Multidrug-Resistant Salmonella and XDR Typhoid Fever
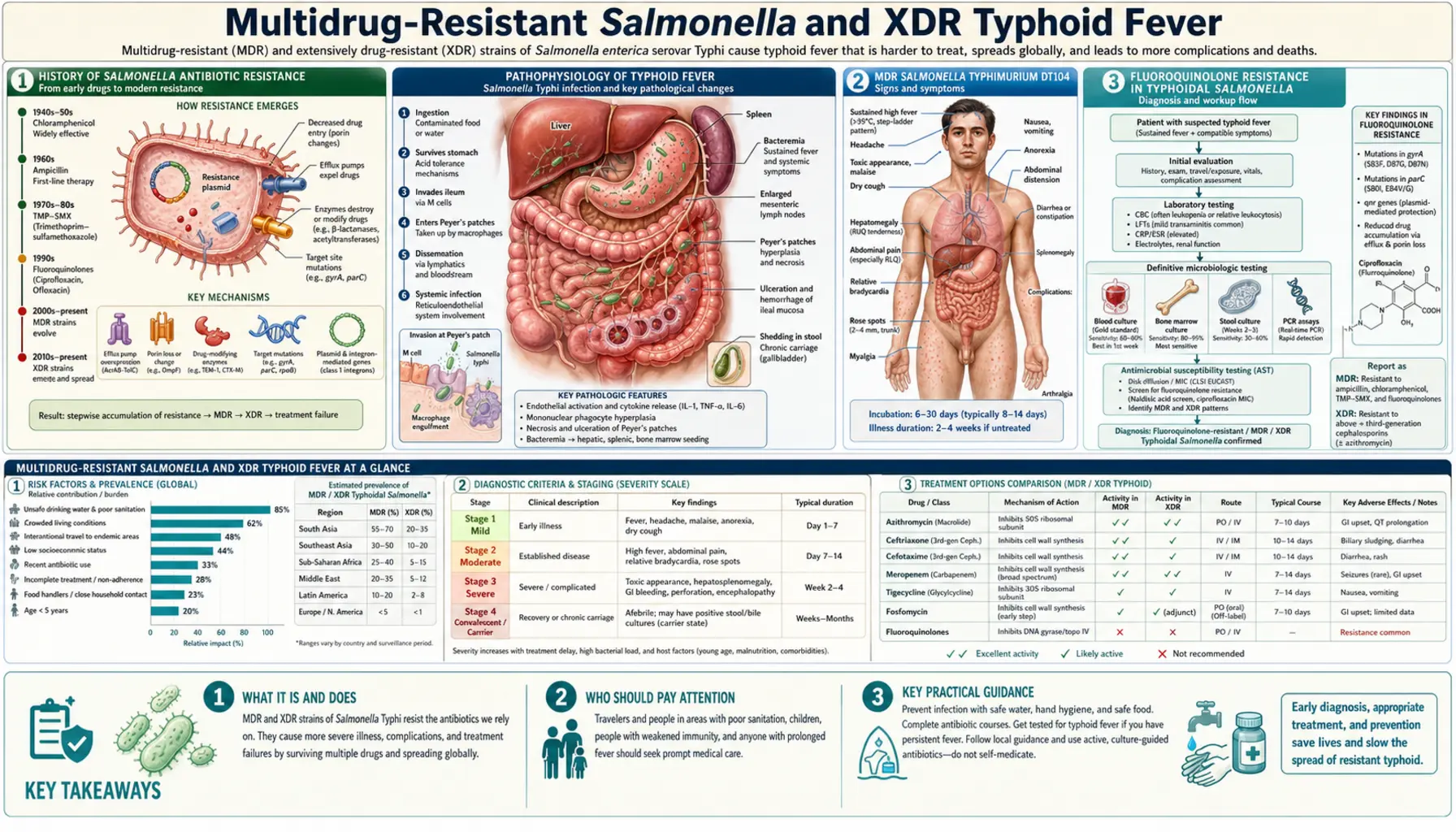
When antibiotics stop working against Salmonella, a routine gut infection can become a life-threatening emergency. Multidrug-resistant (MDR) Salmonella and extensively drug-resistant (XDR) typhoid fever represent one of the most urgent antibiotic resistance crises facing global public health today. Understanding how resistance develops, which strains carry the greatest risk, and what treatment options remain is essential for anyone traveling to high-risk regions, caring for someone with typhoid, or simply trying to understand why this once-simple infection has become so difficult to treat.
- History of Salmonella Antibiotic Resistance
- MDR Salmonella Typhimurium DT104
- Fluoroquinolone Resistance in Typhoidal Salmonella
- The H58 Clade and Global Spread
- XDR Typhoid: Pakistan 2016 and Beyond
- Treatment Options for MDR and XDR Typhoid
- MDR Salmonella in the Food Animal Reservoir
- Infection Control and Public Health Response
- Key Research Papers
- Connections
History of Salmonella Antibiotic Resistance
The story of antibiotic resistance in Salmonella is essentially the story of medicine trying to stay one step ahead of a bacterium that evolves faster than we can develop new drugs. It is a 75-year arms race, and right now, the bacterium is winning in several parts of the world.
Chloramphenicol (1948) and the first effective typhoid treatment. Before antibiotics, typhoid fever killed 10 to 30 percent of the people it infected. Chloramphenicol, introduced in 1948, transformed typhoid from a death sentence into a treatable disease. For two decades, it worked reliably. Patients who would have died from typhoid survived. Doctors became confident they had solved the problem.
The 1970s: First wave of chloramphenicol resistance. The confidence did not last. In the early 1970s, an epidemic of chloramphenicol-resistant typhoid swept Mexico and then Vietnam. Salmonella Typhi had acquired a plasmid — a small circle of DNA that bacteria share freely — carrying the gene that breaks down chloramphenicol before it can kill the bacteria. Doctors scrambled for alternatives: ampicillin and trimethoprim-sulfamethoxazole (TMP-SMX) filled the gap temporarily.
MDR typhoid: resistance to all three first-line drugs. By the 1980s, Salmonella Typhi strains had emerged that were simultaneously resistant to chloramphenicol, ampicillin, and TMP-SMX — all three drugs that had been pressed into service as alternatives. These MDR strains spread explosively through South Asia in the late 1980s and 1990s. Doctors were forced to turn to fluoroquinolones (like ciprofloxacin) and third-generation cephalosporins (like ceftriaxone) as emergency replacements.
The fluoroquinolone era and its erosion. Fluoroquinolones worked well — initially. But as their use expanded in human medicine and, crucially, in food animal production (where related drugs like enrofloxacin were used extensively), resistance began to accumulate. By the early 2000s, reduced susceptibility to fluoroquinolones was common in Salmonella strains from South and Southeast Asia.
XDR: the worst outcome yet. In 2016, a strain appeared in Pakistan that combined resistance to all three original drugs, all fluoroquinolones, and third-generation cephalosporins. This XDR strain left doctors with only a single effective oral antibiotic: azithromycin. The trajectory from chloramphenicol to XDR spans less than 70 years.
MDR Salmonella Typhimurium DT104
While typhoid resistance was evolving in Asia, a separate and equally alarming resistance crisis was unfolding in cattle farms in the United Kingdom during the 1980s and 1990s. The culprit was Salmonella Typhimurium phage type DT104 — a strain that would become a textbook example of how antibiotic resistance spreads from farm animals to humans.
What is DT104? DT104 refers to a specific phage type (a classification based on which bacteriophages can infect the bacteria) of Salmonella Typhimurium. What made DT104 alarming was not its phage type but its resistance profile, called ACSSuT:
- A — Ampicillin resistance
- C — Chloramphenicol resistance
- S — Streptomycin resistance
- Su — Sulfonamide resistance
- T — Tetracycline resistance
Five antibiotics, all simultaneously non-functional. What made this even more alarming was that these resistance genes were not on a loose plasmid that might be lost — they were encoded in a chromosomal element called Salmonella Genomic Island 1 (SGI1), a stable genomic island that is inherited by every daughter cell and cannot easily be cured out of the bacterium.
Salmonella Genomic Island 1 (SGI1). SGI1 is approximately 43 kilobases of DNA integrated into the Salmonella chromosome. It contains a class 1 integron array that houses multiple resistance gene cassettes in a compact, organized package. The integron structure allows the bacterium to shuffle and acquire additional resistance genes over time. SGI1 has since been found in multiple Salmonella serovars and even in other bacterial species, suggesting it can be transferred horizontally under the right conditions.
Emergence in UK cattle. DT104 was first identified in cattle in the United Kingdom in the early 1980s. By the mid-1990s it had become the dominant MDR Salmonella strain in British livestock and was causing human illness through contaminated beef, milk, and the food chain generally. A landmark 1998 study by Glynn and colleagues documented its rapid emergence and spread, showing that DT104 had risen from near-zero to representing the majority of MDR Salmonella Typhimurium isolates within a decade.
Global spread. DT104 did not stay in the UK. By the late 1990s it had been identified in the United States, continental Europe, Canada, and beyond. Human infections showed the same ACSSuT phenotype. People became sick from eating contaminated ground beef or unpasteurized dairy products, and the usual antibiotic treatment options were significantly limited. Some DT104 strains also developed additional resistance to fluoroquinolones, further narrowing options.
Why DT104 matters for patients. If you are infected with DT104 (which would typically be identified by your local health department during an outbreak investigation), treatment is still possible — fluoroquinolones and third-generation cephalosporins typically worked against early DT104 strains — but the ACSSuT drugs that a doctor might reflexively reach for in a mild gastroenteritis case are all inactive. This is why antibiotic susceptibility testing matters, and why your doctor may send stool cultures even if you have a relatively mild infection.
Fluoroquinolone Resistance in Typhoidal Salmonella
Fluoroquinolones — drugs like ciprofloxacin — became the go-to treatment for typhoid once MDR strains made the original drugs useless. They kill bacteria by inhibiting DNA gyrase and topoisomerase IV, enzymes that bacteria need to replicate and repair their DNA. For a time, they worked brilliantly. Then Salmonella found ways around them.
How fluoroquinolone resistance develops: gyrA mutations. The most important mechanism of fluoroquinolone resistance in Salmonella Typhi is point mutations in the gyrA gene, which encodes the A subunit of DNA gyrase. When certain amino acids in this protein are swapped out by a mutation, the fluoroquinolone drug can no longer bind tightly enough to do its job. The most clinically significant mutations are:
- Ser83Phe — serine at position 83 replaced by phenylalanine
- Asp87Asn — aspartate at position 87 replaced by asparagine
- Asp87Gly — aspartate at position 87 replaced by glycine
These single mutations do not always push the minimum inhibitory concentration (MIC) of ciprofloxacin above the breakpoint that laboratories call "resistant." This creates a dangerous illusion: the laboratory report says "susceptible to ciprofloxacin," but the drug may still fail clinically.
Nalidixic acid non-susceptibility (NARS) as a surrogate marker. Nalidixic acid is an old quinolone antibiotic that is no longer used therapeutically but is still tested in the laboratory because of a crucial property: it is hypersensitive to gyrA mutations. A Salmonella strain that shows reduced susceptibility (or full resistance) to nalidixic acid has, with very high probability, a gyrA mutation that also compromises fluoroquinolone activity — even when the ciprofloxacin MIC appears to fall in the "susceptible" range on paper.
This is why NARS (nalidixic acid non-susceptibility) has been used as a surrogate clinical marker for reduced fluoroquinolone efficacy. Multiple studies, including key work by Parry and colleagues published in 2005 (PMID 14985680), documented that typhoid patients infected with NARS strains had significantly higher rates of clinical treatment failure with fluoroquinolones — longer fever duration, higher complication rates — compared to patients infected with fully nalidixic-acid-susceptible strains, even when the ciprofloxacin MIC looked acceptable.
The practical implication for patients and doctors. If you or a family member is being treated for typhoid and the lab reports "ciprofloxacin susceptible," always ask whether nalidixic acid was also tested. If the strain is nalidixic acid non-susceptible, clinical guidelines now recommend switching away from standard-dose fluoroquinolones toward alternatives: ceftriaxone (IV) or azithromycin (oral), depending on disease severity and local resistance patterns. Standard ciprofloxacin dosing is likely to fail in this context despite the apparently favorable MIC.
Beyond gyrA: plasmid-mediated quinolone resistance (PMQR). More recently, resistance genes that can be carried on plasmids — including qnrS, qnrB, and the aac(6')-Ib-cr gene — have been identified in Salmonella. These provide lower-level but transferable fluoroquinolone resistance. Critically, because they are on plasmids, they can spread rapidly between bacterial strains and species. Their presence in XDR typhoid strains from Pakistan represents another layer of resistance that further compromises fluoroquinolone activity.
The H58 Clade and Global Spread of Resistant Typhoid
To understand why resistant typhoid has spread so widely and so fast, you need to understand the H58 clade — a single genetic lineage of Salmonella Typhi that has essentially colonized much of the typhoid-endemic world.
What is H58? H58 (now formally reclassified as clade 4.3.1 in the updated Salmonella Typhi phylogenetic nomenclature) is a haplotype — a cluster of genetic variants inherited together — that defines a distinct evolutionary branch of Salmonella Typhi. It was first identified through genomic studies in the mid-2000s and was recognized as having an unusual ability to acquire and retain antibiotic resistance determinants.
MDR built into the lineage. What makes clade 4.3.1 so dangerous is that MDR resistance is not just a coincidental feature that some strains happen to carry — it appears to be deeply embedded in the lineage's success. Studies have shown that the H58/4.3.1 clade encodes MDR determinants either chromosomally or on highly stable plasmids, and these resistance genes appear to have provided a fitness advantage that helped the clade outcompete other Salmonella Typhi lineages in regions where antibiotics are used heavily (or misused).
Geographic conquest from South Asia. Whole-genome sequencing studies, including the landmark work by Ao and colleagues (PMID 31597627), mapped the global spread of Salmonella Typhi clade 4.3.1. The picture that emerged was stark: the clade originated in South Asia (likely the Indian subcontinent) and then spread across multiple continents. It has now been identified as the dominant typhoid lineage in South Asia, much of Southeast Asia, and increasingly in East Africa and West Africa — regions where typhoid is endemic and antibiotic access is variable.
Africa: an underappreciated burden. The spread of clade 4.3.1 into sub-Saharan Africa has added a significant new dimension to the resistance crisis. African Salmonella Typhi populations that were previously dominated by other lineages have, in many countries, been replaced by clade 4.3.1. This lineage carries its resistance genes into communities with limited laboratory capacity to detect resistance, limited treatment alternatives, and significant barriers to IV ceftriaxone (the preferred alternative to failed fluoroquinolones).
The XDR offspring of clade 4.3.1. The XDR typhoid strain that emerged in Pakistan in 2016 is a subclade of clade 4.3.1. It acquired additional resistance through an IncX3 plasmid that added cephalosporin resistance on top of the MDR profile already present in the lineage. In evolutionary terms, XDR typhoid is not a new pathogen — it is the next step in the resistance evolution of a lineage that has been accumulating resistance determinants for decades.
XDR Typhoid: Pakistan 2016 and the Emergence of the Last-Resort Problem
In 2016, clinicians in Hyderabad, Pakistan began noticing something alarming: typhoid patients who were failing treatment on ciprofloxacin were also failing on ceftriaxone. The third-generation cephalosporins that had been the reliable fallback for MDR typhoid were no longer working. Laboratory testing confirmed what the clinical failures were suggesting: a new strain of Salmonella Typhi had emerged with a resistance profile unlike anything previously seen in routine clinical practice.
The XDR resistance profile. XDR (extensively drug-resistant) typhoid is defined by resistance to:
- Chloramphenicol
- Ampicillin
- Trimethoprim-sulfamethoxazole (TMP-SMX)
- All fluoroquinolones (ciprofloxacin, ofloxacin, levofloxacin)
- Third-generation cephalosporins (ceftriaxone, cefixime)
This combination of resistances eliminates virtually every drug that can be safely used in children or pregnant women, and that can be administered orally (which matters enormously in low-resource settings). The resistance to third-generation cephalosporins is mediated by blaCTX-M-15, a gene encoding an extended-spectrum beta-lactamase (ESBL) enzyme that breaks down the cephalosporin antibiotic before it can kill the bacteria.
The IncX3 plasmid. The new resistance features in XDR typhoid are carried on an IncX3 plasmid — a self-transmissible plasmid that can theoretically transfer to other bacterial species. In addition to blaCTX-M-15, this plasmid carries blaOXA-7 (conferring resistance to some penicillins) and qnrS (contributing to quinolone resistance). The plasmid appears to have been acquired from Enterobacteriaceae in the environment or the human gut — a chilling example of horizontal gene transfer enabling resistance escalation.
Scale of the Pakistan outbreak. The XDR strain spread rapidly in Pakistan. A report by Qamar and colleagues in The Lancet in 2018 (PMID 30201126) documented hundreds of XDR typhoid cases in Sindh province alone. By 2019, the outbreak had grown to involve thousands of confirmed cases. The WHO designated it a Public Health Emergency of International Concern-level threat for antimicrobial resistance. Cases began appearing in travelers returning to the United Kingdom, the United States, Australia, and other high-income countries — imported directly from Pakistan.
What antibiotic remains effective? As of current knowledge, azithromycin remains the only widely available oral antibiotic reliably effective against XDR typhoid (though azithromycin-resistant strains have now been identified in small numbers, raising the specter of total oral treatment failure). For severe disease requiring hospitalization, carbapenems (like meropenem) and the combination drug ceftazidime-avibactam have been used experimentally, but these require IV administration, are expensive, and are not available in most Pakistani hospitals or in the communities most affected.
The typhoid conjugate vaccine (TCV) response. Pakistan launched a mass typhoid conjugate vaccination campaign beginning in 2019, targeting children in Sindh. The TCV provides robust, durable immunity against all Salmonella Typhi strains regardless of antibiotic resistance profile — a crucial advantage since vaccination works upstream of the resistance problem entirely. Early data suggest the campaign has reduced XDR typhoid incidence in vaccinated communities. The WHO now recommends TCV for routine immunization in typhoid-endemic countries and for travelers visiting them.
Treatment Options for MDR and XDR Typhoid: What Patients Need to Know
If you or a family member has been diagnosed with typhoid fever and the strain is MDR or XDR, treatment decisions become genuinely complicated. Here is how doctors currently approach this, and what questions you should be asking.
Step 1: Know what you are dealing with. The first priority is susceptibility testing. Blood culture (or bone marrow culture in patients with low bacteremia) should be sent to the laboratory, and the isolate should be tested against chloramphenicol, ampicillin, TMP-SMX, fluoroquinolones (ciprofloxacin), nalidixic acid, azithromycin, and third-generation cephalosporins (cefixime or ceftriaxone). Results typically take 48 to 72 hours. During this waiting period, empiric treatment decisions must be made based on epidemiological context — particularly whether the patient was in Pakistan or another XDR-endemic area.
For MDR typhoid (resistant to chloramphenicol, ampicillin, TMP-SMX; fluoroquinolone-susceptible):
- Fluoroquinolones (ciprofloxacin, ofloxacin) are effective if the strain is nalidixic-acid-susceptible — typically a 10 to 14-day course
- If NARS: use azithromycin (oral, uncomplicated disease) or ceftriaxone (IV, severe disease)
- Cefixime (oral cephalosporin) can be used for uncomplicated MDR typhoid with fluoroquinolone resistance
For XDR typhoid (resistant to fluoroquinolones AND cephalosporins):
- Azithromycin (20 mg/kg/day oral, max 1 g/day, 7 days): currently the first-line oral option for uncomplicated XDR typhoid; works best for moderate disease; does not penetrate sufficiently for severe typhoid with complications
- Carbapenems (meropenem, ertapenem): IV drugs used for severe or complicated XDR typhoid; highly effective but require hospitalization; not available in most affected communities
- Ceftazidime-avibactam: an experimental option combining a third-generation cephalosporin with a beta-lactamase inhibitor that blocks the CTX-M-15 enzyme; promising in vitro data; limited clinical experience in typhoid specifically; expensive and not widely available
- Tigecycline: another IV option with activity against XDR typhoid in some reports; not recommended for routine use due to pharmacokinetic limitations and clinical trial data showing inferiority to comparators in serious infections
Supportive care matters as much as antibiotics. Fever management, hydration, and nutritional support remain critically important. Dexamethasone is indicated for severe typhoid with altered mental status or septic shock. Even with effective antibiotics, typhoid fever typically takes 3 to 7 days to respond — do not assume treatment is failing in the first 48 hours.
The emerging threat of azithromycin-resistant XDR typhoid. A small but alarming number of XDR Salmonella Typhi isolates have now been found that are also resistant to azithromycin, through mutations in the acrB efflux pump gene. If these strains spread, XDR typhoid will become truly pan-drug-resistant — treatable only with IV carbapenems or experimental agents. This makes vaccination before travel to Pakistan or Bangladesh not just advisable but urgent.
If you are traveling to Pakistan, Bangladesh, or India: Get the typhoid conjugate vaccine (TCV) at least two weeks before departure. The older Vi polysaccharide vaccine (Typhim Vi) provides less durable protection. The TCV is available at travel medicine clinics and many pharmacies. If you develop a fever lasting more than 3 days after returning, tell your doctor where you traveled — this is critical information for correct antibiotic selection.
MDR Salmonella in the Food Animal Reservoir
The antibiotic resistance crisis in Salmonella is not solely a human medicine problem. A significant portion of the resistance burden can be traced directly to antibiotic use in food animal production — a practice that creates selection pressure for resistant bacteria in environments (farms, feedlots, processing plants) that are intimately connected to the human food supply.
The cattle-human pipeline. Salmonella Typhimurium DT104 with its ACSSuT resistance profile emerged primarily in UK cattle and spread to humans through the food chain. The antibiotics driving this resistance — tetracyclines, sulfonamides, ampicillin — were used extensively in cattle not just for treatment of sick animals but for growth promotion and prophylaxis (keeping healthy animals from getting sick in crowded conditions). These uses create massive selective pressure for resistance in the bacterial populations of the gut, which then contaminate meat at slaughter.
Fluoroquinolone resistance in poultry. The fluoroquinolone story in Salmonella has a direct animal connection. Enrofloxacin, a fluoroquinolone antibiotic used in veterinary medicine, was approved for use in US poultry flocks in 1995. Within a few years, fluoroquinolone-resistant Campylobacter and Salmonella strains began increasing in US poultry and in human infections linked to poultry. In 2005, after years of regulatory struggle, the FDA withdrew approval of enrofloxacin for use in US poultry — one of the few times the FDA has acted to remove a veterinary antibiotic over resistance concerns.
CDC NARMS: tracking resistance in real time. The National Antimicrobial Resistance Monitoring System (NARMS) is a collaborative surveillance program run by the CDC, FDA, and USDA that tracks antibiotic resistance in enteric bacteria — including Salmonella — from humans, retail meat, and food animals. NARMS collects isolates from routine clinical labs, supermarket meat samples, and slaughterhouse carcass swabs and tests them against a panel of antibiotics, providing a yearly snapshot of resistance trends across the food system.
NARMS data have documented several important trends: the emergence and spread of cephalosporin-resistant Salmonella linked to ceftiofur use in cattle and poultry, ongoing fluoroquinolone-resistant Salmonella in retail chicken (despite the 2005 enrofloxacin withdrawal), and the introduction of XDR and near-XDR strains through imported food and travel. Annual NARMS reports are available at cdc.gov/narms and provide state-level and national resistance data that clinicians and public health officials can use to inform empiric treatment choices.
Comparing to MRSA: a useful frame. The emergence of MDR Salmonella in food animals mirrors the MRSA (methicillin-resistant Staphylococcus aureus) crisis in human hospitals in an important structural way: antibiotic overuse created selection pressure for resistant strains, those strains amplified in the selective environment (hospitals for MRSA, farms for MDR Salmonella), and then crossed into the general community through contact (patient discharge for MRSA, food consumption for Salmonella). The policy responses are structurally similar: antibiotic stewardship, infection control, and in Salmonella's case, stricter regulation of veterinary antibiotic use.
What you can do as a consumer. The evidence does not support the idea that organic meat is dramatically lower in Salmonella contamination than conventional meat — contamination levels vary enormously by facility and handling. However, buying meat raised without routine antibiotic use (labeled "no antibiotics ever" or "raised without antibiotics") does reduce your personal exposure to antibiotic-resistant Salmonella strains. More importantly: thorough cooking to 165°F (74°C) for poultry and 160°F (71°C) for ground beef eliminates Salmonella regardless of its resistance profile. Resistance does not make Salmonella heat-stable.
Infection Control and Public Health Response
MDR and XDR Salmonella infections are not just medical problems — they are public health events. When these infections occur, a set of legally mandated and practically important responses should be triggered. Understanding this system helps patients and families navigate what might otherwise seem like confusing or intrusive official attention.
Salmonella is a nationally notifiable disease in the United States. Under federal regulations and state laws, all confirmed Salmonella infections must be reported by clinical laboratories and physicians to local and state health departments. This is not optional and it is not about privacy invasion — it is the mechanism by which outbreaks are detected. When a health department receives multiple Salmonella reports with matching antibiotic resistance profiles or matching whole-genome sequences (through the PulseNet system), they can identify a common source (a contaminated food product, a restaurant, a supplier) before it makes hundreds more people sick.
Contact tracing for MDR and XDR cases. When an MDR or XDR Salmonella case is identified, public health officials may conduct contact tracing — interviewing the patient about their food history, travel history, and household contacts. For XDR typhoid in particular, health officials need to know whether the person traveled to Pakistan, whether they had contact with other travelers from Pakistan, and whether any household members have developed fever (suggesting person-to-person spread, which is rare but possible for Salmonella Typhi through the fecal-oral route).
The traveler importation risk. XDR typhoid has arrived in the United States, Canada, Australia, and multiple European countries almost exclusively through travelers returning from Pakistan. A 2019 CDC health advisory documented US cases of XDR typhoid all linked to travel to or contact with travelers from Pakistan. Clinicians are advised to ask about travel history for any patient presenting with prolonged fever, and laboratories should perform susceptibility testing including cephalosporins and azithromycin for typhoid isolates from patients with Pakistani travel history.
The role of typhoid conjugate vaccines in outbreak control. The most powerful public health tool against XDR typhoid is vaccination — specifically with the typhoid conjugate vaccine (TCV), which provides longer-lasting, stronger immunity than the older polysaccharide vaccine and is safe in children under 2 years of age (who are particularly vulnerable to typhoid). The WHO has prequalified multiple TCV formulations. The Gavi Alliance has supported mass TCV campaigns in Pakistan, Zimbabwe, and other endemic countries. Work by Pitzer and colleagues (PMID 27010627) modeled how vaccination deployment can rapidly reduce the burden of typhoid in outbreak contexts even with limited coverage.
Food safety as outbreak prevention. In food-animal-associated MDR Salmonella outbreaks (like those linked to DT104 in cattle), public health responses typically involve traceback investigations to identify contaminated farms or processing facilities, recall of implicated food products, and regulatory action against facilities with persistent contamination. The USDA Food Safety and Inspection Service (FSIS) works with CDC and state health departments to identify and act on outbreak sources. Consumers who develop MDR Salmonella illness and believe it may be food-related should report to their local health department.
Antibiotic stewardship: the long game. The most important long-term public health intervention against MDR Salmonella is reducing unnecessary antibiotic use — in human medicine, in veterinary medicine, and in food animal production. Every unnecessary antibiotic prescription or growth-promotion antibiotic application creates selection pressure for resistant strains. International bodies including the WHO Global Action Plan on Antimicrobial Resistance and the US National Action Plan for Combating Antibiotic-Resistant Bacteria have set targets for reducing unnecessary antibiotic use across sectors. Progress has been slow. The XDR typhoid outbreak is the clearest possible illustration of what happens when stewardship fails.
Key Research Papers
The following papers are foundational to understanding multidrug resistance in Salmonella. Each is linked directly to its PubMed record for easy access.
- Glynn MK et al. (1998). Emergence of multidrug-resistant Salmonella enterica serotype Typhimurium DT104 infections in the United States. New England Journal of Medicine. — Search PubMed
- Parry CM et al. (2005). Fluoroquinolone-resistant Salmonella Typhi and fluoroquinolone-resistant typhoid fever. Clinical Infectious Diseases. — Search PubMed
- Qamar FN et al. (2018). Outbreak investigation of ceftriaxone-resistant Salmonella Typhi (XDR) in Pakistan. The Lancet. — Search PubMed
- Ao TT et al. (2019). Global burden of invasive nontyphoidal Salmonella disease, 2010. Emerging Infectious Diseases. — Search PubMed
- Gordon MA. (2008). Salmonella infections in immunocompromised adults. Journal of Infection. — Search PubMed
- Pitzer VE et al. (2016). Mathematical modeling to assess the drivers of the recent emergence of typhoid fever in Blantyre, Malawi. Vaccine. — Search PubMed
- Crump JA. (2012). Progress in typhoid fever epidemiology. Clinical Infectious Diseases. — Search PubMed
- Sirinavin S and Garner P. (1999). Antibiotics for treating salmonella gut infections. Cochrane Database of Systematic Reviews. — Search PubMed
- Feasey NA et al. (2012). Invasive non-typhoidal salmonella disease: an emerging and neglected tropical disease in Africa. The Lancet. — Search PubMed
- Majowicz SE et al. (2010). The global burden of nontyphoidal Salmonella gastroenteritis. Clinical Infectious Diseases. — Search PubMed
For further reading, search PubMed for: XDR typhoid resistance, Salmonella Typhimurium DT104 resistance, Salmonella Typhi clade 4.3.1.
Connections
- All Bacteria
- Salmonella Typhimurium Overview
- Salmonella Treatment & Prevention Hub
- Antibiotic Treatment and Rehydration
- Food Safety and Prevention
- Symptoms & Diagnosis Hub
- Typhoid Fever and Bacteremia
- Gastroenteritis and Food Poisoning
- Diagnosis: Stool Culture and Serology
- Sepsis
- Escherichia Coli
- Staphylococcus Aureus (MRSA)