen biosynthesis (rfbO1)
- O139 serogroup: genes encoding O139 antigen biosynthesis (rfbO139)
- Toxigenic potential: genes encoding cholera toxin (ctxA) — this is crucial, because non-toxigenic V. cholerae O1 can exist that do not cause epidemic disease
- Biotype: El Tor vs Classical distinction based on genetic markers
- Variant El Tor strains: genes indicating altered cholera toxin expression (important for understanding pandemic potential)
PCR is particularly valuable for outbreak characterization — understanding the genetic profile of the circulating strain to track its origins and spread, inform vaccine decisions (since available vaccines are designed against O1 and O139 strains), and guide public health interventions. Whole-genome sequencing, now increasingly available through international reference networks like the Global Cholera Reference Center, takes this further — allowing researchers to reconstruct transmission chains and trace outbreaks back to their geographic source with high precision.
For clinical care at the point of treatment in most cholera-endemic countries, PCR is not routinely used — the infrastructure is not available in field settings. But samples from the first confirmed cases in each new outbreak are typically sent to national or international reference laboratories for PCR characterization as part of standard surveillance protocol.
Distinguishing Cholera from Other Watery Diarrheas
In a cholera outbreak setting, most watery diarrhea can be presumptively treated as cholera. But in areas without known outbreak activity, or in traveler medicine, distinguishing cholera from other causes of acute watery diarrhea is clinically relevant. The key differential diagnoses include:
Rotavirus and other viral gastroenteritis: Most common cause of acute watery diarrhea worldwide, especially in children. Distinguishing features: rotavirus typically causes vomiting prominently (often before diarrhea), low-grade fever is common, diarrhea is less profuse than cholera (rarely exceeding 250 mL/hour), and the stool may have a more yellow color. Rotavirus most commonly affects children under 5. Duration is typically 3–8 days. No antibiotic treatment is effective.
Enterotoxigenic E. coli (ETEC): The most common cause of traveler's diarrhea and a major cause of diarrheal death in children in low-income countries. ETEC produces toxins (LT and ST) that cause a watery diarrhea with similar mechanisms to cholera but typically less severe. Clinical distinction: ETEC diarrhea is rarely as profuse as cholera, dehydration is less extreme, and the clinical course is typically shorter (3–5 days). In outbreak settings, stool culture can distinguish ETEC from V. cholerae.
Cryptosporidiosis: Causes profuse watery diarrhea particularly in immunocompromised individuals (HIV, malnutrition, transplant patients). Stool examination shows oocysts on modified acid-fast staining. Antibiotic treatment (which helps cholera) is largely ineffective for cryptosporidium. Suspect cryptosporidium when cholera treatment is not improving the clinical picture.
Dysentery (bloody diarrhea): Shigella, Salmonella, Campylobacter, and E. coli O157 cause inflammatory diarrhea with blood and/or mucus in the stool, fever, and tenesmus (painful urge to defecate). Cholera is essentially never bloody. Blood in the stool in a cholera outbreak setting should prompt culture for these alternative pathogens, as the treatment differs significantly.
When Lab Confirmation Is Needed vs. Just Treating
The decision to pursue laboratory confirmation versus simply treating follows a practical public health logic:
When clinical treatment takes priority and confirmation can wait:
- Known outbreak area with confirmed cholera circulation in the community or district
- Patient presents with rice-water diarrhea and signs of dehydration — treat immediately with ORS/IV fluids
- Resource-limited setting where laboratory capacity is unavailable or results would take more than 24 hours
- Patient is deteriorating rapidly — waiting for any test is not acceptable
When laboratory confirmation is essential:
- First cases in a new area: Before declaring a cholera outbreak, laboratory confirmation of the first 5–10 cases is essential. This prevents misclassification of ETEC or rotavirus clusters as cholera, which has happened and led to inappropriate outbreak responses
- Outbreak that is not responding to standard treatment: May indicate a resistant strain or a co-circulating pathogen requiring different treatment
- Surveillance: Continuous sampling throughout outbreaks tracks strain evolution and antibiotic resistance trends — essential for guiding treatment decisions for all subsequent patients
- Sporadic case in a non-endemic country: A traveler returning from a cholera-endemic country with watery diarrhea should have stool culture performed even if treated empirically, both to confirm diagnosis and to ensure public health notification is accurate
Antibiotic Susceptibility Testing
Knowing the antibiotic susceptibility pattern of the V. cholerae strain circulating in a given outbreak is not needed for individual patient treatment decisions — the first-line antibiotics are given empirically — but it is critically important for guiding outbreak-wide treatment policy.
Susceptibility testing is performed on isolates recovered from stool culture, typically using disk diffusion (Kirby-Bauer) or broth microdilution methods, following CLSI or EUCAST guidelines. The key antibiotics tested include:
- Azithromycin: Currently the preferred first-line antibiotic for most cholera outbreaks globally; resistance is still uncommon but has been reported
- Doxycycline: Traditional first-line agent for adults; widespread tetracycline resistance developed in the 1990s in Bangladesh and spread globally — many current strains are tetracycline-resistant
- Ciprofloxacin: Second-line option; fluoroquinolone resistance has been documented in South Asian strains since the early 2000s and is increasing
- Trimethoprim-sulfamethoxazole (TMP-SMX): Resistance is widespread in many settings
- Ampicillin: Also widely resistant
Antibiotic resistance in V. cholerae is often plasmid-mediated, meaning resistance genes can transfer between strains and even between bacterial species in the gut. Multi-drug resistant (MDR) strains carrying resistance to ampicillin, trimethoprim, tetracycline, and streptomycin on a single integrating conjugative element (ICE) have been documented since the 1980s and continue to spread. This is why surveillance-level susceptibility testing — culturing and testing isolates throughout an outbreak — is a public health necessity, not a laboratory luxury.
When an outbreak reveals a strain resistant to the standard first-line antibiotic, national health authorities update their treatment guidelines for that outbreak. Switching antibiotic classes for tens of thousands of patients based on laboratory data from the first few hundred isolates is one of the most impactful uses of diagnostic information in outbreak medicine.
Key Research
- Garg P, et al. "Molecular epidemiology of Vibrio cholerae O139 cholera in India and Bangladesh." J Clin Microbiol. 2003;41(6):2489–2496 — Search PubMed
- Nato F, et al. "One-step immunochromatographic dipstick tests for rapid detection of Vibrio cholerae O1 and O139 in stool samples." Clin Diagn Lab Immunol. 2003;10(3):476–478 — Search PubMed
- Mukhopadhyay AK, et al. "A novel genetically altered V. cholerae O1 biotype El Tor with classical CT phage." Emerg Infect Dis. 1996;2(3):266 — Search PubMed
- Cholera Working Group. "Use of thiosulphate citrate bile sucrose agar for the isolation of Vibrio species." J Clin Pathol. 1970;23(3):218–219 — Search PubMed
- WHO. "Laboratory methods for the diagnosis of Vibrio cholerae." Geneva: World Health Organization; 1992. (Foundational WHO laboratory manual)
- Alam M, et al. "Diagnostic limitation of a commercial rapid test in determining the cause of cholera." J Clin Microbiol. 2010;48(5):1862–1866 — Search PubMed
- Weill FX, et al. "Multidrug resistance in Vibrio cholerae." Antimicrob Agents Chemother. 2017;61(4):e02026–16 — Search PubMed
- Siddique AK, et al. "Why treatment centres failed to prevent cholera deaths among Rwandan refugees in Goma, Zaire." Lancet. 1995;345(8946):359–361. PMID: 7845126
- Ali M, et al. "Interpretation of the rapid dipstick test Crystal VC for Vibrio cholerae O1." J Clin Microbiol. 2006;44(4):1563–1564 — Search PubMed
- Raychoudhuri A, et al. "Clinical V. cholerae O1 in Kolkata in 2010: Antibiotic susceptibility, virulence genes and molecular subtypes." Indian J Med Res. 2013;137(5):867–872 — Search PubMed
- Okeke IN, et al. "Diagnostics as essential tools for containing antibacterial resistance." Drug Resist Updat. 2011;14(2):95–106 — Search PubMed
Connections
- All Bacteria
- Cholera Symptoms Overview
- Watery Diarrhea and Dehydration
- Cholera in Children and Vulnerable Groups
- Antibiotic Treatment and Resistance
- Cholera Treatment and Prevention
- Vibrio cholerae Overview
- Gastroenteritis
- Lab Tests
- Oral Rehydration and IV Fluids
- Cholera — full clinical overview of the disease being diagnosed.